

Journal list menu

 Issue
IssueClinical & Experimental Immunology: Volume 187, Issue 1
Special Issue:Ageing and the immune system, effects of immunosenescence and clinical implications
1-184January 2017
Export Citations
Download PDFs
Editorial
Ageing and the immune system, effects of immunosenescence and clinical implications
Immunosenescence: the importance of considering age in health and disease
- Pages: 1-3
- First Published: 18 December 2016
Commentary
Ageing and the immune system, effects of immunosenescence and clinical implications
The convergence of senescence and nutrient sensing during lymphocyte ageing
- Pages: 4-5
- First Published: 30 September 2016
Review Articles
Ageing and the immune system, effects of immunosenescence and clinical implications
Immune senescence: significance of the stromal microenvironment
- Pages: 6-15
- First Published: 16 August 2016
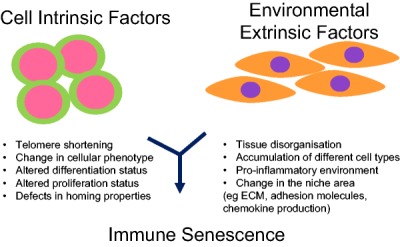
Whilst the exact mechanisms underlying immunosenescence are still unclear, several studies have identified intrinsic defects within many of the cells of the immune system. Despite the stromal niche playing a critical role in the development, maintenance and activation of immune cells the role of the microenvironment in immunosenescence remains an overlook area, but is increasingly becoming recognised as playing an important role in the decline of immune function in the aged.
Innate immune responses in the ageing lung
- Pages: 16-25
- First Published: 06 October 2016
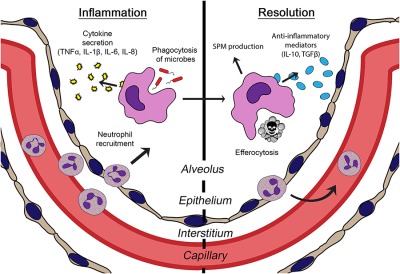
The elderly are a growing demographic at high risk for respiratory infections due to innate immune dysfunction in the lungs. In this review, we examine research on age-related changes in the response of the innate immune system to pulmonary infections.
Age-related alterations in immune responses to West Nile virus infection
- Pages: 26-34
- First Published: 10 September 2016
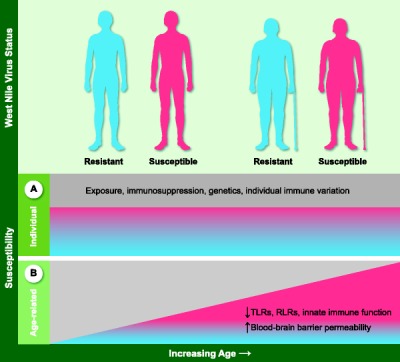
West Nile virus (WNV) is the most important causative agent of viral encephalitis worldwide and is an important public health concern in the USA due to its high prevalence, severe disease, and the absence of effective treatments. Individual host factors play a role in susceptibility to WNV infection, but age is the most well-defined risk factor for susceptibility to severe disease. Understanding the specific immune parameters and mechanisms that influence susceptibility to symptomatic WNV may lead to a better understanding of increased susceptibility in elderly individuals.
Intracellular signalling pathways: targets to reverse immunosenescence
- Pages: 35-43
- First Published: 01 July 2016
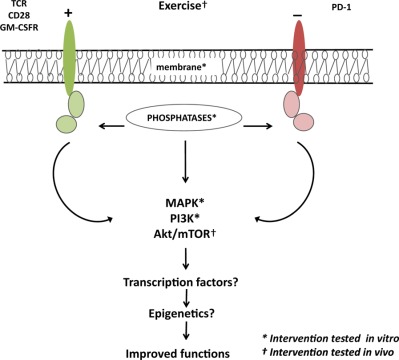
Alterations to immune cell signaling may be a prominent cause of malfunctioning immunity with aging. Emerging attempts to reverse immunosenescence have recently targeted the signaling pathways in various different cell types of the immune system. Here, we review and discuss alterations in the signaling pathways of immune cells with aging and consider current targets and means to modulate altered functions.
