


All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Norovirus Management and Outcomes in a Multicenter Pediatric Kidney Transplant Populationoa
Graphical Abstract
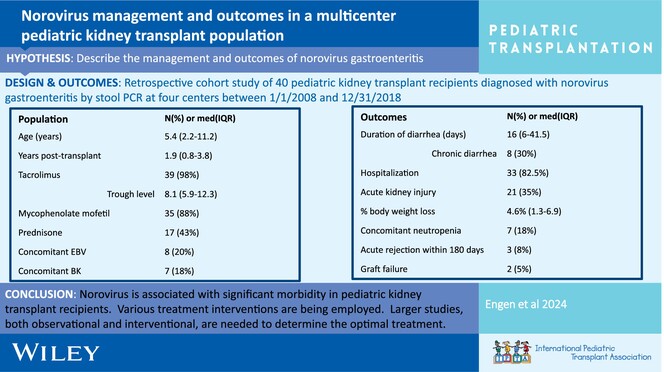
Post-transplant norovirus diarrhea persists for a median of 16 days (IQR 6–41.5 days) with 30% of patients developing chronic diarrhea. Morbidity is high, including AKI in 53% of patients, reduction in immunosuppression 20%, and acute rejection in 8% within 6 months of diagnosis.
-
BK polyomavirus DNAemia, allograft rejection, and de novo donor-specific antibodies after lowering target tacrolimus levels in pediatric kidney transplant recipientsno
Graphical Abstract
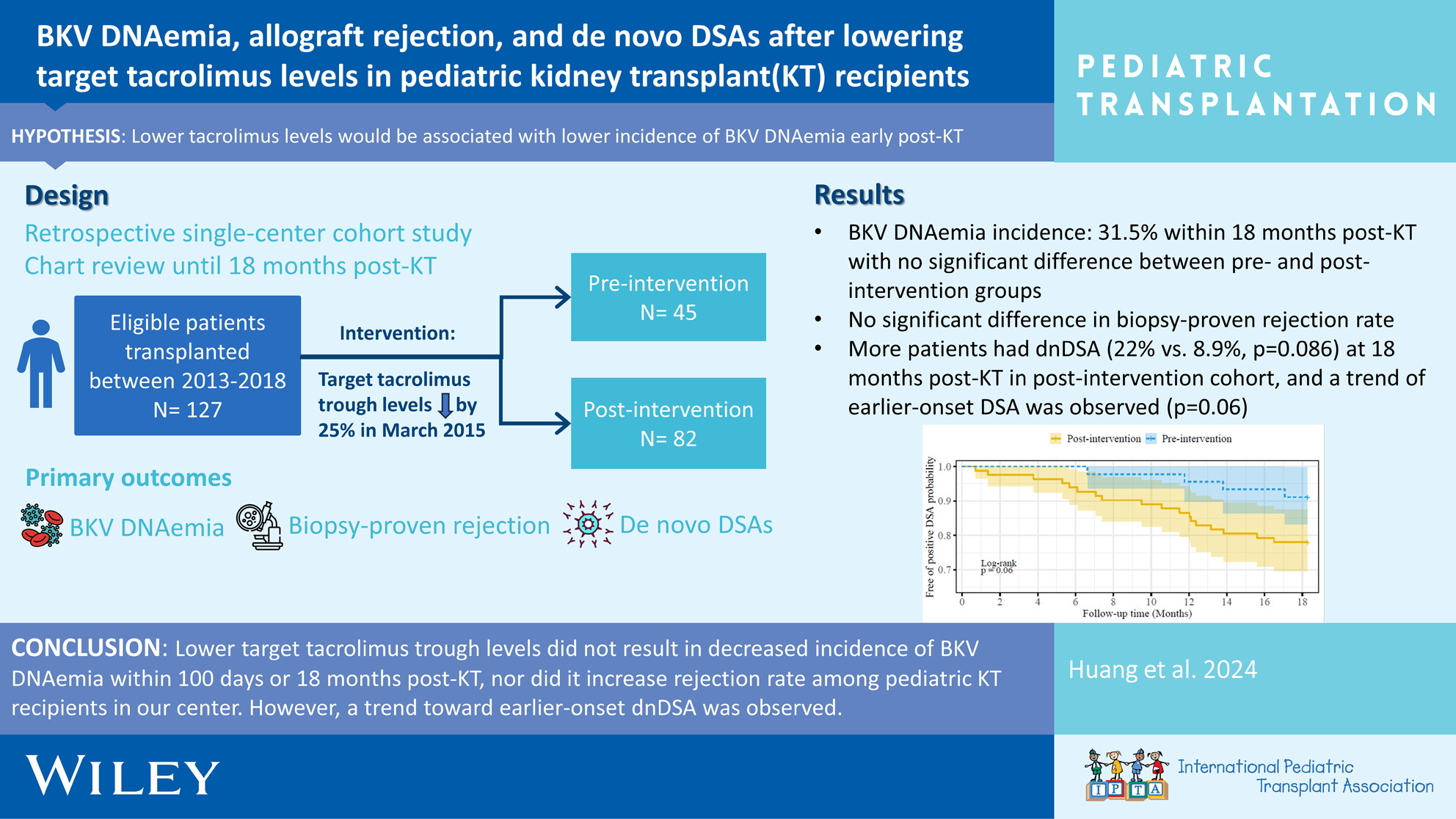
Early BKV DNAemia is common post-pediatric kidney transplant, especially in younger ages, with ~30% incidence within 18 months post-transplant. Favorable outcomes are achieved with (1) frequent monitoring of viremia and (2) timely reduction of immunosuppressive medications, which must be balanced against risk of rejection and development of HLA antibodies.
