Journal list menu

 Issue
IssueANZ Journal of Surgery: Volume 94, Issue 6
980-1193June 2024
Export Citations
Download PDFs
ISSUE INFORMATION
EDITORIAL
Cutting carbon out of surgical care delivery
- Pages: 984-985
- First Published: 18 June 2024
PERSPECTIVES
Changes and challenges in health technology assessment
- Pages: 986-988
- First Published: 13 May 2024
Augmented prehabilitation – is there a role for glucocorticoids and/or anabolic steroids to improve surgical outcomes?
- Pages: 989-992
- First Published: 25 March 2024
The good, the bad, and the frail – the role of prehabilitation in frail patients undergoing cancer surgery
- Pages: 993-995
- First Published: 08 May 2024
Chimeric antigen receptor T cell immunotherapy in colorectal cancer: primetime yet?
- Pages: 996-997
- First Published: 31 March 2024
SPECIAL ARTICLE
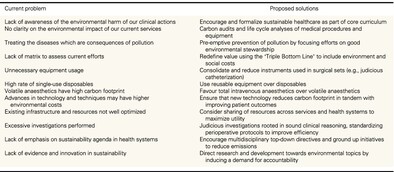
How we can reduce the environmental impact of our operating theatres: a narrative review
- Pages: 1000-1010
- First Published: 20 November 2023
This narrative review encompasses a broad approach to different changes that can be made to improve the environmental sustainability in operating theatres. The review may be used by individual institutions to suggest changes, or be a resource for the development of future policies for surgical sustainability.
REVIEW ARTICLES
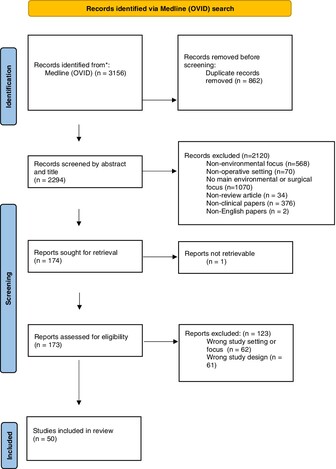
A guide to outcome evaluation of simulation-based education programmes in low and middle-income countries
- Pages: 1011-1020
- First Published: 30 March 2024
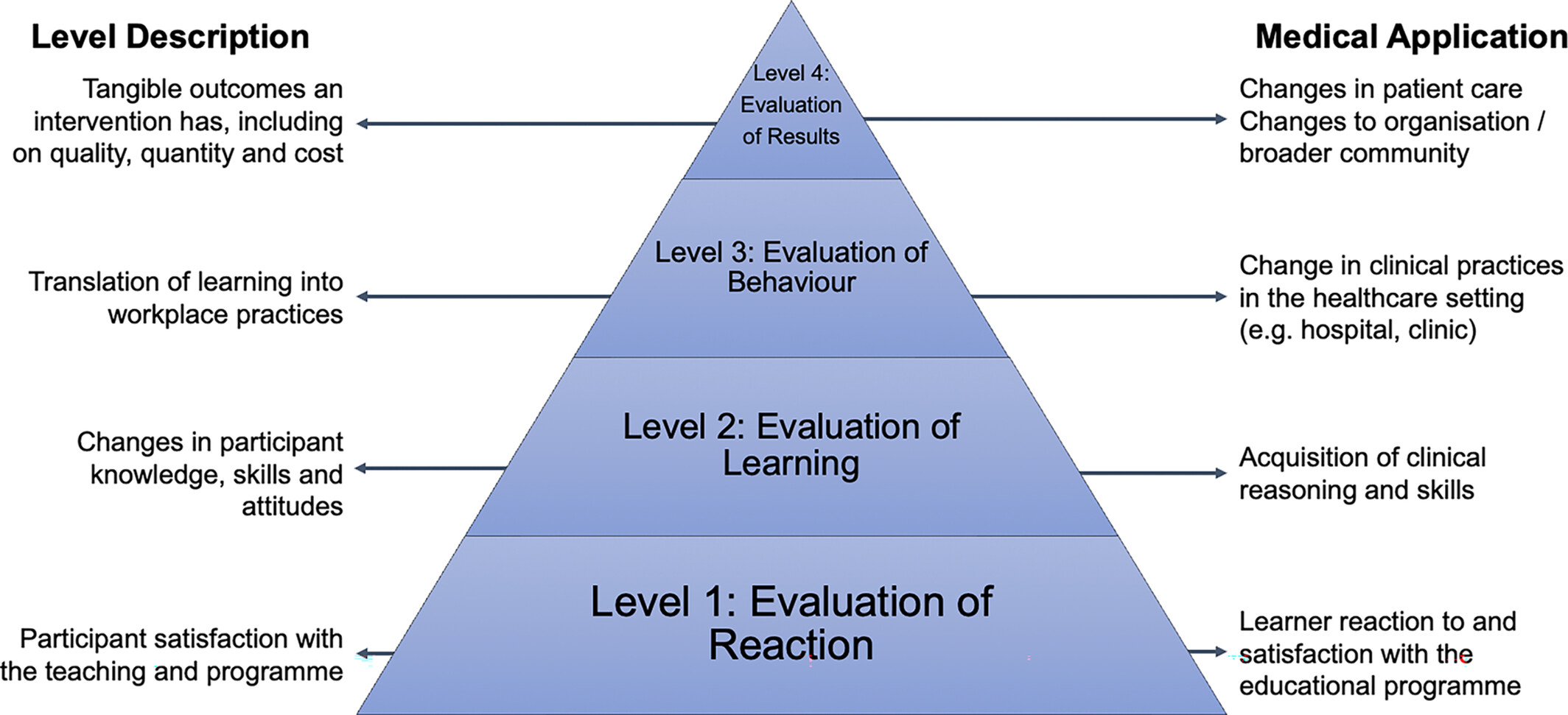
Evaluation is a vital part of any learning activity and is essential to optimise and improve educational programmes. This review provides a framework for conducting outcome evaluation of simulation-based educational programmes in low- and middle-income countries through the lens of a successful surgical simulation programme in Myanmar. It includes a discussion of evaluation theory and methods, grounded in a practical application, to enable other educators in low-resource settings to evaluate their own activities.
Effects of glossopharyngeal nerve block on pain control after tonsillectomy: a systemic review and meta-analysis
- Pages: 1021-1029
- First Published: 30 March 2024
We compared perioperative glossopharyngeal nerve block to placebo or normal saline group in terms of postoperative pain, analgesic use, nausea, vomiting, and emergence agitation. Postoperative pain reduction was observed in treatment groups after 1–4 and 5–8 h, but glossopharyngeal nerve block did not significantly reduce pain or analgesic drug use after 12 h. Intraoral glossopharyngeal nerve block for tonsillectomy did not reduce postoperative pain compared to control group.