Ageing and inflammation in patients with HIV infection
- Pages: 44-52
- First Published: 20 May 2016
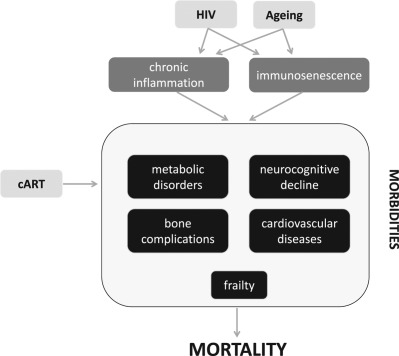
HIV+ patients can present neurocognitive disorders, cardiovascular diseases, metabolic syndrome, bone abnormalities, and non-HIV associated cancers. Chronic inflammation and immune activation that are typically observed in elderly people and were defined “inflammaging” can be present in HIV+ patients, who experience a sort of premature aging, which affects heavily the quality of life. Main factors have been identified beside the traditional behavioral risk factors, that are the toxicity of antiretroviral treatments and chronic inflammation, leading to a functional decline and a vulnerability to injury or pathologies.
Considerations for successful cancer immunotherapy in aged hosts
- Pages: 53-63
- First Published: 30 September 2016
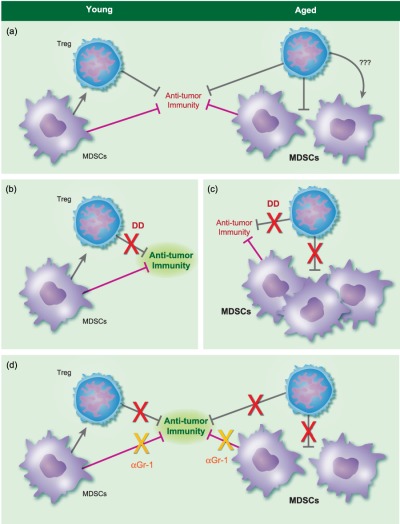
This is a comprehensive review of age effects on responses to cancer immunotherapy.
Ageing and obesity similarly impair antibody responses
- Pages: 64-70
- First Published: 17 June 2016
The life cycle of a T cell after vaccination – where does immune ageing strike?
- Pages: 71-81
- First Published: 20 June 2016
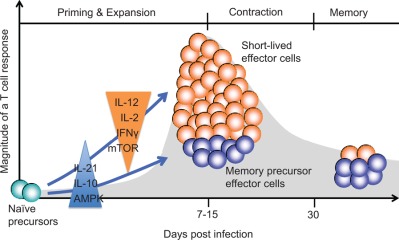
T cell responses to vaccinations are a staged process starting with activation of antigen-specific T cells followed by expansion and differentiation into short-lived effector and memory precursor cells and then attrition with memory precursor cells surviving as long-lived memory T cells. Each of these stages is regulated by T cell-extrinsic as well as T cell-intrinsic mechanisms, several of which have been shown to be affected by immune aging and therefore represent promising targets for immune intervention to enhance the benefit from vaccination in an older population.
Herpes zoster and the search for an effective vaccine
- Pages: 82-92
- First Published: 10 May 2016
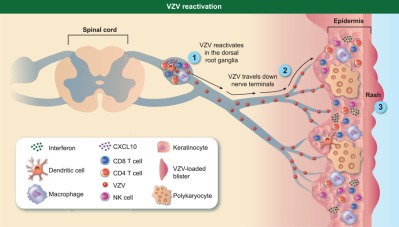
Herpes Zoster is a painful and debilitating disease caused by the reactivation of Varicella Zoster Virus (VZV), the causative agents of chicken pox. This review summarizes our current understanding of the virus life cycle, the immune response during both chickenpox and herpes zoster.
We then review vaccines against herpes zoster that have been approved and those that are in the pipeline. Finally, we discuss animal models that can be used to develop novel vaccine strategies and gain additional insight into interactions between host and VZV.
Adult vaccination against tetanus and diphtheria: the European perspective
- Pages: 93-99
- First Published: 09 June 2016
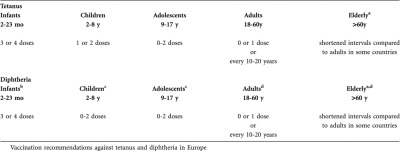
Besides immunizations against influenza, Streptococcus pneumoniae and herpes zoster, which are recommended specifically for the elderly regular booster vaccinations against tetanus, diphtheria and in some cases pertussis and polio are recommended in many European countries for adults including the elderly. Vaccination recommendations for adults differ greatly between individual countries. Tetanus-specific antibody concentrations are generally higher than diphtheria-specific antibodies, and a substantial proportion of adults, and particularly of the elderly do not have protective antibody concentrations against diphtheria. Antibody levels increase upon booster vaccination in all age groups, but diphtheria-specific antibody concentrations remain below protective levels in some older individuals even immediately after vaccination and long-term protection is frequently not achieved. Future vaccination strategies should therefore include regular and well-documented booster shots e.g. against tetanus and diphtheria throughout life.