-
Adrenal insufficiency in pediatric kidney transplantation recipientsoa
Graphical Abstract
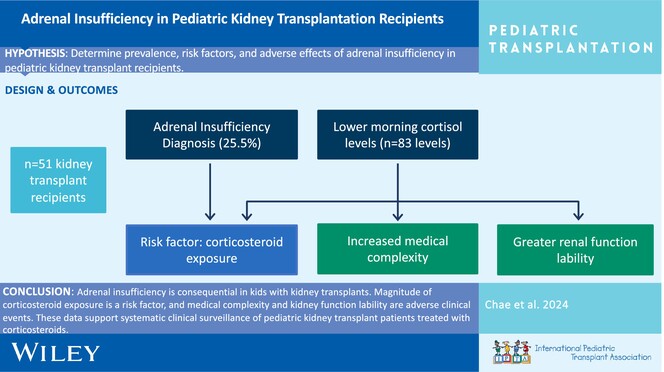
Adrenal insufficiency is common in pediatric kidney transplant recipients. Corticosteroid exposure is a risk factor, and medical complexity and kidney function lability are adverse clinical outcomes. These data support systemic clinical surveillance of adrenal insufficiency in pediatric kidney transplant recipients treated with corticosteroids.
-
Alemtuzumab induction is associated with decreased hospitalization rates in pediatric kidney transplant: A UNOS data review for safety and outcomes with common induction regimensno
Graphical Abstract
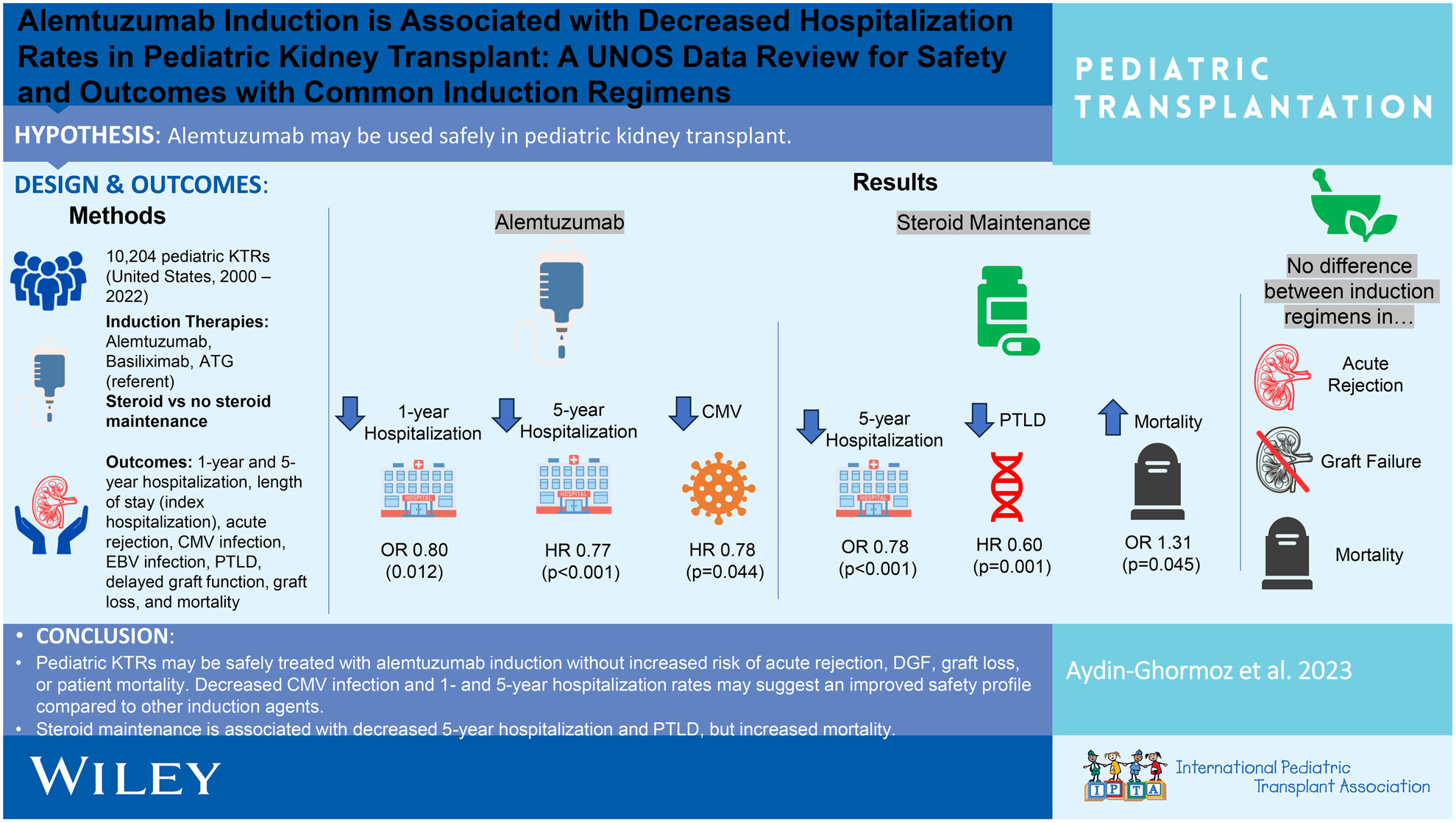
Pediatric KTRs may be safely treated with alemtuzumab induction without increased acute rejection, delayed graft function, graft loss, or patient mortality, but with decreased CMV infection and 1 and 5 years hospitalization rates. Steroid maintenance is associated with decreased 5 years hospitalization and PTLD, but increased mortality.
