Journal list menu

 Issue
IssueEuropean Journal of Heart Failure: Volume 27, Issue 5
i-v, 743-934May 2025
Export Citations
Download PDFs
ISSUE INFORMATION
EDITORIAL
PHARMACOTHERAPIES
Position Paper
How to handle polypharmacy in heart failure. A clinical consensus statement of the Heart Failure Association of the ESC
- Pages: 747-759
- First Published: 17 March 2025
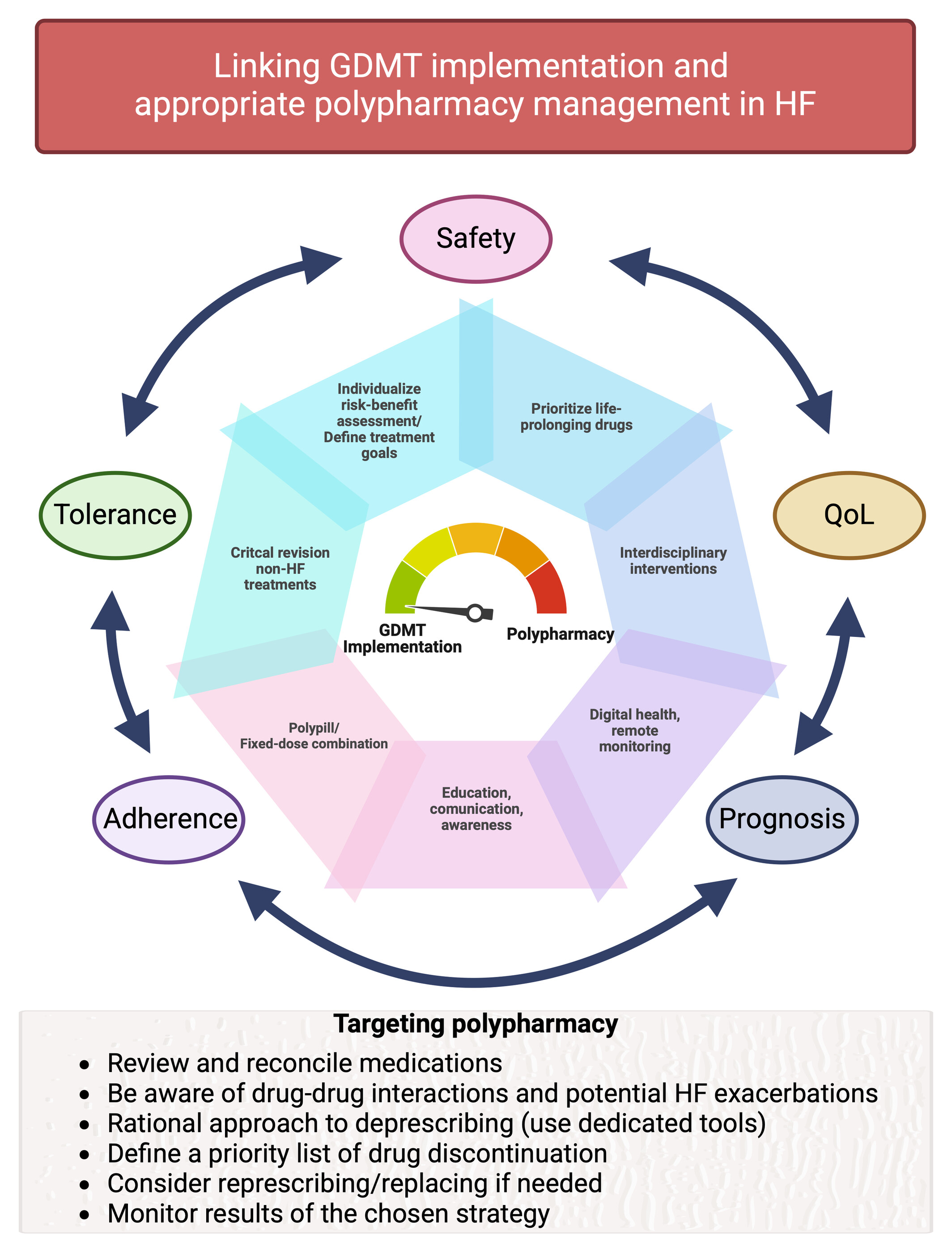
Linking guideline-directed medical therapy (GDMT) implementation and appropriate polypharmacy management in heart failure (HF). Polypharmacy can represent a barrier to the proper implementation of life-prolonging GDMT for HF. A reasonable balance between the optimization of GDMT and avoiding inappropriate polypharmacy is mandatory in the contemporary care of patients with HF. Clinicians are encouraged to use individualized risk–benefit assessments, and patient-centred goals should be defined and pursued, which include outcomes such as prognosis and quality of life (QoL), or factors more related with treatments such as adherence, tolerance and safety. There are multiple aspects that can contribute to the success of the overall process: collaboration with other healthcare professionals and structured interdisciplinary interventions, implementation of digital technologies, use, when appropriate, of fixed-dose combinations for simplification of medication regimens. Life-prolonging medications should be regularly prioritized during the processes of medication revision and appropriateness of non-HF treatment medications critically reassessed. Targeting polypharmacy through a stepwise approach can contribute to facilitate GDMT implementation strategies, to preserve adherence and, finally, to better GDMT.