Original Articles
Translational
Allergy
Impaired virus replication and decreased innate immune responses to viral infections in nasal epithelial cells from patients with allergic rhinitis
- Pages: 100-112
- First Published: 26 September 2016

The study demonstrated impaired immune response to viral infections in nasal epithelial cells (NECs) from allergic rhinitis patients. Significant differences in viral proliferation and innate response to parainfluenza type 3 (PIV3) and to a lesser extent to rhinovirus 1B (RV1B) in NECs from atopic donors as compared to healthy individuals have been shown.
Autoimmunity
Tolerogenic dendritic cells generated with dexamethasone and vitamin D3 regulate rheumatoid arthritis CD4+ T cells partly via transforming growth factor-β1
- Pages: 113-123
- First Published: 26 September 2016

We report that tolerogenic dendritic cells generated with dexamethasone and vitamin D3 express the immunoregulatory cytokine TGF-β1. Despite CD4+ T-cells from rheumatoid arthritis patients being measurably less responsive to TGF-β1 they can nonetheless be efficiently regulated by tolDC in a TGF-β1-dependent manner.
Cancer
Human leucocyte antigen class I-redirected anti-tumour CD4+ T cells require a higher T cell receptor binding affinity for optimal activity than CD8+ T cells
- Pages: 124-137
- First Published: 20 June 2016
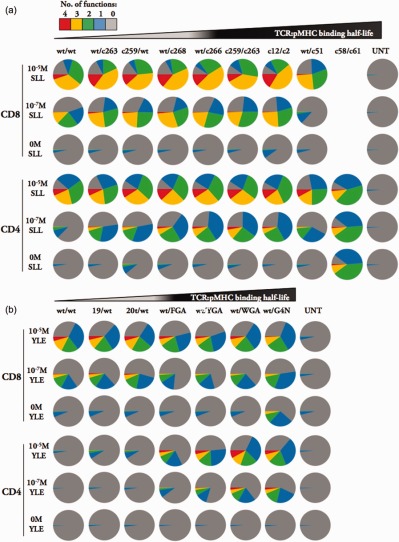
Since both CD4+ and CD8+ T-cell responses are believed to be beneficial for tumour clearance, it could be advantageous to include HLA-I-redirected CD4+ T-cells in adoptive cell transfer regimes in addition to CD8+ T-cells. Comparison of primary CD4+ and CD8+ T-cells expressing wildtype and a range of affinity-enhanced TCRs specific for the HLA A*0201-restricted NY-ESO-1- and gp100 tumour antigens shows that redirected primary CD4+ T-cells expressing TCRs of sufficiently high affinity exhibit a wide range of effector functions, including cytotoxicity, in response to cognate peptide; and that optimal TCR binding affinity is higher in CD4+ T-cells than CD8+ T-cells. Our results suggest that the most beneficial therapy might involve engineered CD4+ and CD8+ T-cells expressing different TCRs with the appropriate TCR:pMHC affinities to allow optimal, synergistic function of both T cell subsets.
Immunodeficiency
FDG PET-CT imaging of therapeutic response in granulomatous lymphocytic interstitial lung disease (GLILD) in common variable immunodeficiency (CVID)
- Pages: 138-145
- First Published: 28 November 2016
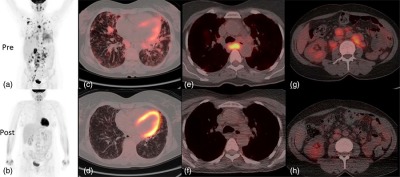
The Figure shows combined 2-[(18)F]-fluoro-2-deoxy-d-glucose positron emission tomography and computed tomography (FDG PET-CT) scanning for the assessment and monitoring of response to treatment in GLILD. The synergistic combination of functional and anatomical imaging in GLILD demonstrates a widespread and high level of metabolic activity in the lungs and lymph nodes. Following treatment with rituximab and mycophenolate there was almost complete resolution of the high metabolic activity alongside significant normalisation in lymph node size and lung architecture.