-
Safety and infectious outcomes in pediatric kidney transplant recipients after COVID-19 vaccination: A pediatric nephrology research consortium studyno
Graphical Abstract
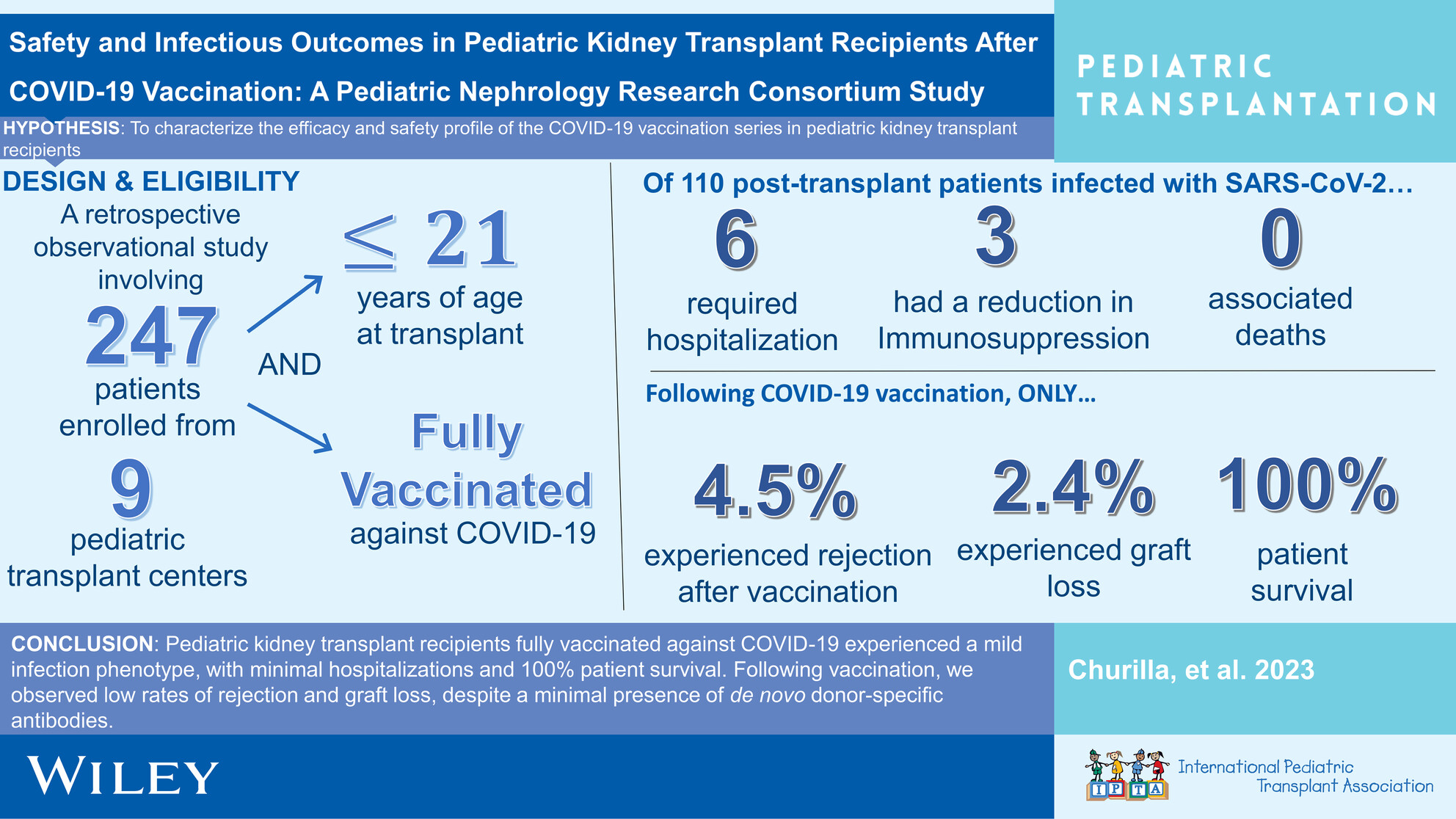
This observational, retrospective investigation demonstrates temporal associations pointing to a reassuring vaccine safety profile and mild SARS-Cov-2 infectious phenotype in pediatric renal transplant recipients fully vaccinated against COVID-19.