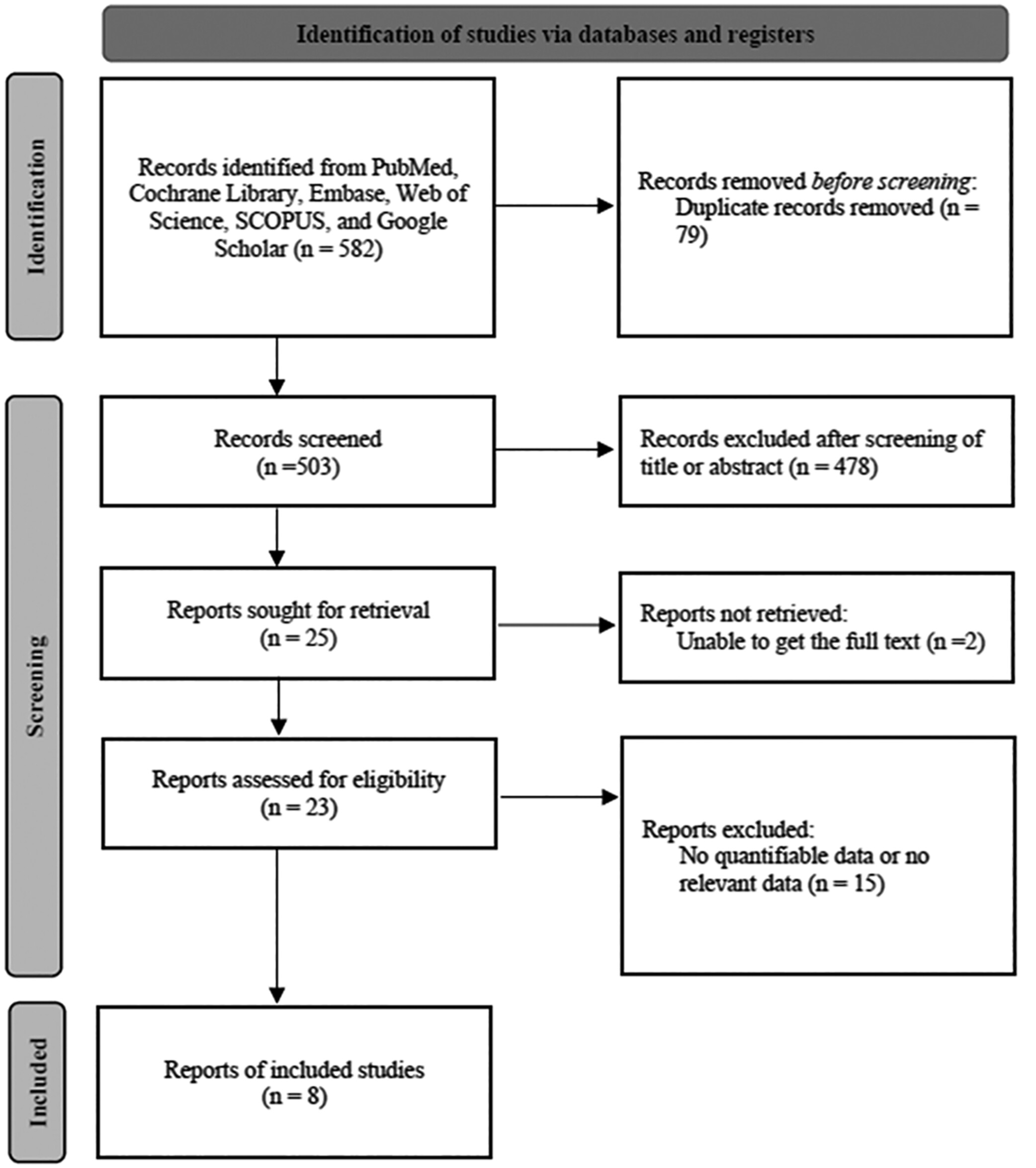
Association of preoperative CT-scan features and clinically relevant postoperative pancreatic fistula after pancreaticoduodenectomy: a meta-analysis
- Pages: 1030-1038
- First Published: 05 June 2024
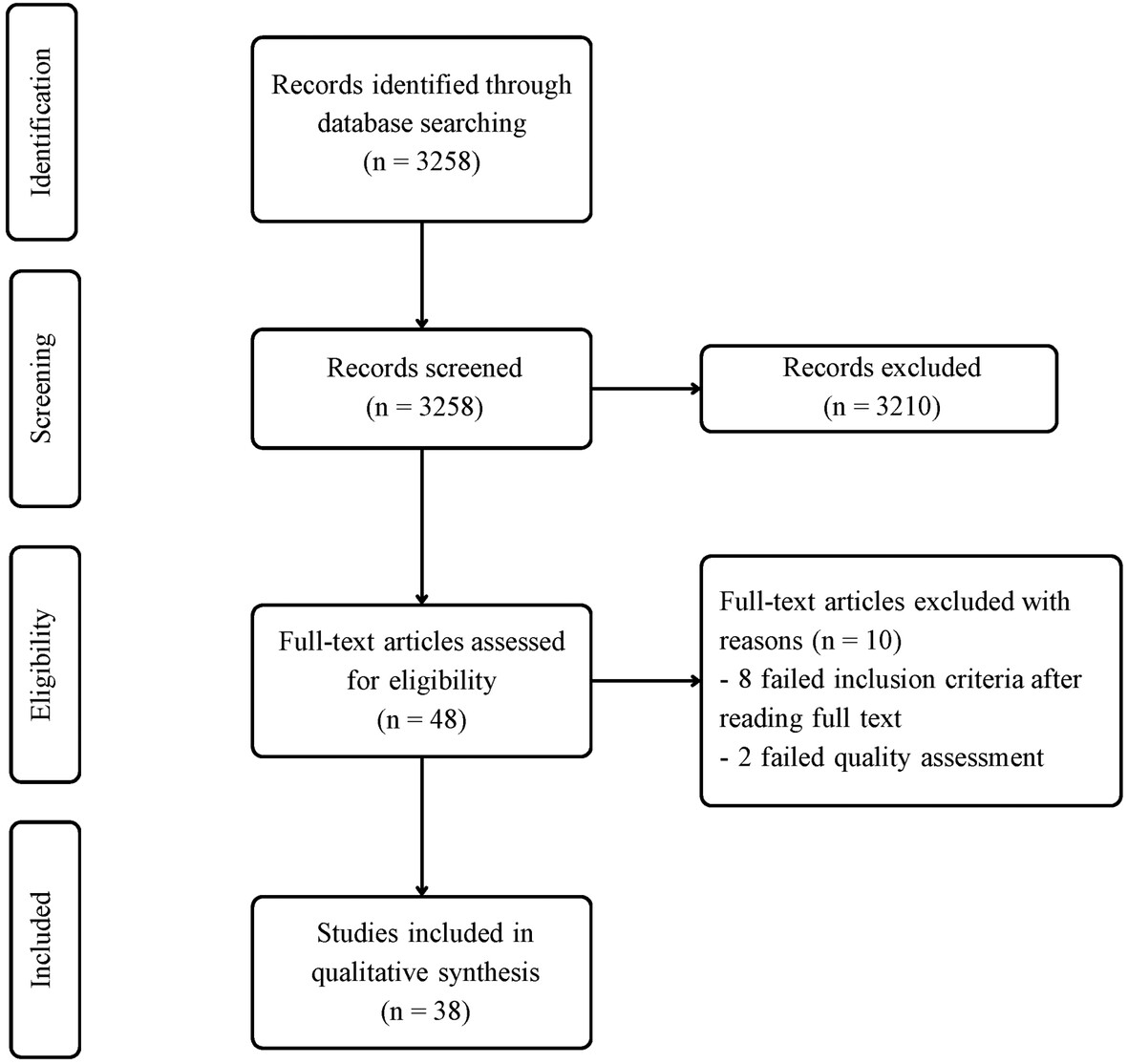
This systematic review and meta-analysis of 38 studies found that smaller pancreatic duct diameter (PDD) and decreased pancreatic parenchymal thickness (PPT) on preoperative CT scans are significant predictors of clinically relevant postoperative pancreatic fistula (CR-POPF) after pancreaticoduodenectomy. Age also correlates with an increased risk of this complication.
SURGICAL EDUCATION AND TRAINING
Review of Māori equity in surgical trainee selection
- Pages: 1039-1044
- First Published: 17 February 2024

The Royal Australasian College of Surgeons (RACS) aims to achieve Māori health equity and cultural safety within the surgical workforce. The RACS Māori Health Strategy and Action Plans encourage research utilizing Kaupapa Māori (KM) methodology and Surgical Education and Training (SET) selection criteria that recognizes and credits applicants who identify as Māori or demonstrate competence in Māori health issues. Unfortunately, the SET selection criteria for some specialties fail to recognize or credit Māori identification and cultural competency.