Invited Editorial
Time for a new perspective on polypharmacy in heart failure
- Pages: 760-763
- First Published: 27 March 2025
CLINICAL STUDIES
Research Article
Efficacy and safety of finerenone in patients with chronic kidney disease and type 2 diabetes by diuretic use: A FIDELITY analysis
- Pages: 764-774
- First Published: 17 January 2025
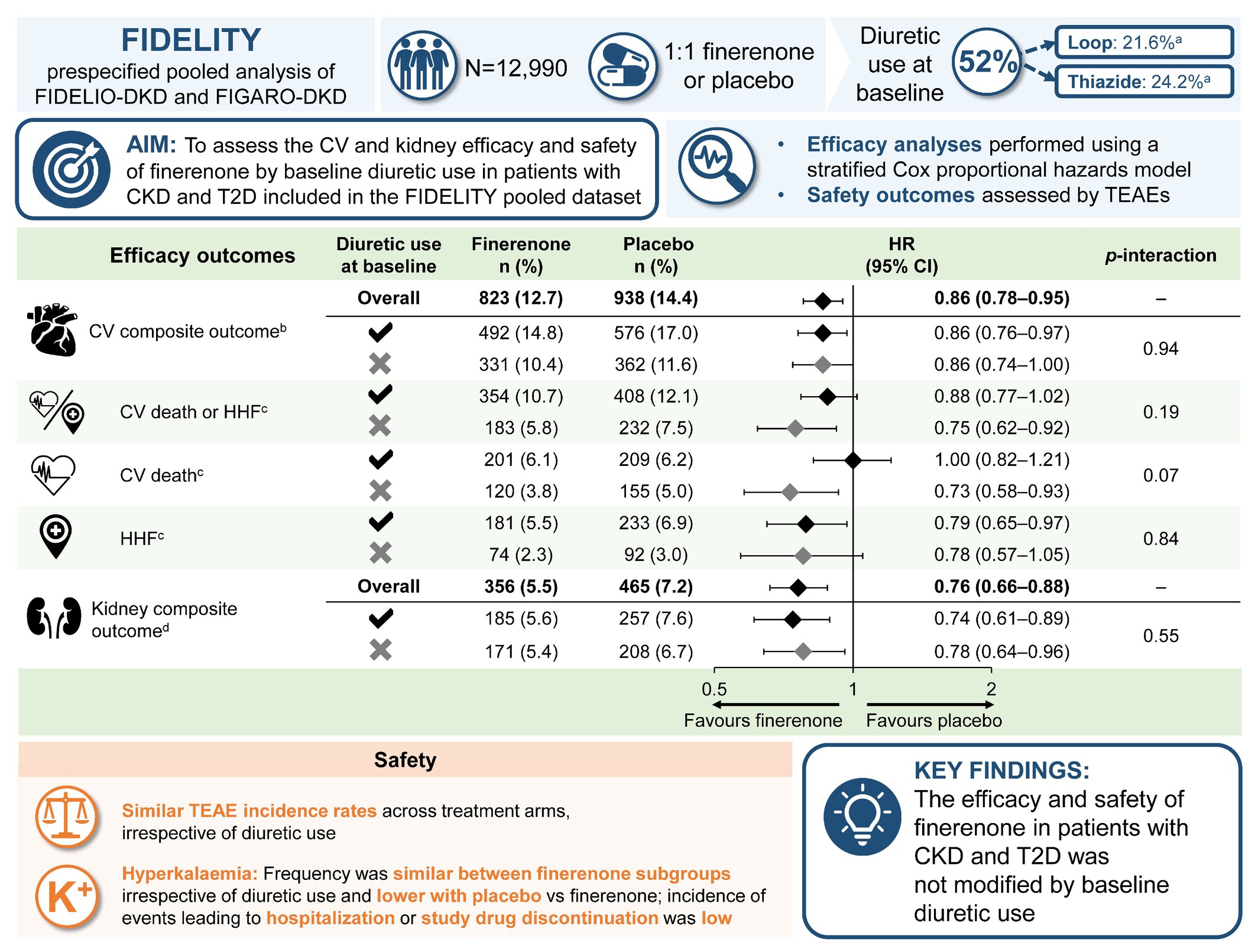
Efficacy and safety of finerenone in patients with chronic kidney disease and type 2 diabetes by diuretic use: a FIDELITY analysis. CI, confidence interval; CKD, chronic kidney disease; CV, cardiovascular; eGFR, estimated glomerular filtration rate; FIDELIO-DKD, FInerenone in reducing kiDnEy faiLure and dIsease prOgression in Diabetic Kidney Disease; FIDELITY, FInerenone in chronic kiDney diseasE and type 2 diabetes: Combined FIDELIO-DKD and FIGARO-DKD Trial programme analYsis; FIGARO-DKD, FInerenone in reducinG cArdiovascular moRtality and mOrbidity in Diabetic Kidney Disease; HHF, hospitalization for heart failure; HR, hazard ratio; K+, potassium; MI, myocardial infarction; T2D, type 2 diabetes; TEAE, treatment-emergent adverse event. aIf patients were receiving both types of diuretics at baseline, they were included in both subgroups. Patients receiving diuretics who were not included in either group were taking non-loop, non-thiazide diuretics. bComposite of time to CV death, non-fatal MI, non-fatal stroke, or HHF. cCV composite outcome component(s). dComposite of time to kidney failure, sustained ≥57% decrease in eGFR from baseline over ≥4 weeks, or kidney-related death.
Invited Editorial
Effect of finerenone across the stages of heart failure: From prevention to treatment
- Pages: 775-778
- First Published: 17 February 2025
Research Article
Effects of sacubitril/valsartan according to background beta-blocker therapy in patients with heart failure and reduced ejection fraction: Insights from PARADIGM-HF
- Pages: 779-787
- First Published: 19 November 2024
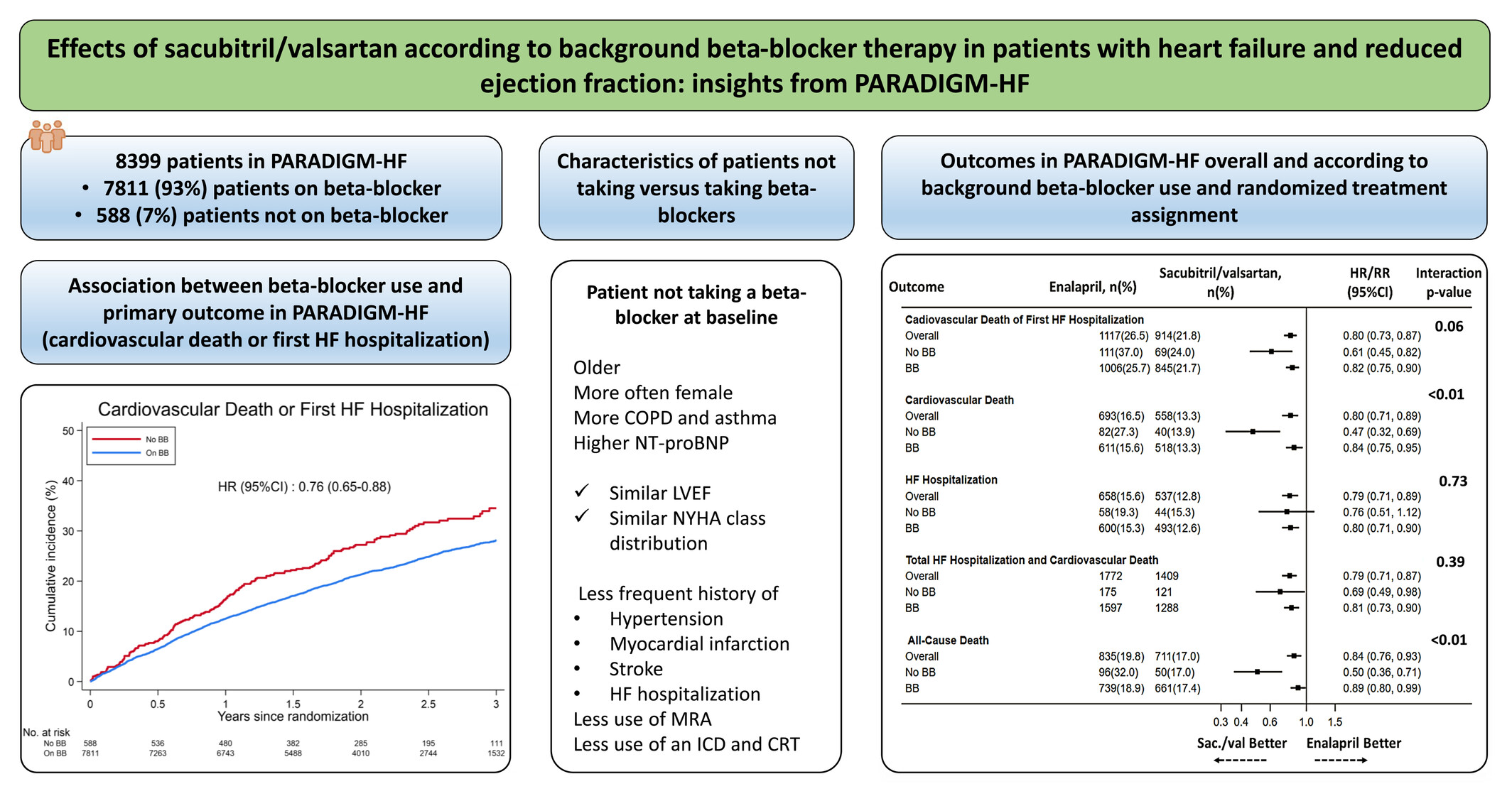
Effects of sacubitril/valsartan with or without background beta-blocker therapy in patients with heart failure with reduced ejection fraction from PARADIGM-HF. BB, beta-blocker; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CRT, cardiac resynchronization therapy; HF, heart failure; HR, hazard ratio; ICD, implantable cardioverter-defibrillator; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association; RR, rate ratio.