-
Pregnancy after transplant in the older adolescent: Anticipatory guidance for the pediatric providernoCollections: Special Issue on Adolescence and Transplantation
Graphical Abstract
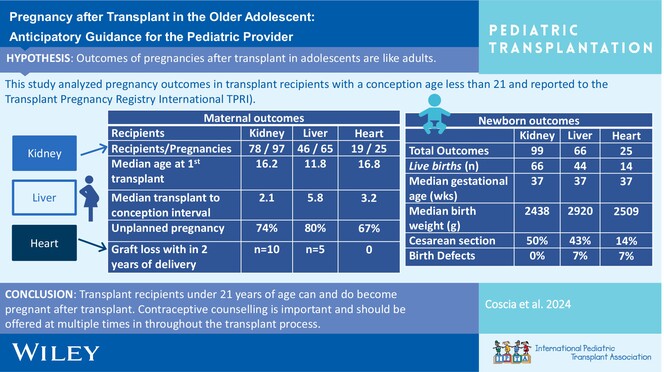
This manuscript will provide a brief review of current recommendations for contraception for adolescent and young adult solid organ transplant recipients, a short review of immunosuppression and pregnancy exposure, overview of outcomes in recipients who had a pregnancy before age 21 years, and pregnancy outcomes in the general transplant population.
-
Long-term outcomes of two-dose alemtuzumab induction in pediatric kidney transplantationoa
Graphical Abstract
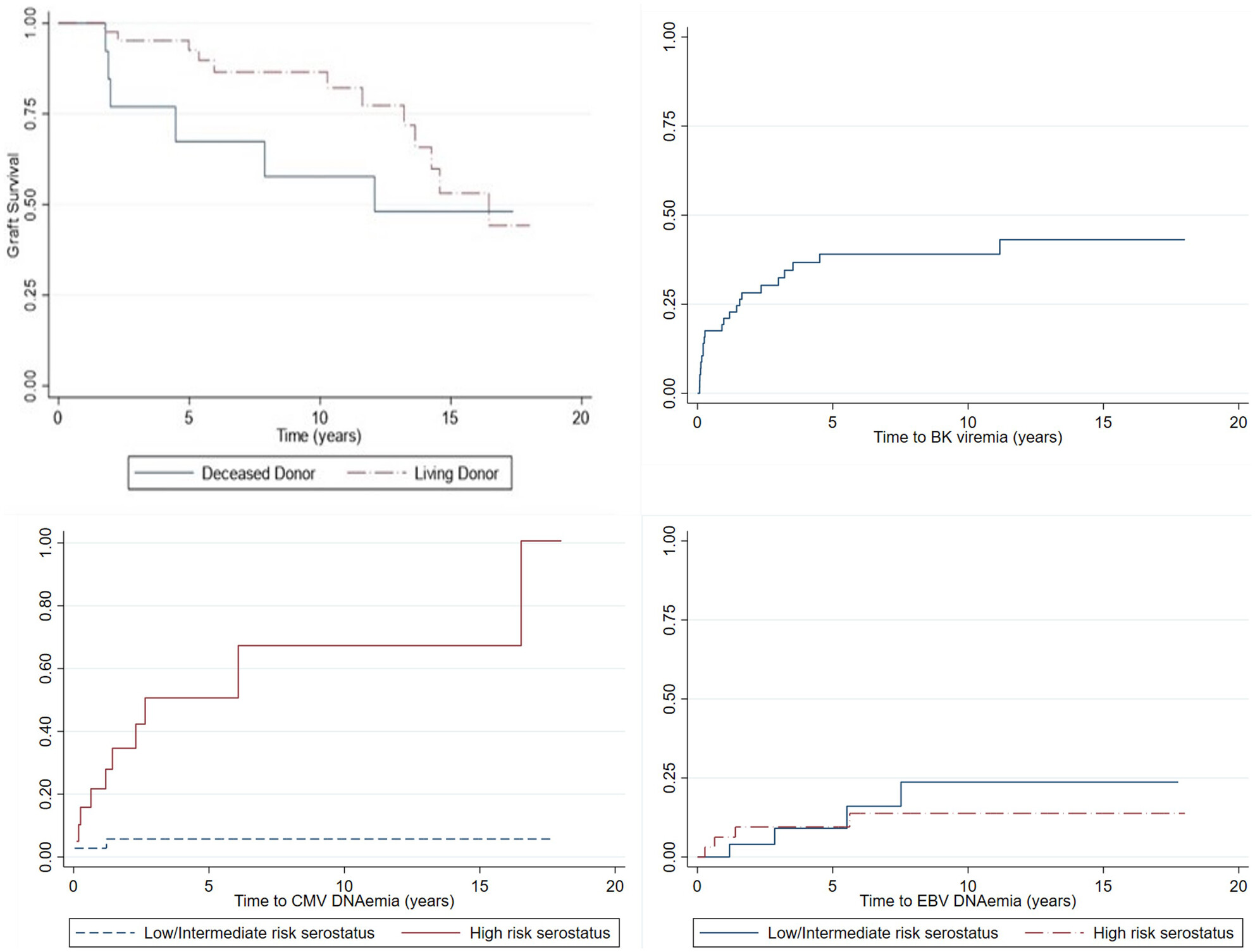
Pediatric kidney transplant recipients given two doses of alemtuzumab induction immunosuppression, with steroid-free maintenance immunosuppression, had a ten-year living-donor graft survival of 86.5% and a deceased donor graft survival of 57.7%. The incidence of viral infections was similar to that reported in other cohorts, and growth improved after transplant.