The impact of COVID-19 on general surgical trainees' surgical exposure in Australia
- Pages: 1045-1050
- First Published: 30 January 2024
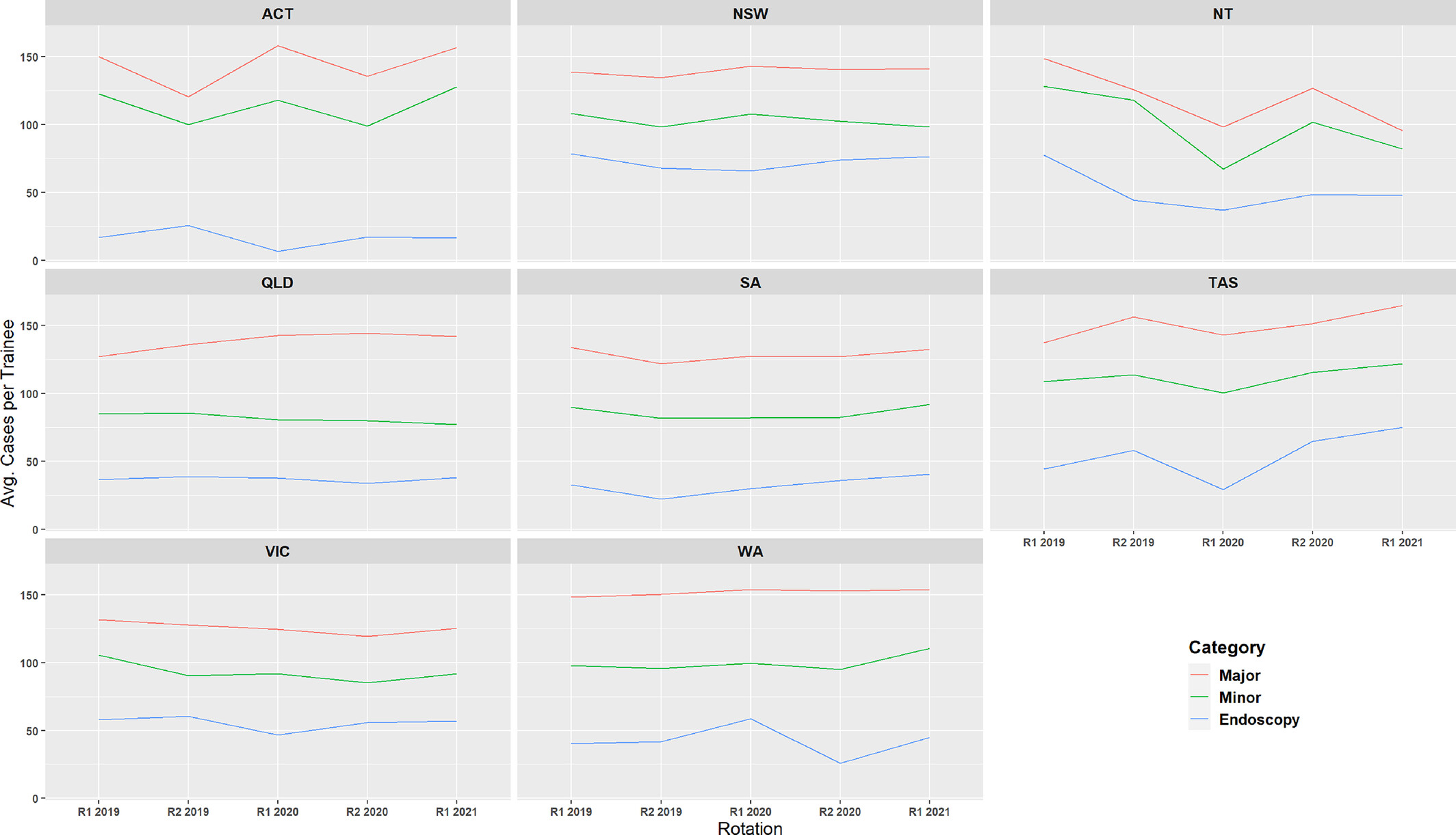
The impact of COVID-19 on surgical trainees globally has been significant. This data demonstrates that AGST have been relatively spared from significant impacts of the pandemic on their operative exposure or autonomy. Although this study does not assess other important aspects of surgical training that may have been affected by the pandemic, it supports trainees who have progressed adequately through the pandemic to avoid unnecessary extensions to their training.
Can open cholecystectomy be taught by cadaveric simulation?
- Pages: 1051-1055
- First Published: 08 May 2024
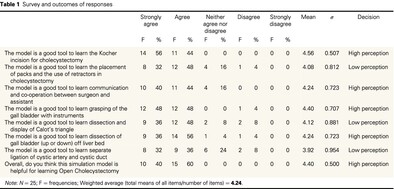
Laparoscopic cholecystectomy is the current standard of treatment for surgical gallbladder removal as it has an overall improved post-operative recovery compared to open. This has resulted in the loss of exposure to surgical trainees and the associated technical skills and decision-making required to convert to open cholecystectomy. The aim of this study is to provide construct validity to the proposition that cadaveric simulation can be used successfully to teach and learn open cholecystectomy.
Novel, intermediate-fidelity simulator for aortic arch surgery for the cardiothoracic surgical trainee
- Pages: 1056-1058
- First Published: 30 January 2024

Training cardiothoracic surgeons in open aortic surgery is challenging due to the complexity of technical skills and limited operator experience. The study reports on a reproducible, intermediate-fidelity simulator for aortic surgery.
CARDIOTHORACIC SURGERY
Healthcare sustainability in cardiothoracic surgery
- Pages: 1059-1064
- First Published: 12 February 2024
Cardiothoracic surgery should champion sustainability in healthcare as our patients have most to gain from improving enviromental sustainability.
Coronary artery bypass grafting in octogenarians: an Australian experience
- Pages: 1065-1070
- First Published: 15 February 2024
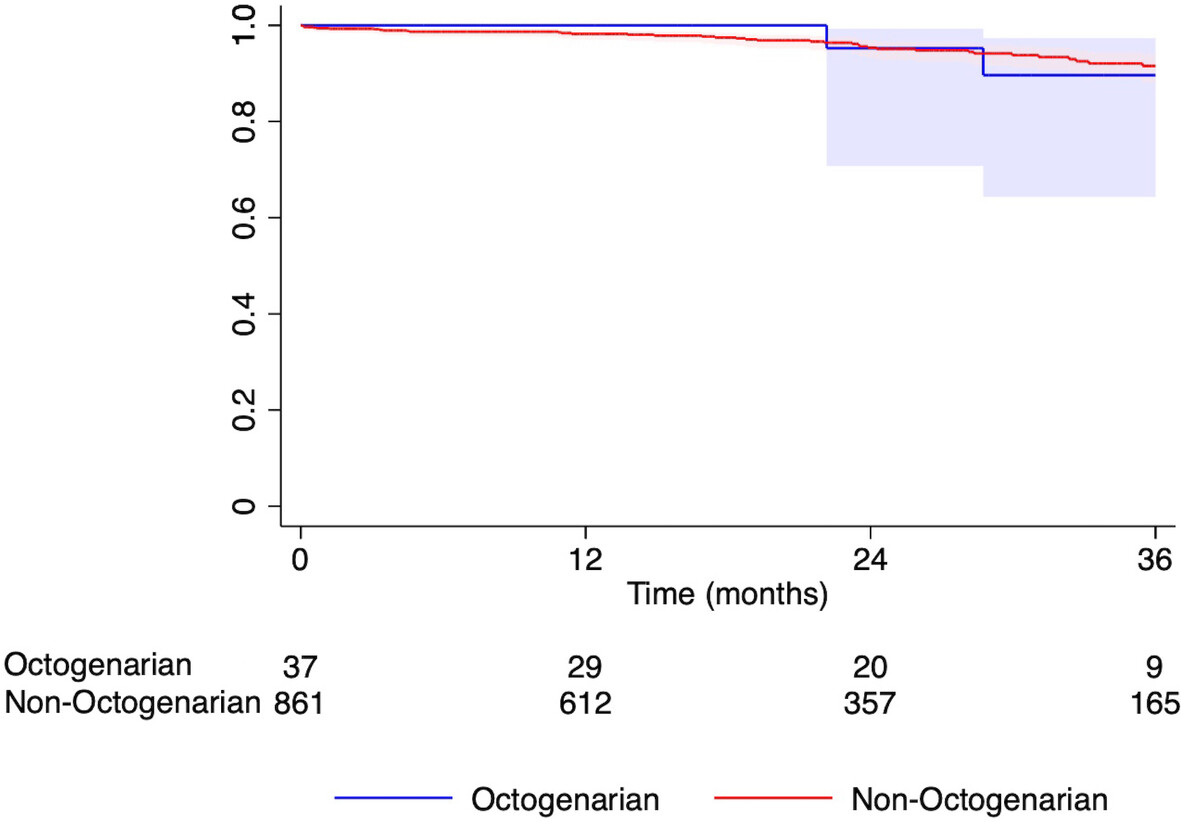
The aims of this study were to describe early and mid-term morbidity and mortality in octogenarian patients undergoing CABG, to determine if outcomes are comparable to younger patients undergoing the same procedure. Despite an increase in post-operative morbidity and LOS, there was no difference in hospital readmission, in-hospital mortality or 1 year mortality in octogenarian patients who underwent CABG. CABG is safe and remains an important management option for these patients.