Sex differences in cardiac structure and function following acute myocardial infarction: Insights from the PARADISE-MI echocardiographic substudy
- Pages: 788-799
- First Published: 24 September 2024
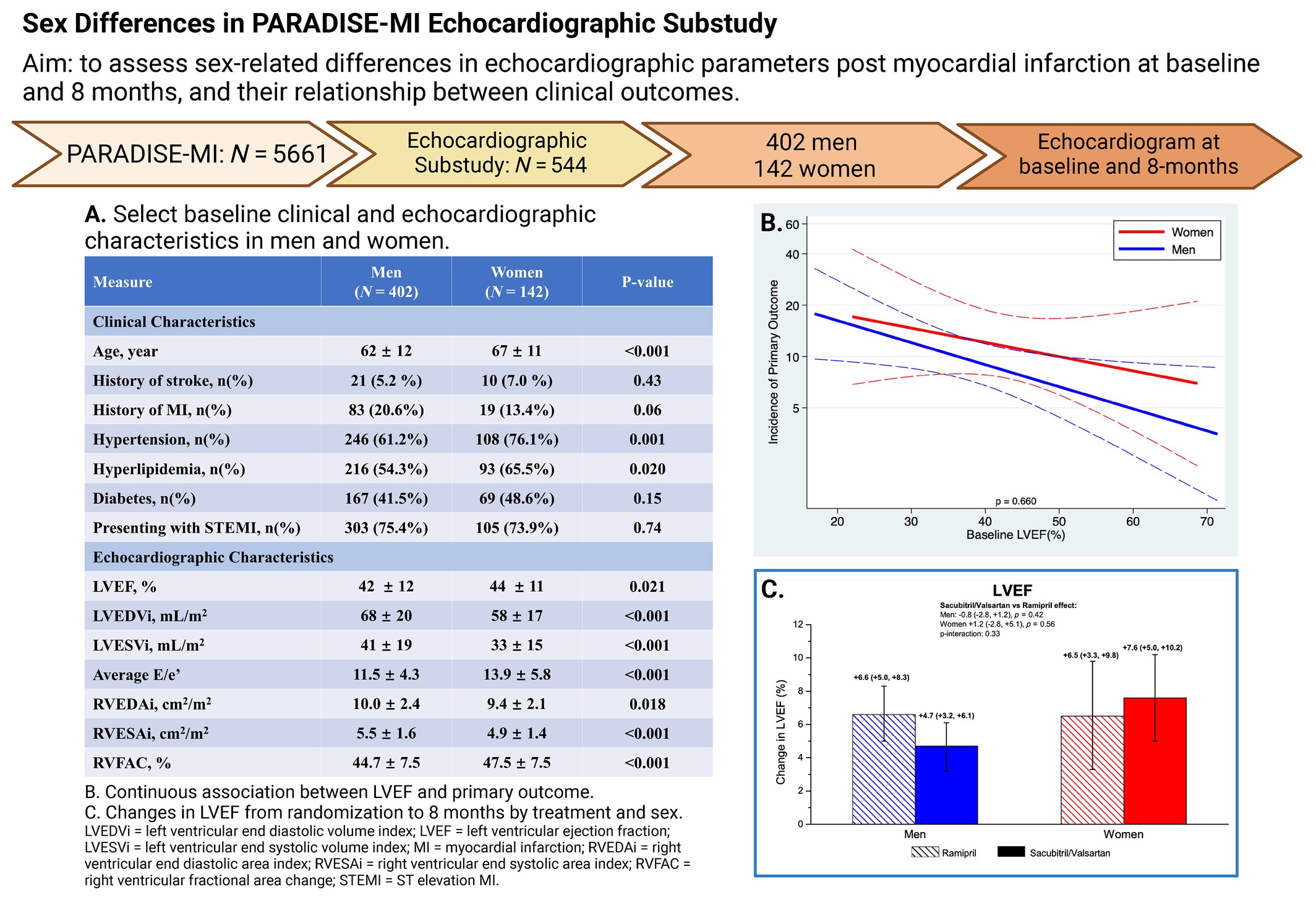
Sex differences in the PARADISE-MI echocardiographic substudy.