-
A novel approach to reducing hepatotoxicity related to fungal prophylaxis in pediatric lung transplant recipientsno
Graphical Abstract
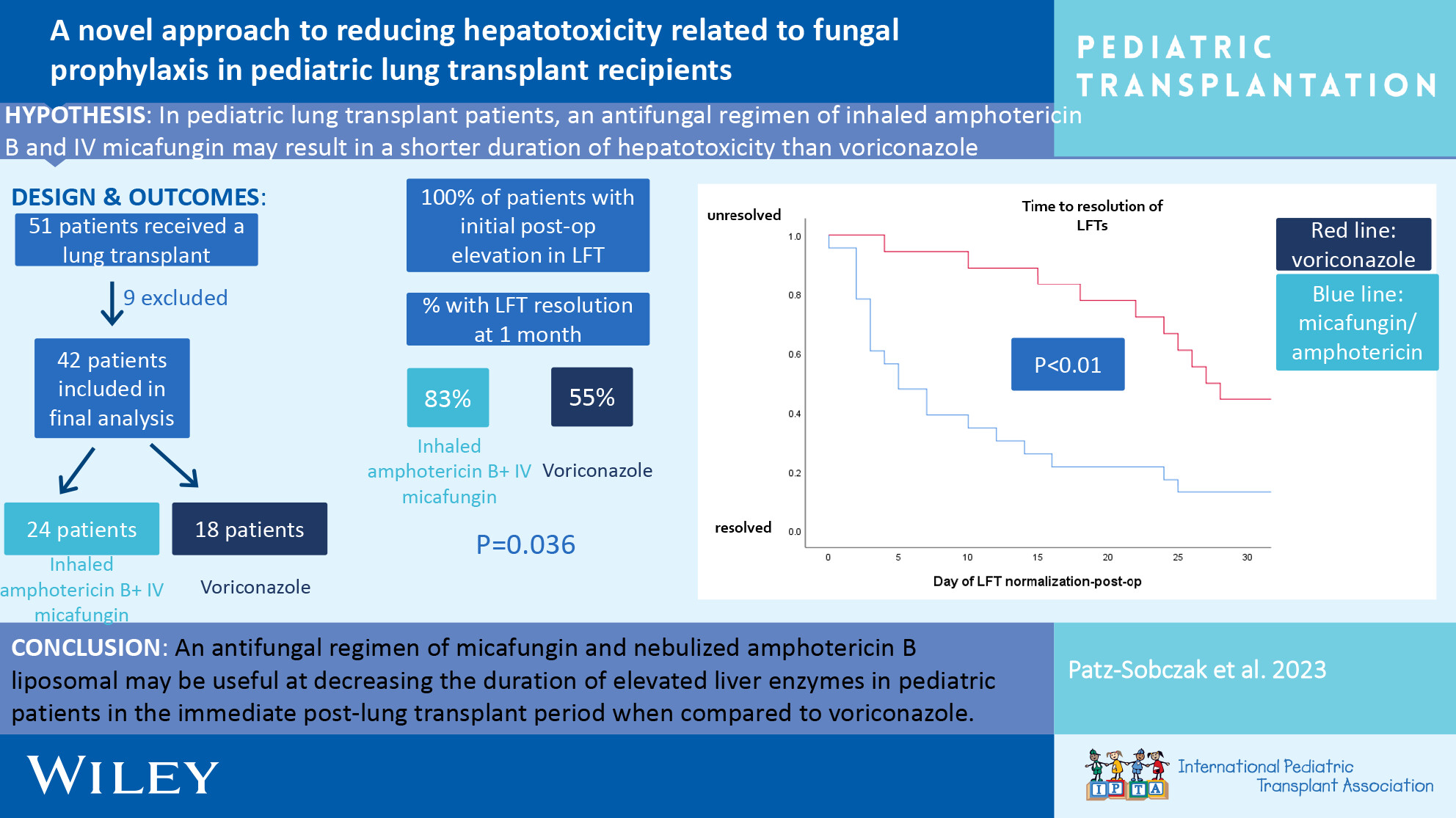
An antifungal regimen of micafungin and nebulized amphotericin B liposomal may be useful at decreasing the duration of elevated liver enzymes in pediatric patients in the immediate post-lung transplant period when compared to voriconazole monotherapy.