Efficacy, safety, tolerability and pharmacokinetics of a novel human immune globulin subcutaneous, 20%: a Phase 2/3 study in Europe in patients with primary immunodeficiencies
- Pages: 146-159
- First Published: 10 September 2016
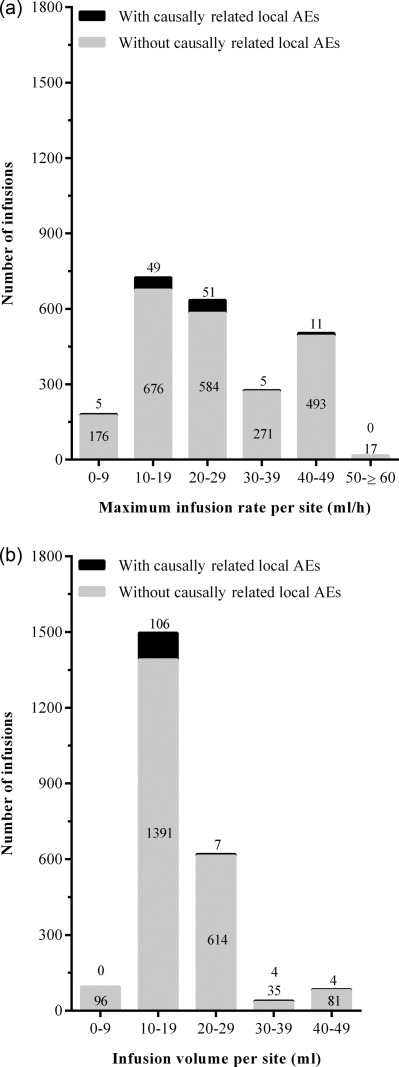
In 94.8% of IGSC 20% infusions (n=2338) administered to patients with PIDD in this European study, no causally related local AE occurred.
Higher infusion rates or infusion volumes per site were not associated with an increased incidence of causally related local AEs. IGSC 20% provided an effective and well-tolerated therapy for patients previously on intravenous or subcutaneous treatment, with no dose adjustment.
Infectious disease
Mycobacterium tuberculosis multi-drug-resistant strain M induces IL-17+IFNγ– CD4+ T cell expansion through an IL-23 and TGF-β-dependent mechanism in patients with MDR-TB tuberculosis
- Pages: 160-173
- First Published: 28 September 2016
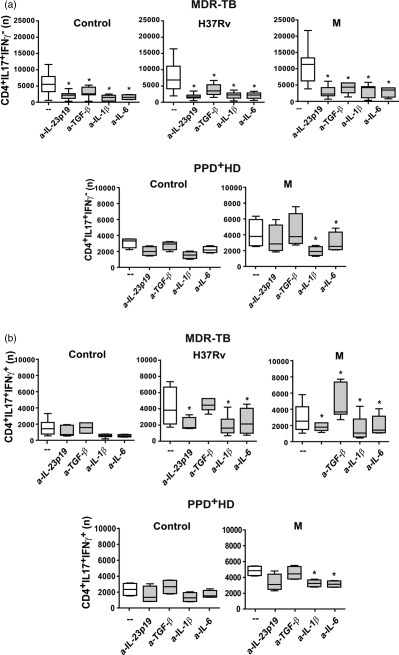
M. tuberculosis (Mtb) multidrug resistant strain M induces differential expansion of IL-17+ T cell subsets in patients with MDR-TB: IL-1β and IL-6 secreted by Mtb stimulated APCs are crucial for IL-17 secretion and IL-17+ T cell expansion in MDR-TB and PPD+ healthy donors (HD). Particularly, in PPD+HD, Mtb induce the expansion of IL-17+IFNγ+ cells through a TLR-4 and IL-23-dependent mechanism, independent of the strain. In the case of MDR-TB patients, recognition of MDR strain M via TLR2 induces APCs and CD4+ T cells binding LAP/TGF-β complex (LAP) to secrete large amounts of TGF-β that, in concert with IL-23, supports the expansion of IL-17+IFNγ− CD4+ T cells which are responsible for the high Th17 response observed in MDR-TB patients.
Inflammation
MicroRNA-26a–interleukin (IL)-6–IL-17 axis regulates the development of non-alcoholic fatty liver disease in a murine model
- Pages: 174-184
- First Published: 05 July 2016
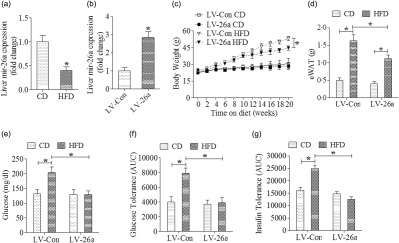
Mir-26a-IL-6-IL-17 axis regulates the development of NAFLD in a murine model.
Sign up for email alerts
Tools
An Official Journal of the British Society for Immunology
More from this journal
Visit the British Society for Immunology on Social Media:
![]()
![]()
![]()
![]()
![]()
ALSO VISIT Clinical & Experimental Immunology App