Invited Editorial
Failure to improve cardiac remodelling and outcomes post-myocardial infarction: Insights from EMPRESS-MI
- Pages: 800-803
- First Published: 12 February 2025
Beta-blockers and heart failure with mildly reduced and preserved ejection fraction. A personalized approach beyond the heart failure syndrome phenotypes is needed
- Pages: 804-807
- First Published: 21 January 2025
ADVANCED AND ACUTE HEART FAILURE
Position Paper
Research Article
Time-varying analyses of survival and outcomes in patients with HeartMate 3 left ventricular assist devices
- Pages: 822-829
- First Published: 09 January 2025
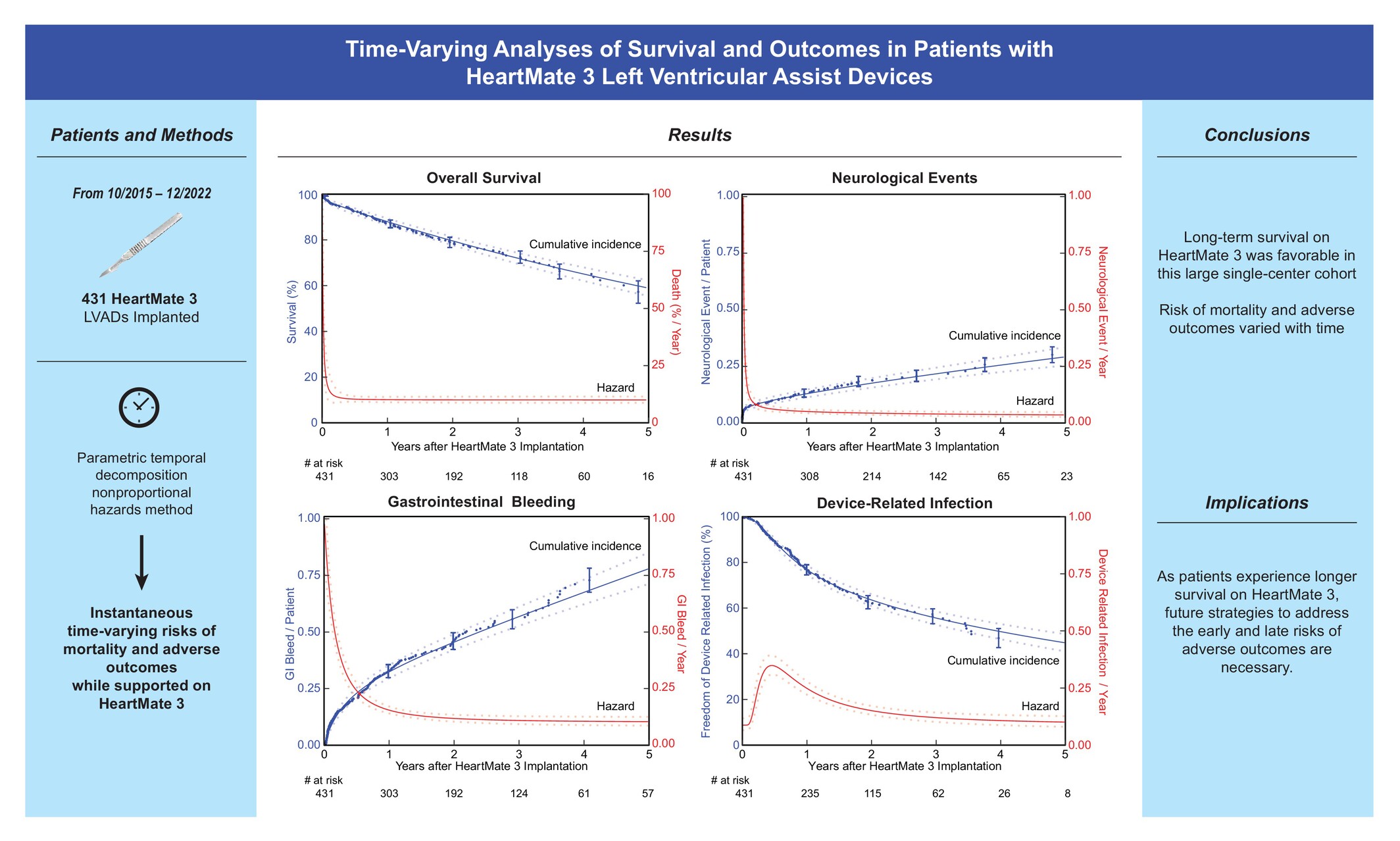
HeartMate 3 time-varying analyses. LVAD, left ventricular assist device.
Invited Editorial
Recognizing the temporal variability of adverse events after HeartMate 3 implantation: Tackling the expected event at the right time
- Pages: 830-831
- First Published: 05 February 2025
Research Article
Incidence and predictors of weaning failure from veno-arterial extracorporeal membrane oxygenation therapy in patients with cardiogenic shock
- Pages: 832-841
- First Published: 17 January 2025
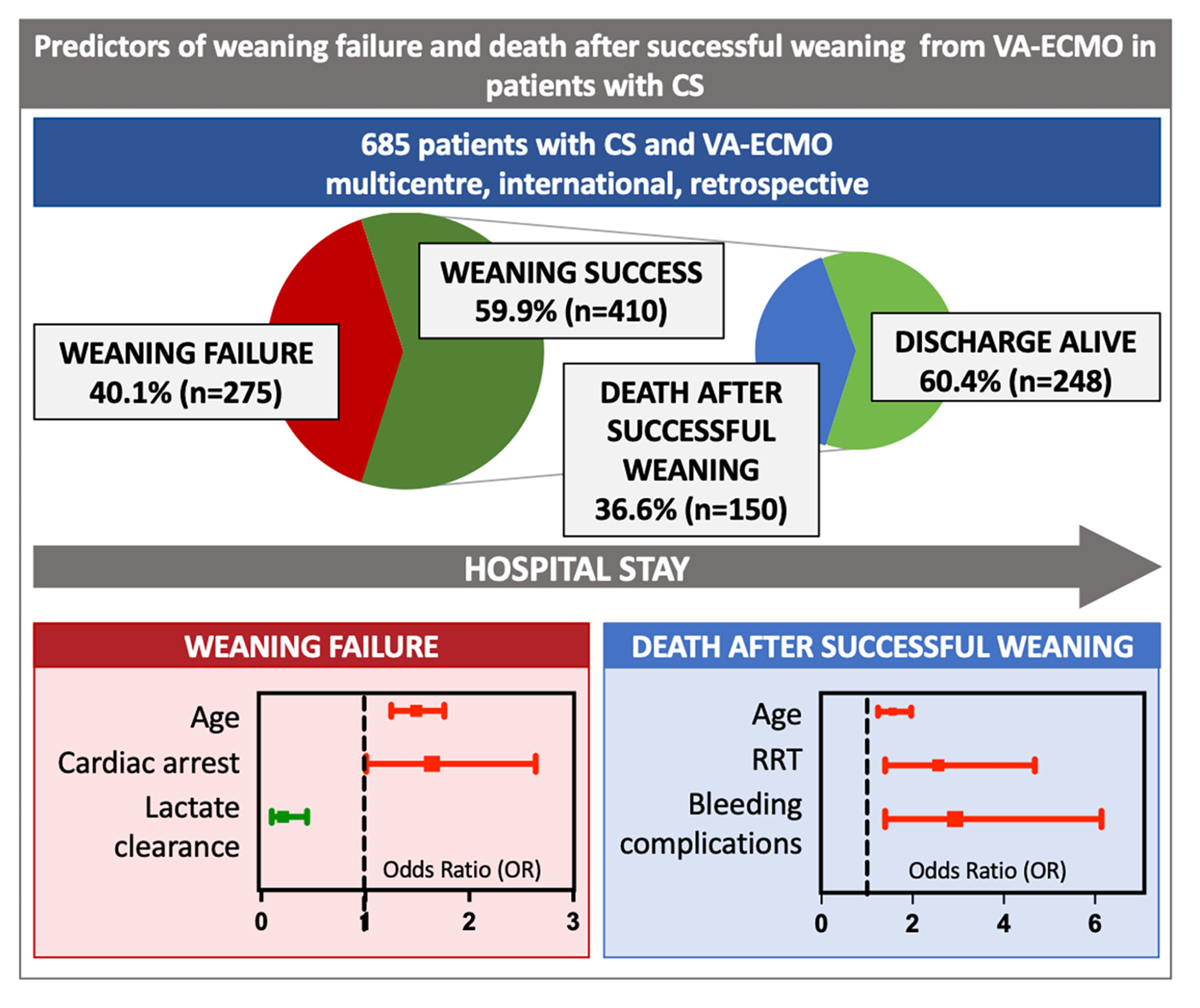
Predictors of weaning failure from veno-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiogenic shock. RRT, renal replacement therapy.