-
Antibody-mediated rejection in pediatric kidney transplant recipients: A report from the Pediatric Nephrology Research Consortiumno
Graphical Abstract
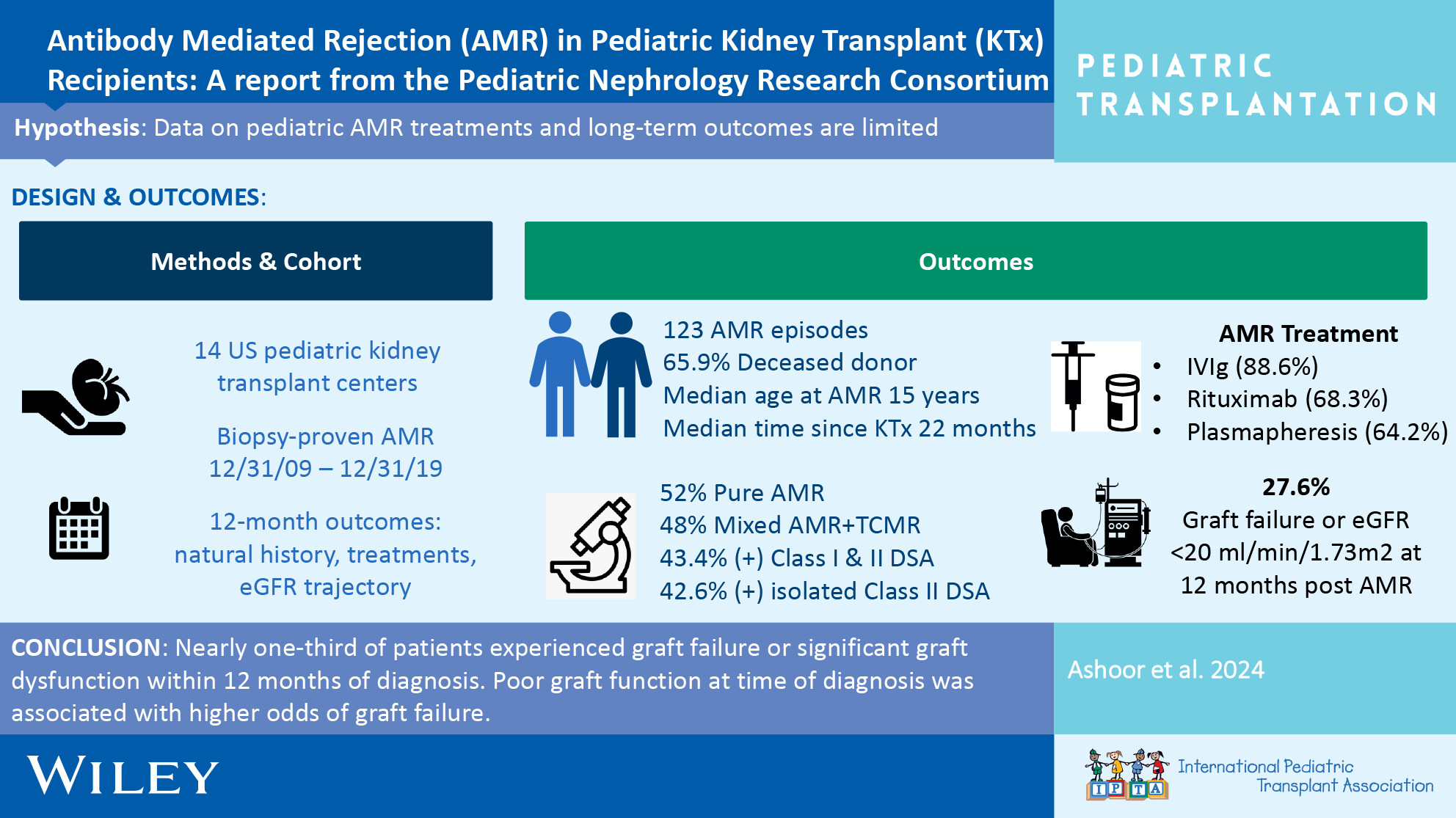
In this large cohort of pediatric kidney transplant recipients with antibody mediated rejection, nearly one-third of patients experienced graft failure or significant graft dysfunction within 12 months of diagnosis. Poor graft function at time of diagnosis was associated with higher odds of graft failure.