UROLOGY
Nurse-led renal cell carcinoma clinic: a single center review
- Pages: 1071-1075
- First Published: 01 March 2024
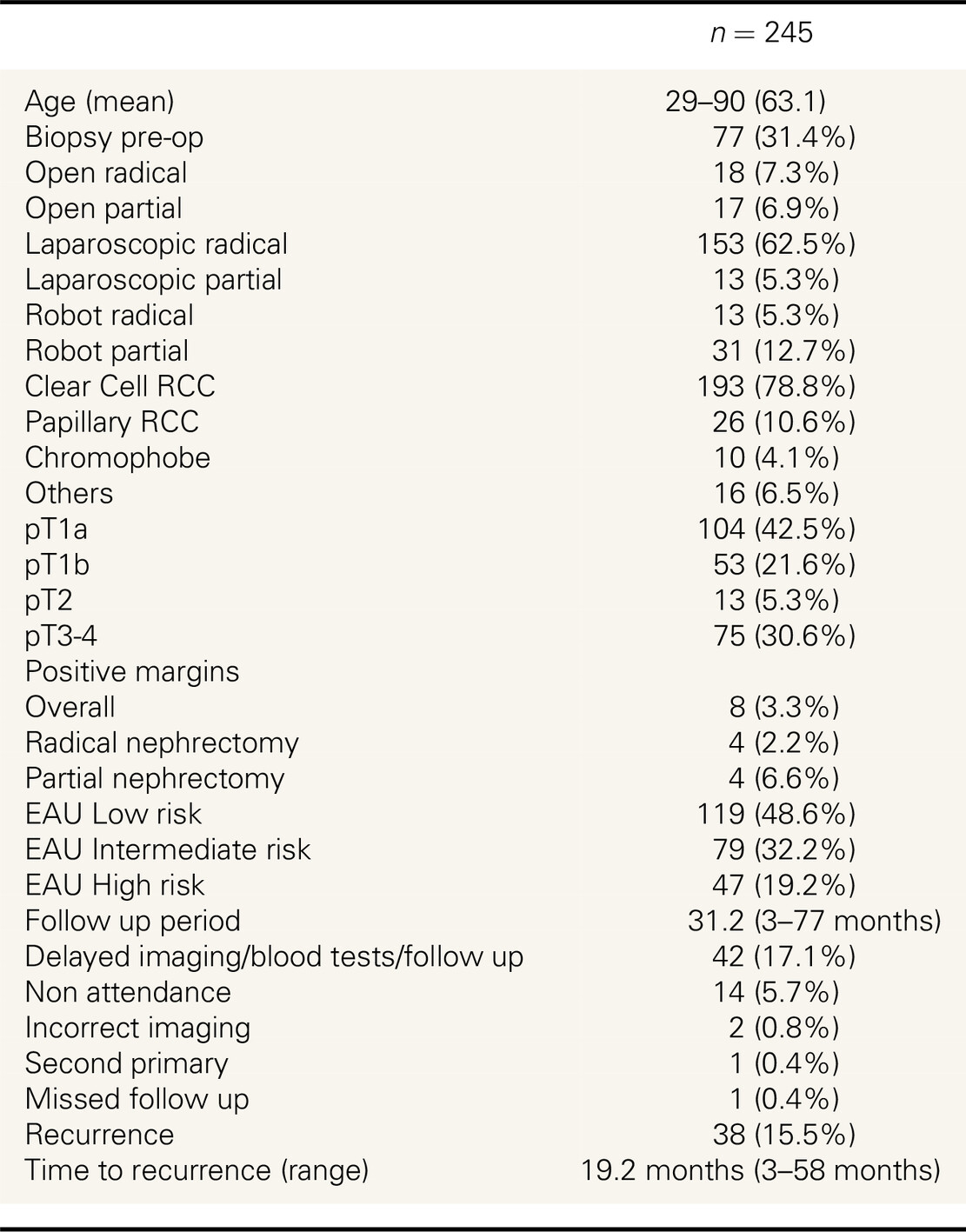
Nurse-led renal cell cancer follow up is a safe, reliable and effective clinical framework that has significant benefits in regard to resource utilization. USS and CXR are ineffective in detecting recurrence and CT should be considered the imaging modality of choice for this purpose.