Invited Editorial
What can be done to improve the outcomes for cardiogenic shock patients with circulatory support devices?
- Pages: 842-843
- First Published: 12 February 2025
MARKERS AND MECHANISMS
Research Article
Unlocking the power of empagliflozin: Rescuing inflammation in hyperglycaemia-exposed human cardiomyocytes through comprehensive multi-level analysis
- Pages: 844-856
- First Published: 14 January 2025
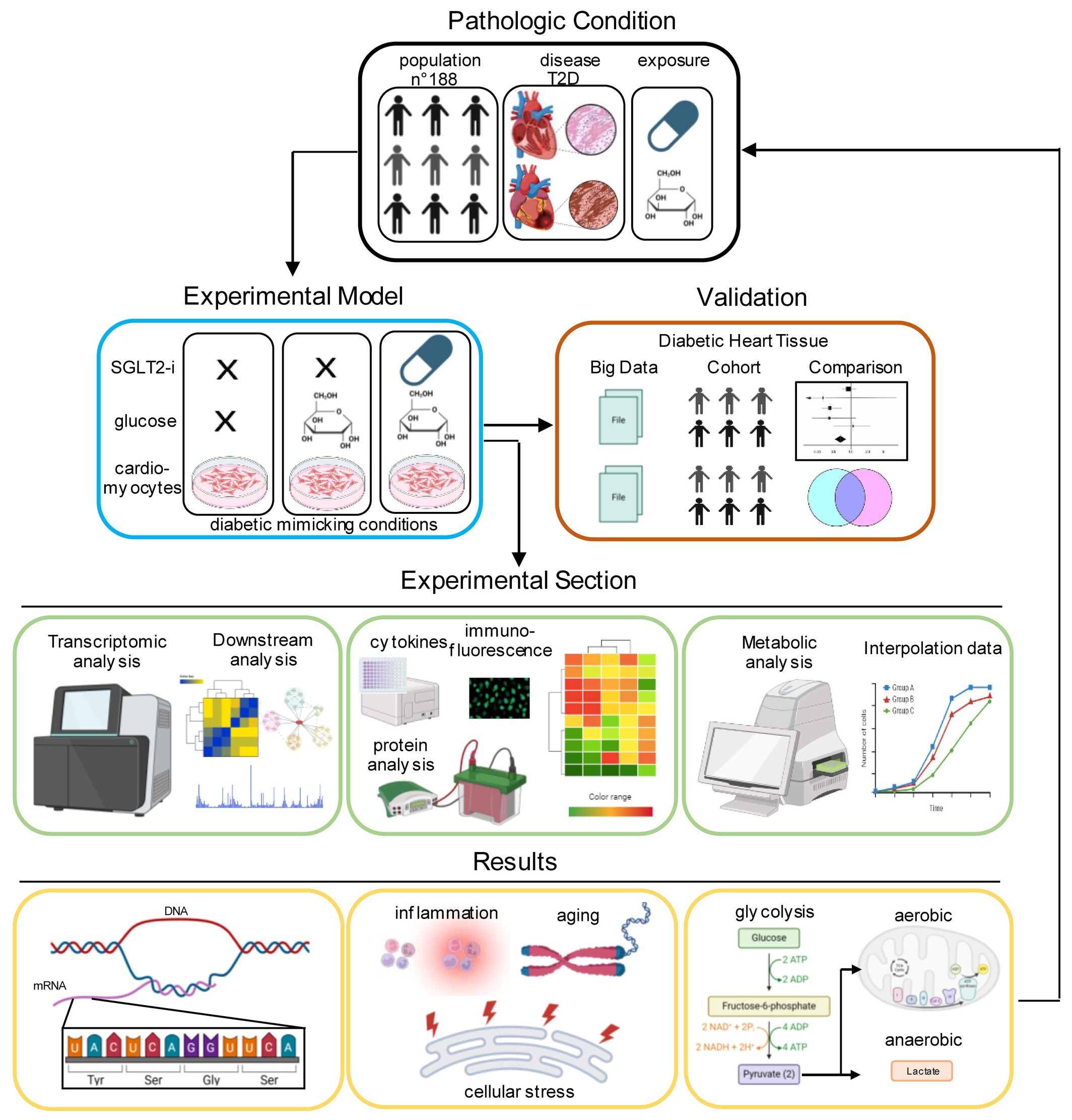
Schematic representation of the study workflow, pathological model, experimental workflow, and key findings deriving from the integration of clinical trials, public databases, and the cellular model. SGLT2-i, sodium–glucose cotransporter 2 inhibitor; T2D, type 2 diabetes.