-
Effect of pre-emptive rituximab on EBV DNA levels and prevention of post-transplant lymphoproliferative disorder in pediatric kidney transplant recipients: A case series from the pediatric nephrology research consortiumno
Graphical Abstract
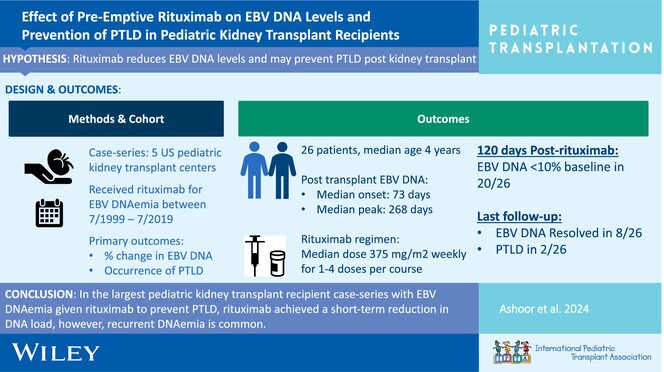
In the largest pediatric kidney transplant recipient case series with EBV DNAemia given rituximab to prevent PTLD, rituximab achieved a short-term reduction in DNA load; however, recurrent DNAemia is common.
-
Optimizing the approach to monitoring allograft inflammation using serial urinary CXCL10/creatinine testing in pediatric kidney transplant recipientsoa
Graphical Abstract
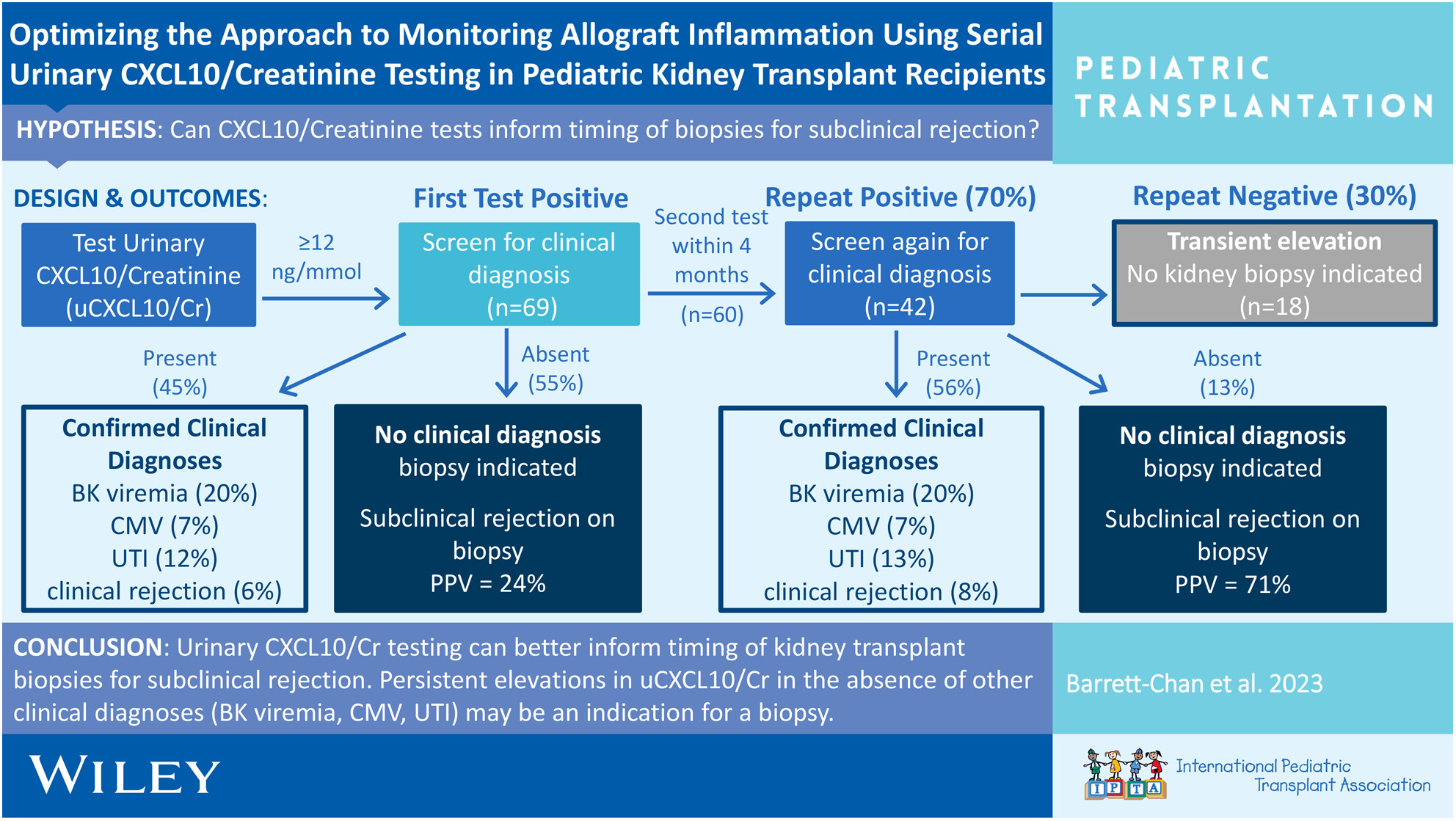
Urinary CXCL10/creatinine (uCXCL10/Cr) is an effective biomarker in pediatric kidney transplant recipients for reliably identifying kidney allograft inflammation. This study modelled the clinical implementation of this test and supported a two-test approach to reliably exclude other clinically identifiable sources of inflammation, for kidney biopsy indication to rule-out subclinical rejection.