Expanding urological services into regional Australia and reducing interhospital transfers: how the nurse practitioner can help
- Pages: 1076-1082
- First Published: 15 April 2024
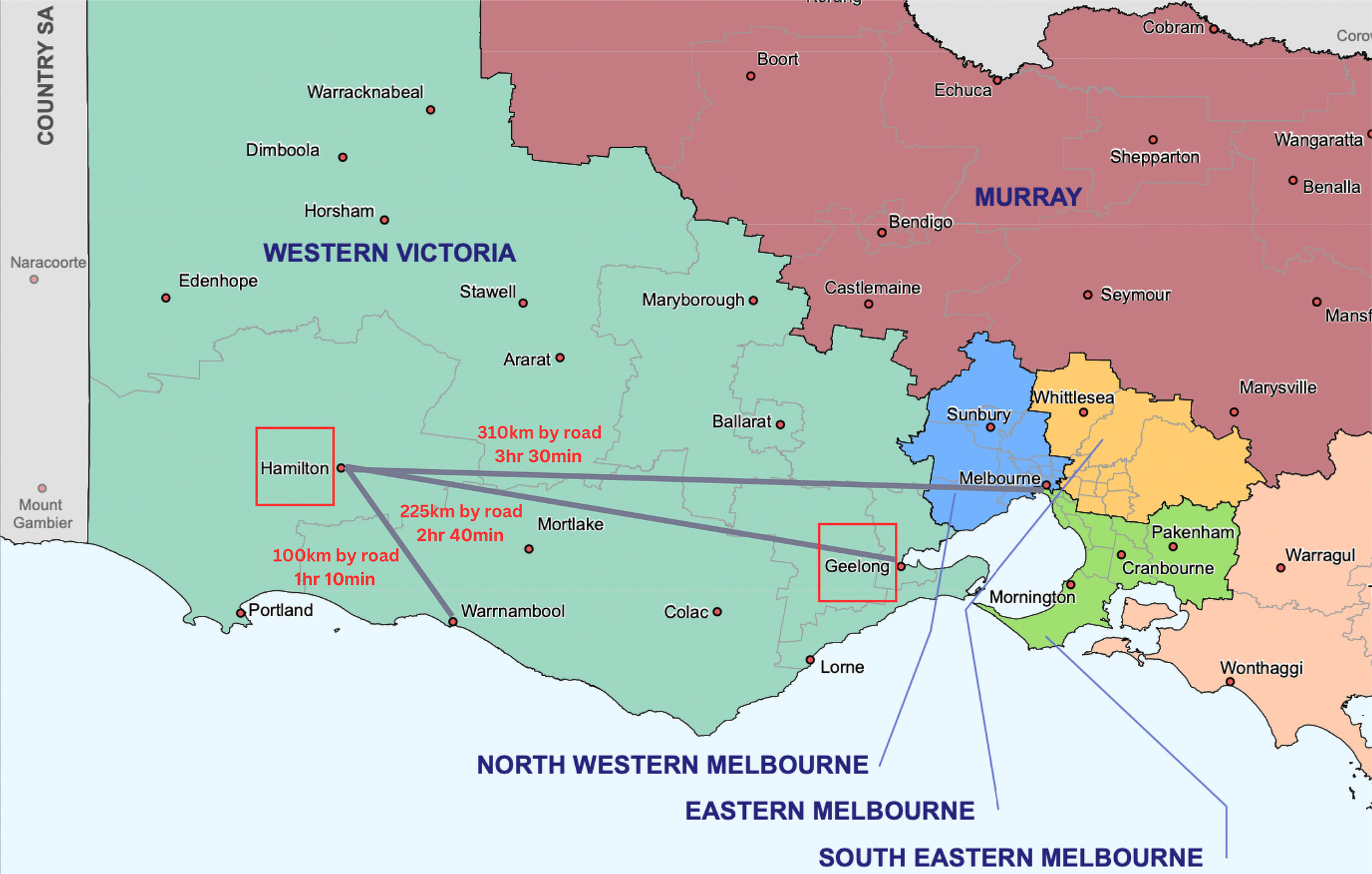
A visiting urology service has been in existence at Hamilton Base Hospital, Western Victoria, over the past 25 years, serving an unmet need. We aim to assess the impact of the UNP's role in the delivery of regional urological care. Transferring an acute patient from a regional to a tertiary hospital for specialist care is often necessary but not ideal for the patient and their family. The presence of a dedicated UNP in a regional centre is important for patient care and has an important role in preventing unnecessary transfers. This is a vital component of a visiting urological service to a rural community.
BREAST SURGERY
Radar localization of breast and axillary lesions with SCOUT: a prospective single institution pilot study
- Pages: 1083-1089
- First Published: 13 May 2024
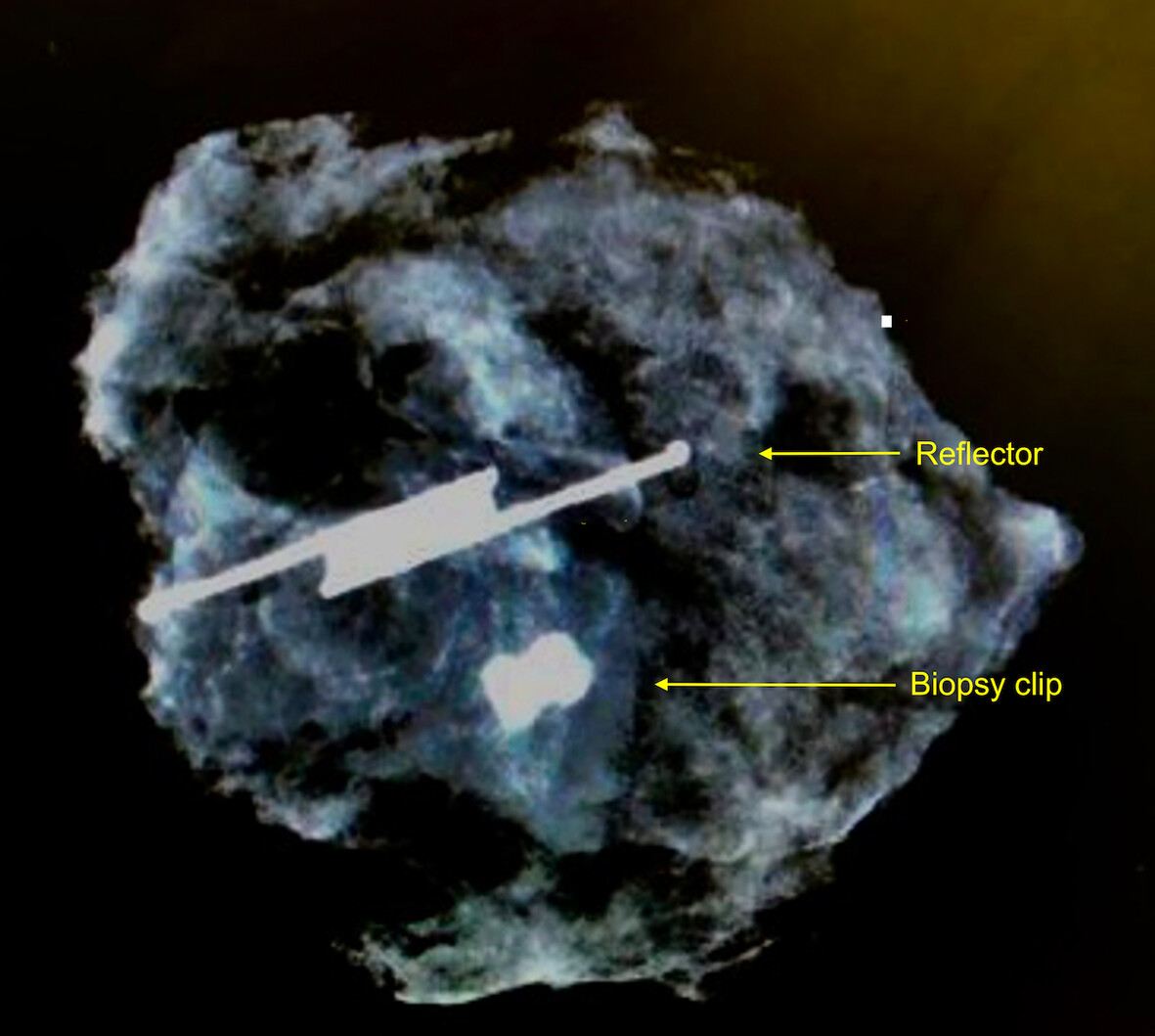
SCOUT® is a non-radioactive wireless localization technology. It was an accurate and reliable method to localize and excise both breast and axillary lesions. In most cases the surgeon was satisfied with ease of localization.
Avoiding unnecessary sentinel lymph node biopsy with the use of superparamagnetic iron oxide mapping agents (Magtrace®) in breast surgery
- Pages: 1090-1095
- First Published: 08 March 2024

Superparamagnetic iron oxide (SPIO) (Magtrace®) is a liquid tracer that can stay in the sentinel lymph nodes for 30-days. This is a retrospective study that assesses the use of SPIO at time of primary breast surgery where upfront sentinel lymph node biopsy is not immediately indicated, such as in surgery for non-invasive disease and prophylactic breast surgery. SPIO then allows a delayed sentinel lymph node biopsy to be performed if pathology then identifies invasive disease.