Invited Editorial
Empagliflozin's anti-inflammatory spectrum in type 2 diabetes mellitus: Piecing together the puzzle
- Pages: 857-859
- First Published: 12 February 2025
Research Article
Association of ventricular–arterial coupling with biomarkers involved in heart failure pathophysiology – the STANISLAS cohort
- Pages: 860-871
- First Published: 27 August 2024
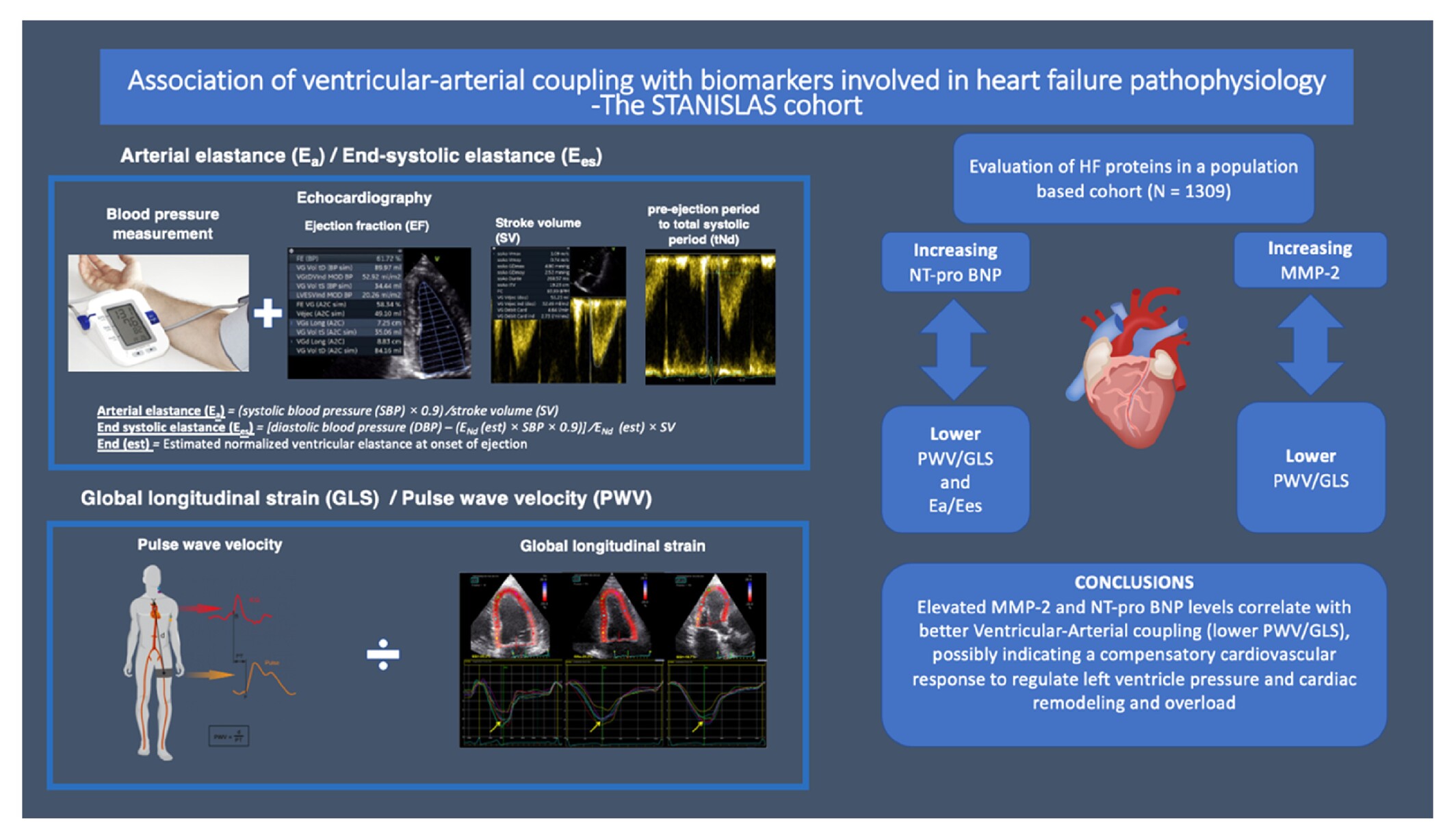
Association of ventricular–arterial coupling with heart failure (HF) biomarkers in the STANISLAS cohort. MMP, matrix metalloproteinase; NT-proBNP, N-terminal pro-B-type natriuretic peptide.
Characterization of serum phosphate levels over time with intravenous ferric carboxymaltose versus placebo as treatment for heart failure with reduced ejection fraction and iron deficiency: An exploratory prospective substudy from HEART-FID
- Pages: 872-880
- First Published: 19 June 2024
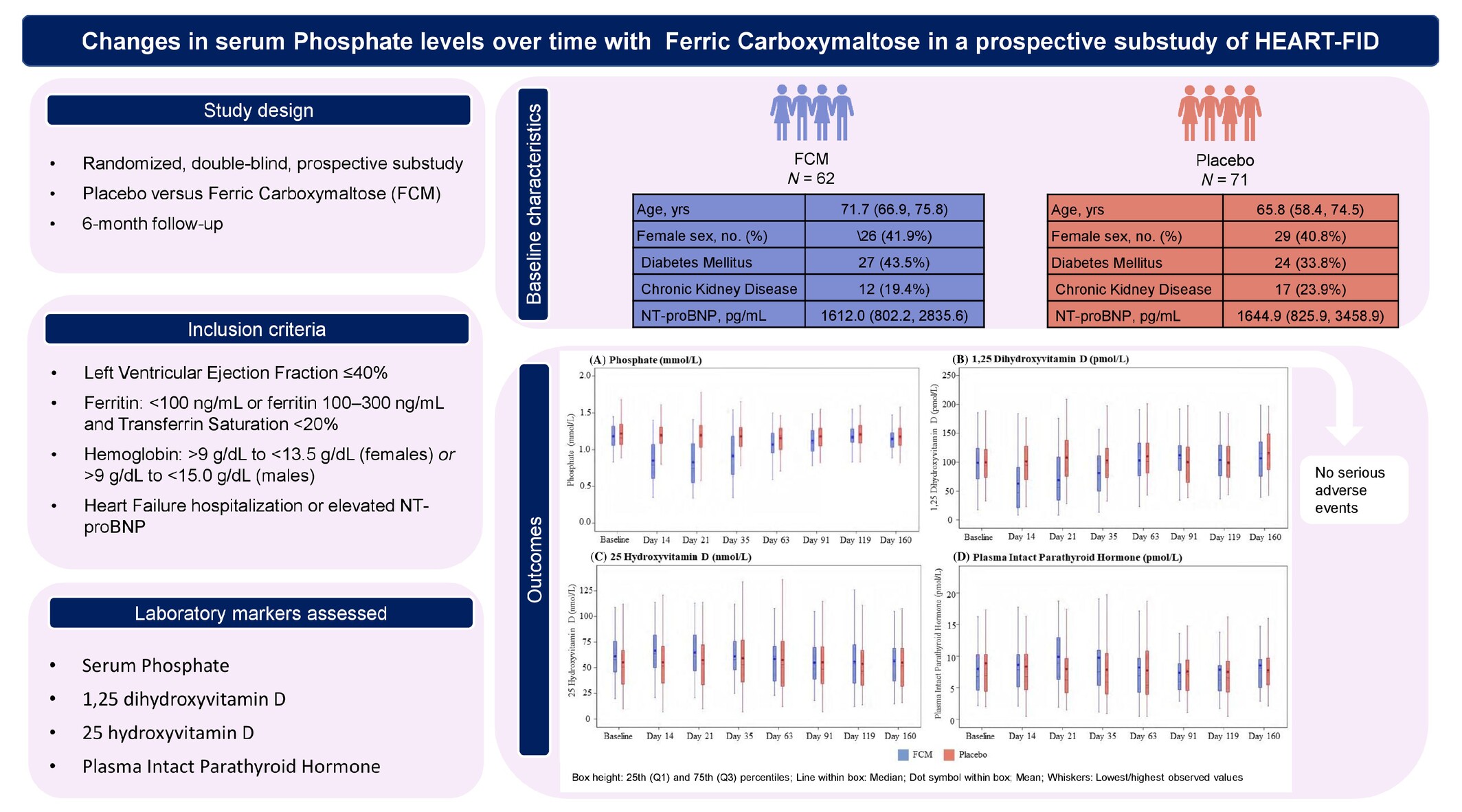
Changes in serum phosphate levels over time with ferric carboxymaltose (FCM) in a randomized, double-blind, prospective substudy of HEART-FID assessing the following outcomes: serum phosphate, 1,25 dihydroxyvitamin D, 25-hydroxyvitamin D levels and plasma levels of intact parathyroid hormone during 6 months subsequent to FCM infusion. The study included a total of 133 patients (n = 62 FCM, n = 71 placebo). Outcomes are shown for each substudy visit at baseline through day 14, 21, 35, 63, 91, 119, and 160. NT-proBNP, N-terminal pro-B-type natriuretic peptide.