-
Leflunomide as adjunct therapy for BK viremia management in pediatric kidney transplant recipientsno
Graphical Abstract
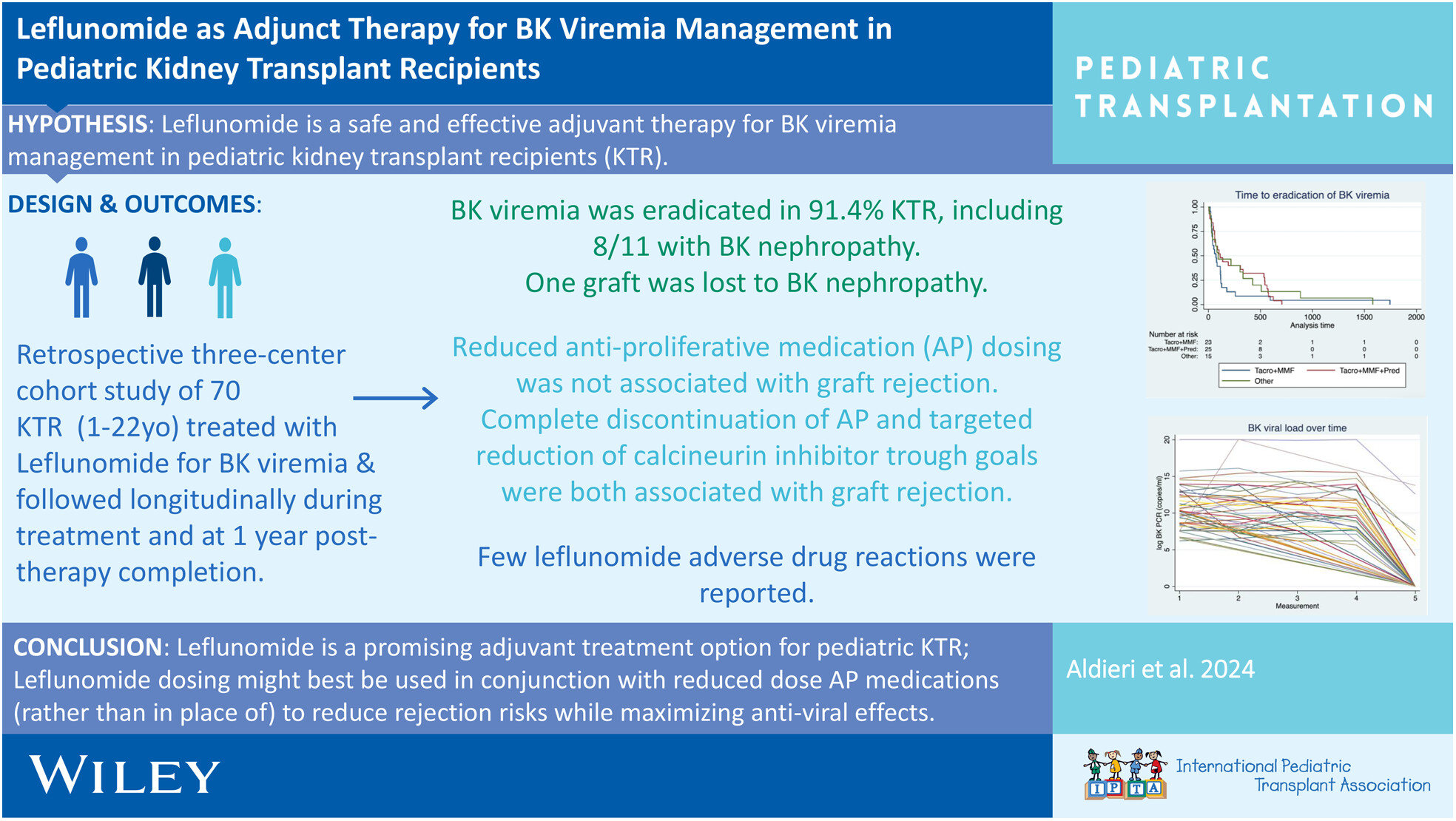
Leflunomide is a promising adjunctive treatment for BK virus eradication and prevention of BK nephropathy, along with IS reduction, particularly anti-proliferative immunosuppression reduction, without significant risk for the development of biopsy-proven rejection in pediatric kidney transplant recipients. Given the significant risk for the development of biopsy-proven rejection with complete AP discontinuation and CNI reduction in our study cohort, we suggest anti-proliferative reduction, not discontinuation, and judicious reduction in CNI trough goals with close monitoring as a strategy for treatment of BK viremia with concomitant use of leflunomide therapy.