Enhanced recovery after surgery for oncological breast surgery reduces length of stay in a resource limited setting
- Pages: 1096-1101
- First Published: 15 March 2024
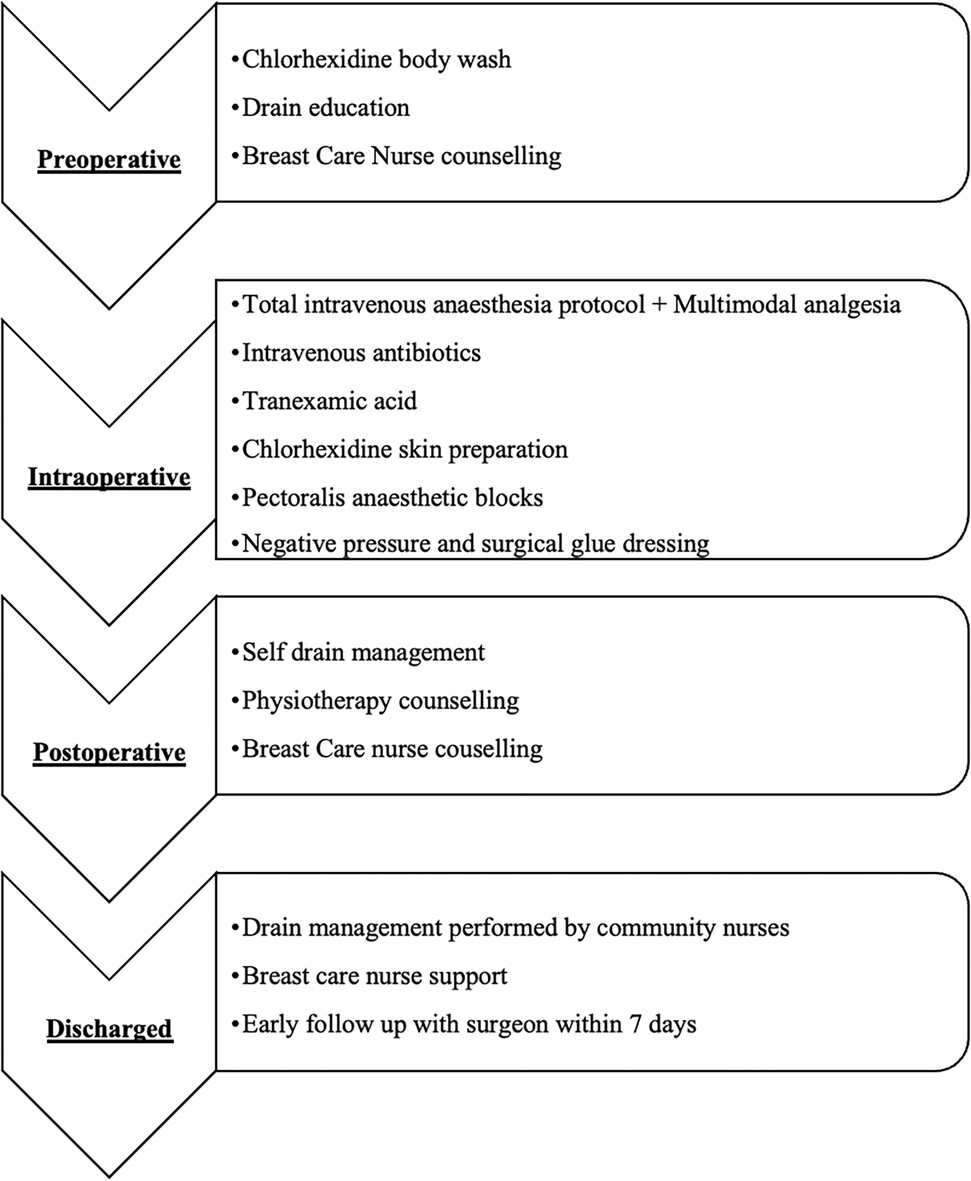
Our enhanced recovery after surgery protocol has reduced the length of stay in patients undergoing oncological breast surgery from 2.26 to 1.42 days.
HEPATOPANCREATICOBILIARY SURGERY
Searching for low phospholipid associated cholelithiasis among patients with post-cholecystectomy biliary pain
- Pages: 1102-1107
- First Published: 15 February 2024

Low phospholipid associated cholelithiasis is present in 1% of patients with gallstones and post-cholecystectomy pain but is an under recognized. In an audit of 258 patients undergoing a cholecystectomy under the age of 40, 1.9% of patients fulfilled the criteria for LPAC and no patients had the diagnosis of LPAC considered by their treating clinicians.
External validation of the CholeS conversion from laparoscopic to open cholecystectomy (CLOC) risk score in Aotearoa New Zealand: a validation study
- Pages: 1108-1113
- First Published: 25 March 2024
The CLOC score performs suboptimally in the Aotearoa New Zealand setting to predict conversion of laparoscopic cholecystectomy to open.
3D visualization systems improve operator efficiency during difficult laparoscopic cholecystectomy: a retrospective blinded review of surgical videos
- Pages: 1114-1121
- First Published: 14 March 2024
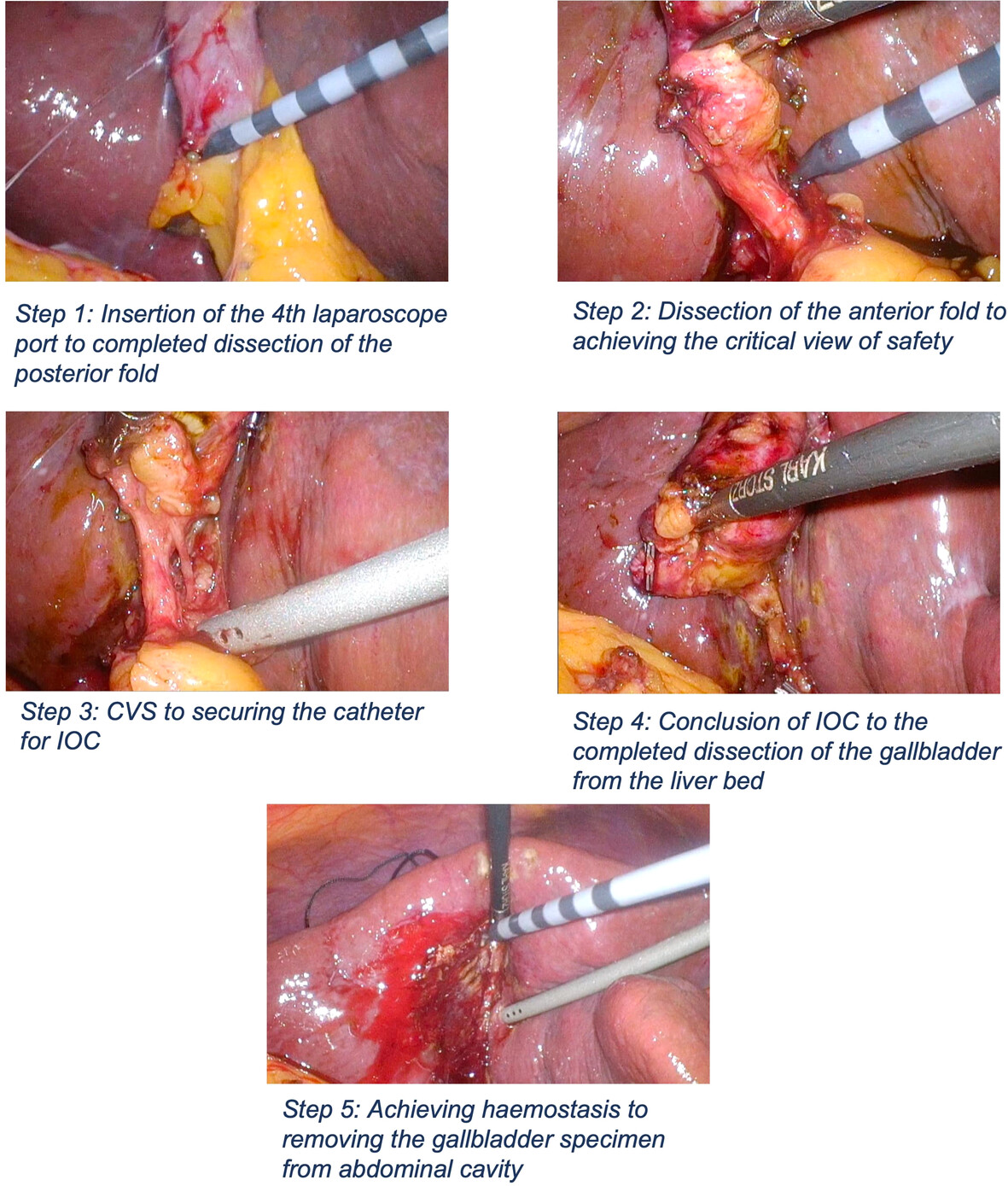
With advances in technology in surgery, it is important to determine if they are gimmicks or if it has any clinical value. This paper explores the impact of 3D visualisation systems on difficult laparoscopic cholecystectomy. It was determined that the critical step in achieving critical view of safety was completed faster and more efficiently with 3D systems when compared to traditional 2D.