Disease progression in chronic heart failure is linear: Insights from multistate modelling
- Pages: 881-888
- First Published: 06 August 2024
Associations of iron deficiency with cardiac function, congestion, exercise capacity and prognosis in heart failure
- Pages: 889-900
- First Published: 28 November 2024
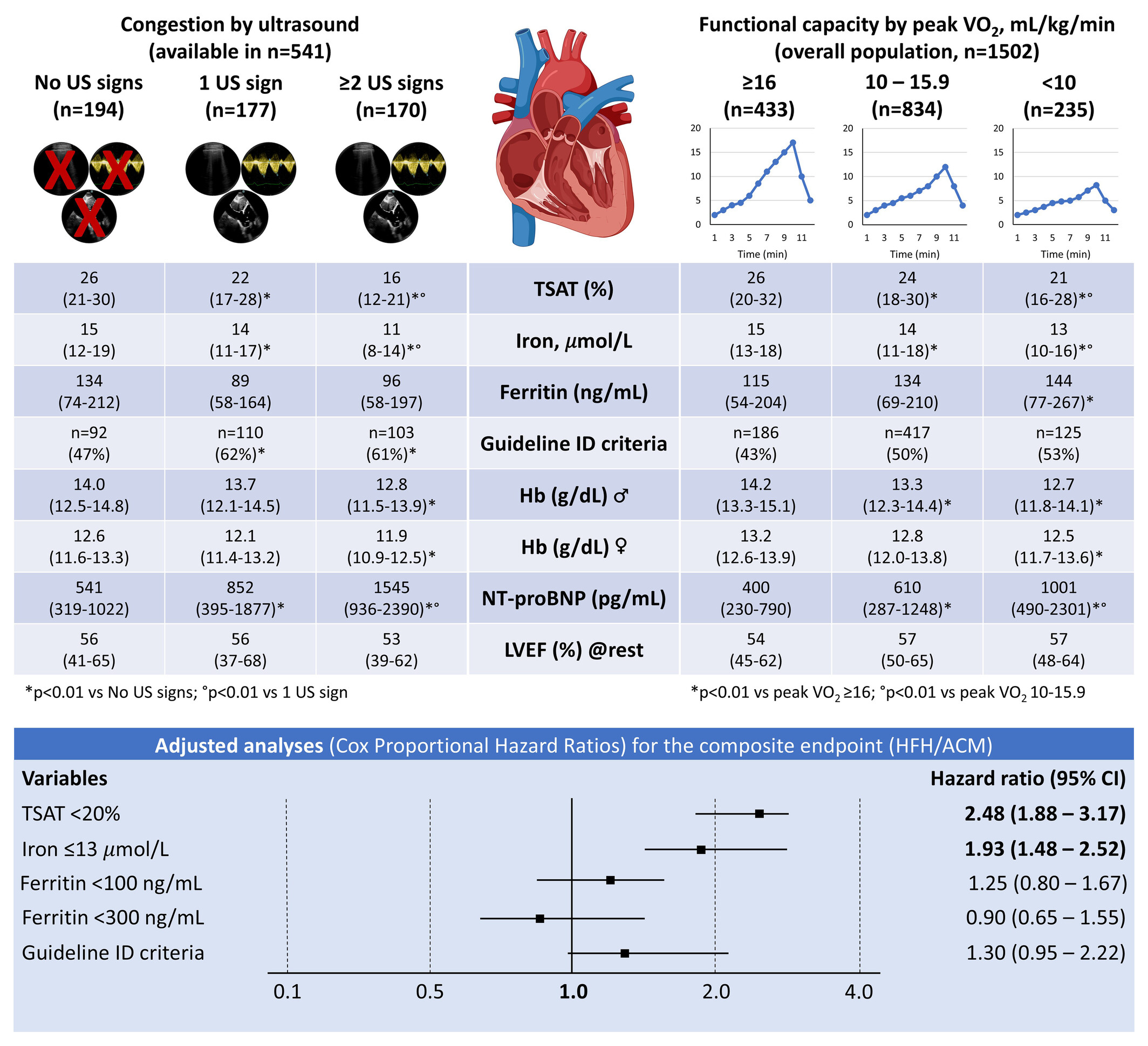
Association of iron markers with congestion, functional capacity and prognosis. Congestion assessment at rest by ultrasound: B-lines ≥4, discontinuous renal venous flow and dilated inferior vena cava (≥21 mm). Functional capacity by peak oxygen uptake (VO2): ≥16 ml/kg/min, 10–15.9 ml/kg/min and <10 ml/kg/min. Adjusted analyses (Cox proportional hazard ratios) illustrate a higher risk of heart failure hospitalization (HFH) and all-cause mortality (ACM) after a median follow-up of 18 months in patients with heart failure and iron deficiency (ID) as assessed by transferrin saturation (TSAT) <20% and iron ≤13 μmol/L. All models were adjusted for age (years), sex (male), diabetes, haemoglobin (Hb, g/dl), estimated glomerular filtration rate (ml/min/1.73 m2), Ln(NT-proBNP) (pg/ml), Ln (hs-CRP) (mg/dl), atrial fibrillation/flutter, peak VO2 <16 ml/kg/min and heart failure phenotype (heart failure with preserved vs. reduced ejection fraction), including its interaction with iron markers. CI, confidence interval; hs-CRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide; US, ultrasound.
Short Report
High variability in assays of blood markers of collagen turnover in cardiovascular disease: Implications for research and clinical practice
- Pages: 901-904
- First Published: 09 July 2024
Peroxiredoxin-4, a marker of systemic oxidative stress, is associated with incident heart failure
- Pages: 905-911
- First Published: 06 April 2025
VALVE INTERVENTIONS
Research Article
Transcatheter edge-to-edge repair in severe mitral regurgitation following acute myocardial infarction – aetiology-based analysis
- Pages: 912-921
- First Published: 14 January 2025
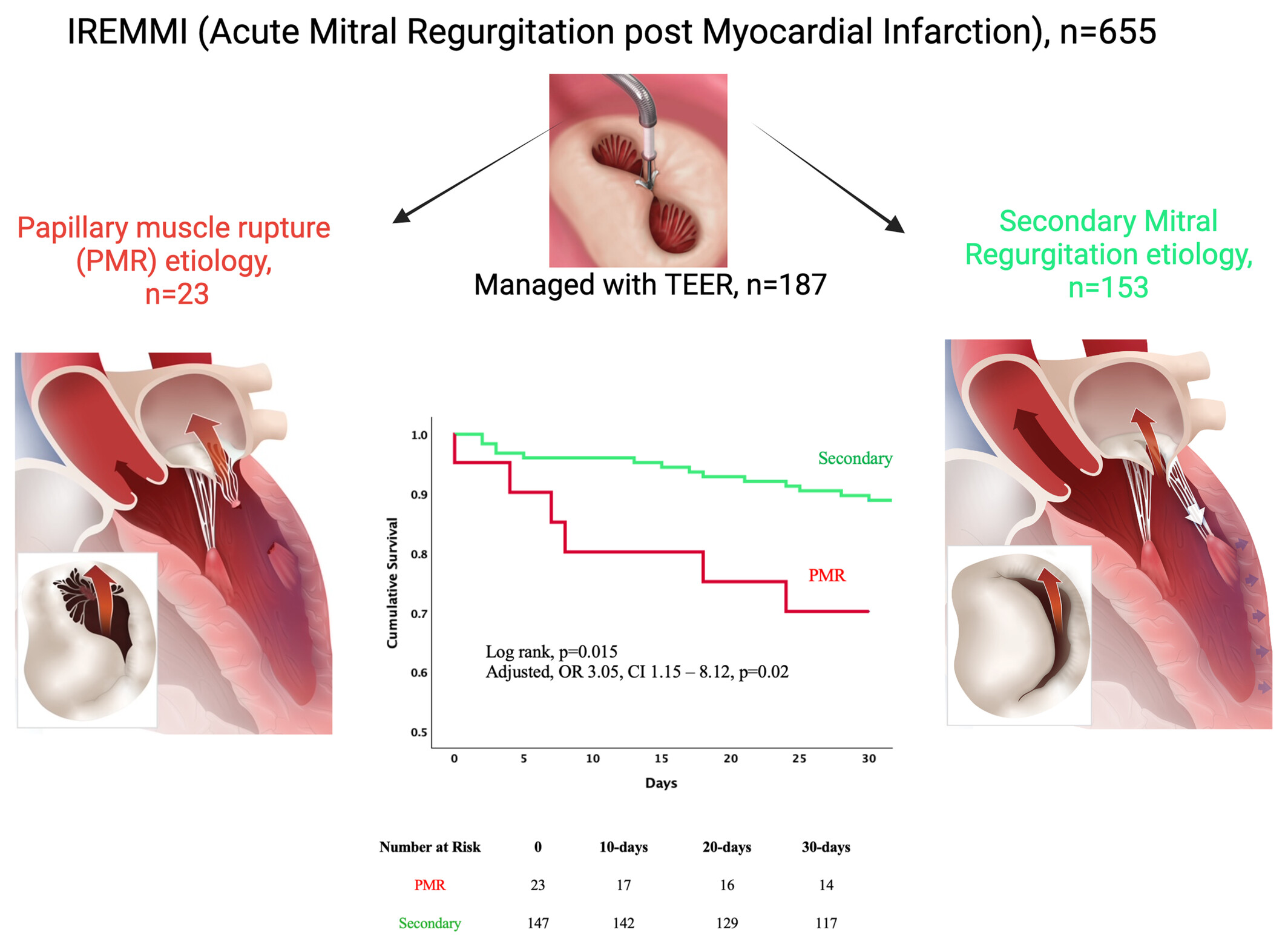
The International Registry of MitraClip in Acute Mitral Regurgitation following Acute Myocardial Infarction (IREMMI). CI, confidence interval; OR, odds ratio; TEER, transcatheter edge-to-edge repair.
Invited Editorial
Rescuing patients with post-myocardial infarction mitral regurgitation with transcatheter edge-to-edge repair: A salvation for all mechanisms of mitral regurgitation
- Pages: 922-923
- First Published: 12 February 2025
Research Letter
Tricuspid regurgitation risk scores in patients undergoing tricuspid valve transcatheter edge-to-edge repair
- Pages: 924-925
- First Published: 05 February 2025
Invited Editorial
Therapeutic decision making in tricuspid regurgitation: Many risk scores for transcatheter repair with no specific answer
- Pages: 926-928
- First Published: 10 March 2025
CORRESPONDENCE
Letter regarding the article ‘Efficacy and safety of angiotensin receptor–neprilysin inhibition in heart failure patients with end-stage kidney disease on maintenance dialysis: A systematic review and meta-analysis’
- Page: 929
- First Published: 10 February 2025
Reply to the letter regarding the article ‘Efficacy and safety of angiotensin receptor–neprilysin inhibition in heart failure patients with end-stage kidney disease on maintenance dialysis: A systematic review and meta-analysis’
- Pages: 929-932
- First Published: 10 February 2025
Letter regarding the article ‘Association of clonal haematopoiesis with heart failure incidence and outcomes: A systematic review and meta-analysis’
- Pages: 932-933
- First Published: 09 April 2025
Reply to the letter regarding the article ‘Association of clonal haematopoiesis with heart failure incidence and outcomes: A systematic review and meta-analysis’
- Pages: 933-934
- First Published: 09 April 2025
Sign up for email alerts
Tools
Published on behalf of the Heart Failure Association of the European Society of Cardiology