Cholecystectomy in the red centre: a review of the surgical outcomes in Central Australia in a five-year period
- Pages: 1122-1126
- First Published: 29 April 2024

Indigenous Australians are more likely to require emergency cholecystectomy in Central Australia. There are barriers clinicians need to consider when managing this group of patient's.
COLORECTAL SURGERY
MRI-based parameters and clinical risk factors to predict lymph node metastasis in patients with ypT0 rectal cancer after neoadjuvant chemoradiotherapy
- Pages: 1127-1132
- First Published: 22 January 2024
This study is the first to utilize detailed MRI parameters in conjunction with clinical examination to predict lymph node metastasis in ypT0 patients.
Comparison of preoperative magnetic resonance imaging with postoperative pathology results in rectal cancer patients undergoing neoadjuvant therapy
- Pages: 1133-1137
- First Published: 12 February 2024
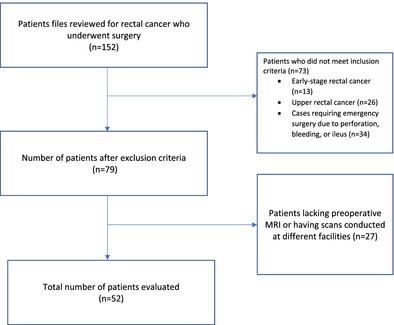
The study aimed to compare preoperative magnetic resonance imaging with postoperative pathology results in rectal cancer patients undergoing neoadjuvant therapy but found a limited concordance.
Management & surveillance of rectal neuroendocrine tumours: a single-centre retrospective analysis
- Pages: 1138-1145
- First Published: 12 February 2024
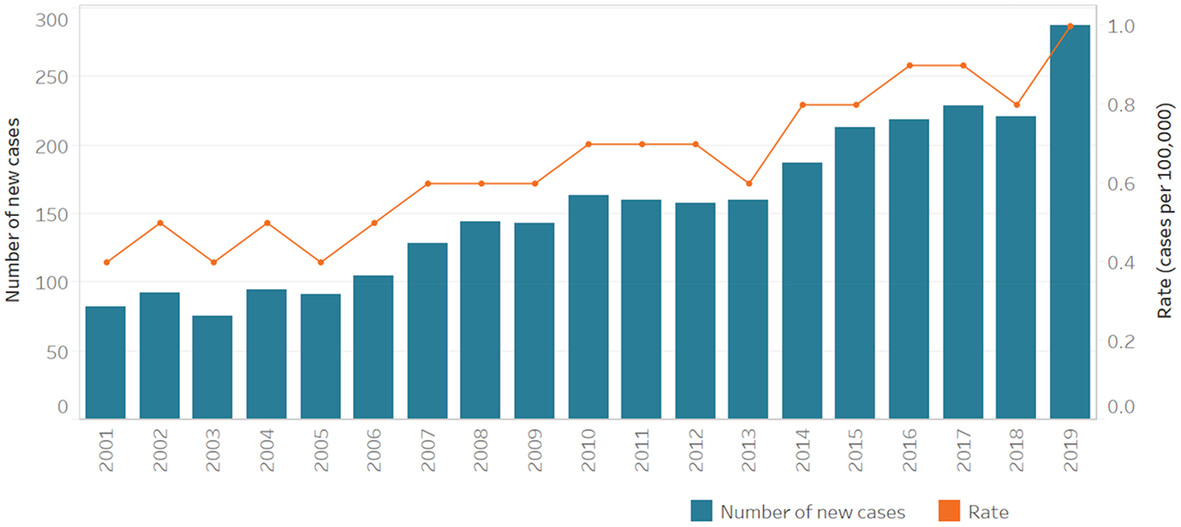
This is a retrospective single-centre study from QLD Australia looking at rectal neuroendocrine tumors diagnosed between 2012 and June 2023. 28 cases were identified and included in this study. Several observations were made including the increasing number of rNET diagnoses, the high incidence of R1 endoscopic resections within our cohort, the contribution of under-recognition and endoscopic resection technique to R1 results, and inconsistent surveillance practices. Recommendations from this study include increased endoscopist education for recognition and treatment of rNETs and increased education surrounding appropriate surveillance practice. We also advocate for further large-scale, prospective studies both to elucidate optimal techniques to achieve initial R0 resection and further understand the risk of surveilling small rNETs with an initial R1 resection.
Loss of psoas muscle during neoadjuvant treatment for rectal cancer is associated with poor oncological and surgical outcomes
- Pages: 1146-1150
- First Published: 14 March 2024

Psoas muscle change during neoadjuvant therapy is associated with worse outcomes in rectal cancer.
Comparing outcomes and cost in surgery versus watch & wait surveillance of patients with rectal cancer post neoadjuvant long course chemoradiotherapy
- Pages: 1151-1160
- First Published: 15 March 2024
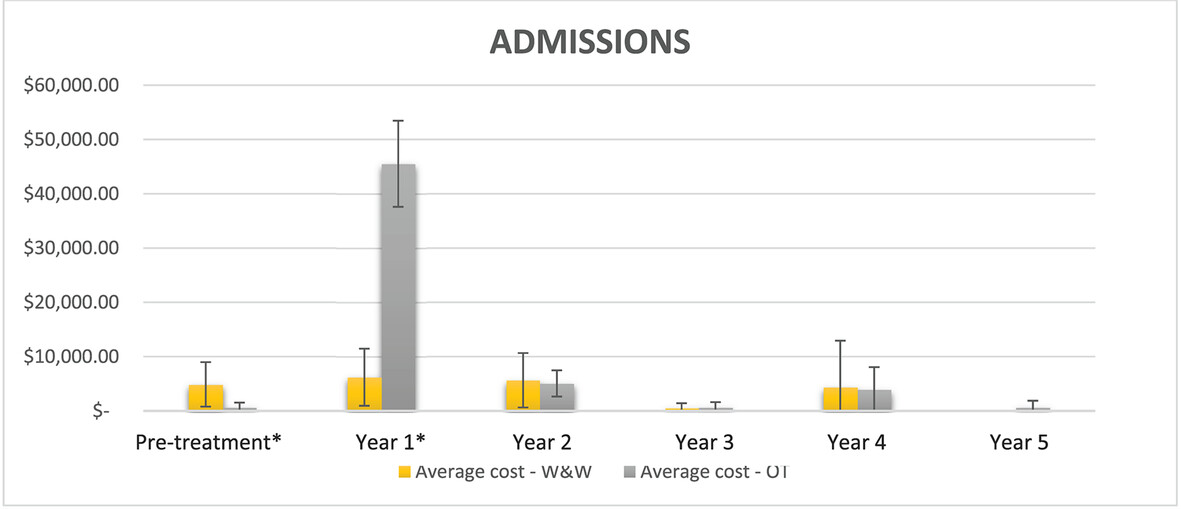
Watch and wait in complete clinical responders after neoadjuvant chemoradiotherapy is gaining prevalence as robust data confirms its oncological safety. Additionally, while surveillance can be expensive, the cost of sequelae from surgical morbidity is more so. Our study demonstrates that care in the OT group cost more than W&W, accounting for local regrowth management; $NZ70,759.56 versus $NZ47,905.52 (P = 0.014).
A single centre experience on the formation of double barrelled uro-colostomy in pelvic exenteration surgery: a cohort study
- Pages: 1161-1166
- First Published: 09 January 2024
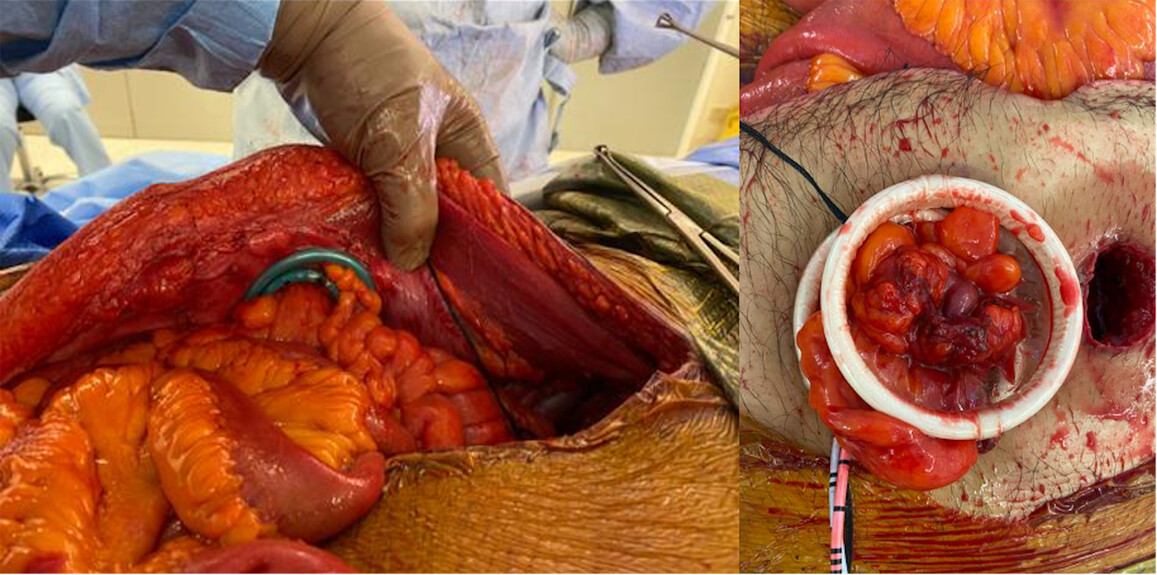
Double barrelled uro-colostomy (DBUC) is an alternative to traditional ileal conduit and separate colostomy in patients requiring simultaneous urinary and faecal diversion for reconstruction in pelvic exenteration surgery (PES). This cohort study demonstrated acceptable short- and long-term morbidity outcomes following DBUC formation in 20 consecutive adult patients undergoing PES in a New South Wales Complex Pelvic Surgical Unit.
HOW I DO IT
How to do laparoscopic right hemicolectomy with transvaginal natural orifice specimen extraction
- Pages: 1167-1169
- First Published: 26 April 2024
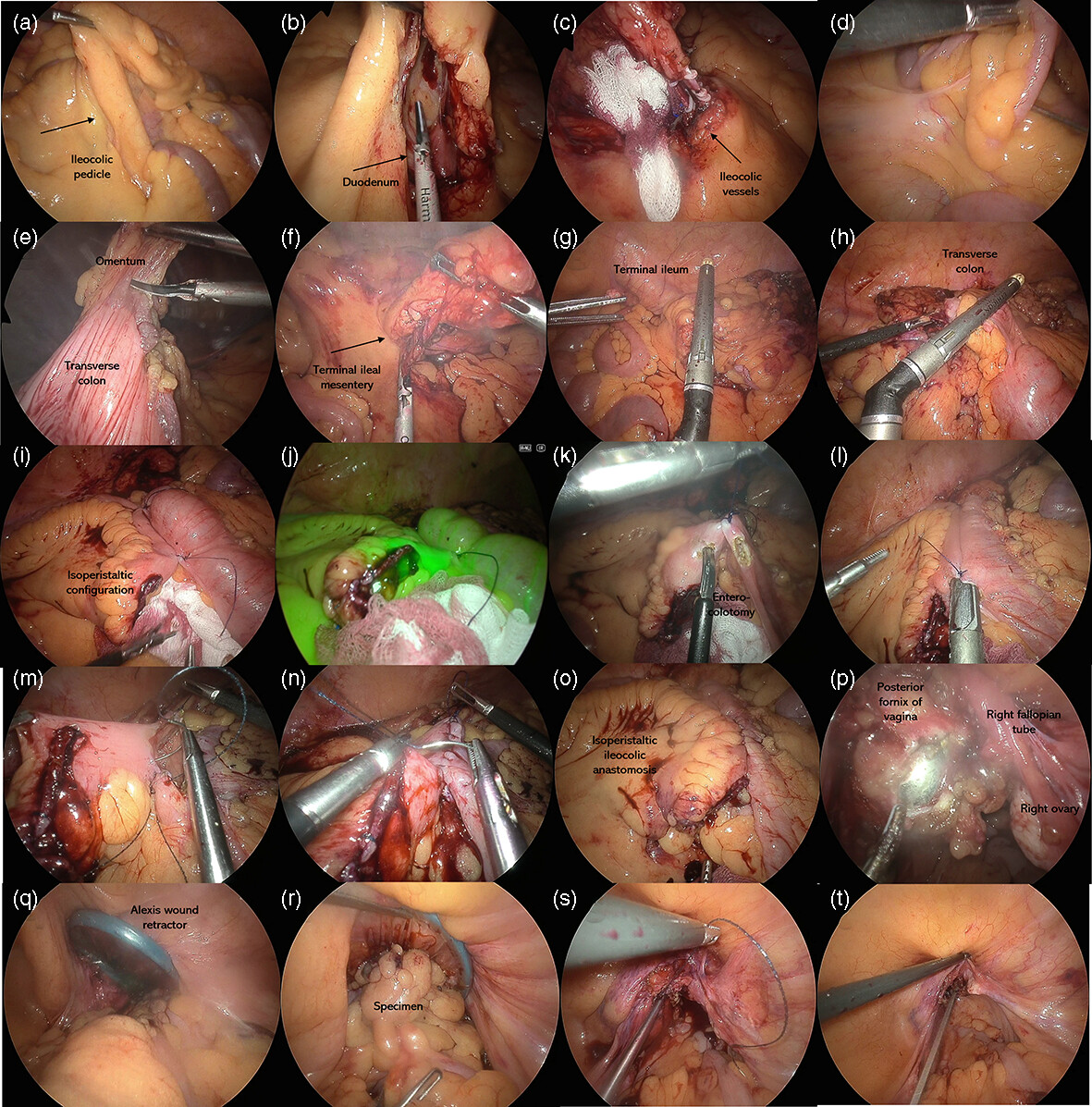
The key steps of performing a laparoscopic right hemicolectomy with transvaginal natural orifice specimen extraction surgery.
PROFESSIONAL SKILLS FOR SURGEONS
IMAGES FOR SURGEONS
When the pelvic water balloon isn't the bladder. A rare case of a seminal vesicle cystic tumour causing lower urinary tract symptoms
- Pages: 1184-1185
- First Published: 26 March 2024
Verrucous squamous cell carcinoma arising from recurrent chronic pilonidal disease
- Pages: 1186-1187
- First Published: 02 April 2024
Obstructed urosepsis secondary to a ureteroinguinal hernia, managed with urgent hernia repair
- Pages: 1188-1189
- First Published: 15 April 2024
LETTERS TO THE EDITOR
Re: Artificial intelligence is poised to usher in a paradigm shift in surgery
- Page: 1192
- First Published: 03 May 2024
RETRACTION
Retraction: Effect of magnesium on arrhythmia incidence in patients undergoing coronary artery bypass grafting
- Page: 1193
- First Published: 15 May 2024
Sign up for email alerts
Journal Information
ANZ Journal of Surgery is published on behalf of the Royal Australasian College of Surgeons.
![]()
ANZ J Surgery Resources