


All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Bortezomib for antibody-mediated rejection of kidney transplant in youth: Associations with donor-specific antibodyno
Graphical Abstract
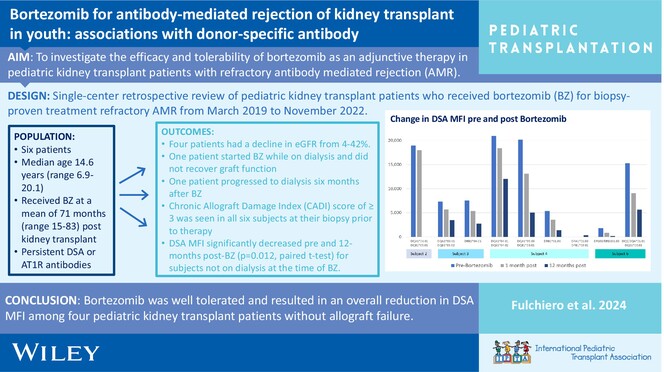
Bortezomib was well tolerated as an adjunctive therapy in four pediatric kidney transplant patients with refractory antibody-mediated rejection and persistent donor-specific antibodies and resulted in an overall statistically significant reduction in DSA MFI.
-
Treatment outcome at the pediatric stem cell transplantation center in Syria: A single-center experienceno
Graphical Abstract
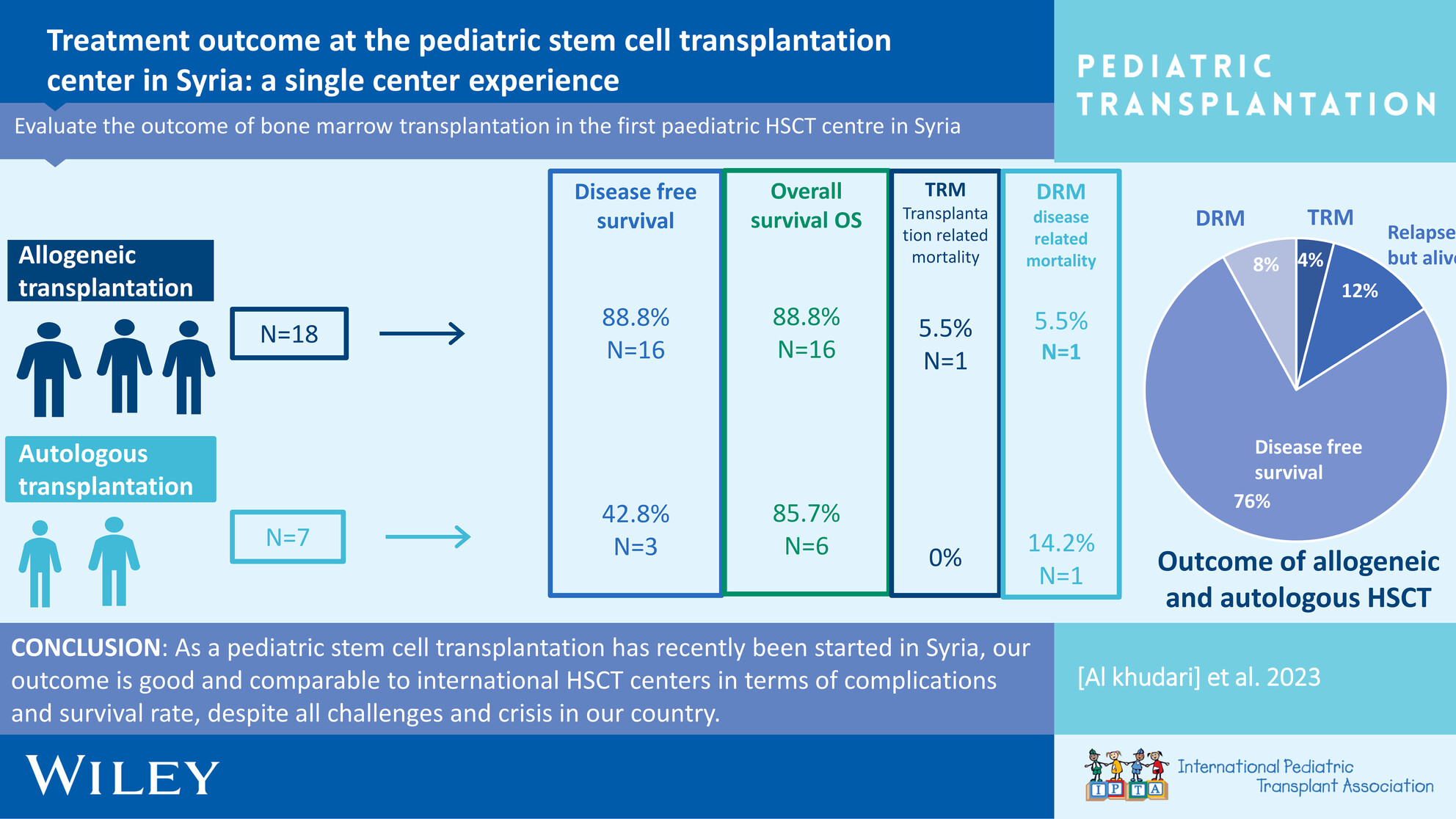
In autologous patients, transplant-related mortality (TRM) was 0%, with 4 (57%) experiencing disease relapse, resulting in the death of one patient. Additionally, 3 (42.8%) of patients remain alive under second-line management. The overall survival rate was 6 (85.7%), and the disease-free survival rate was 16 (88%). In allogeneic patients, TRM was 5.5% (1/18). One allogeneic patient experienced disease relapse and subsequently died. The overall survival rate and disease-free survival rate were 16 (88%). The objective of this study was to assess the outcomes of pediatric hematopoietic stem cell transplantation (HSCT) patients who have undergone transplantation thus far.
-
Adrenal insufficiency in pediatric kidney transplantation recipientsoa
Graphical Abstract
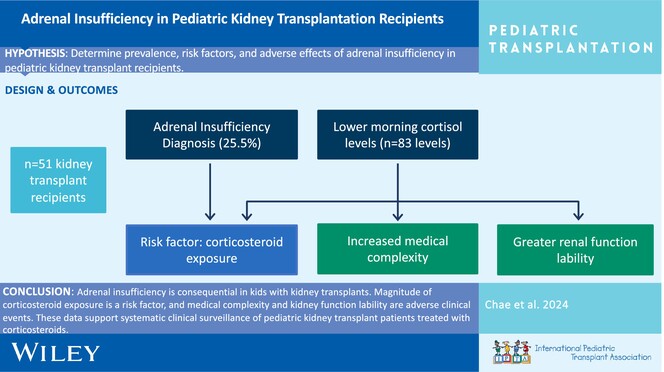
Adrenal insufficiency is common in pediatric kidney transplant recipients. Corticosteroid exposure is a risk factor, and medical complexity and kidney function lability are adverse clinical outcomes. These data support systemic clinical surveillance of adrenal insufficiency in pediatric kidney transplant recipients treated with corticosteroids.
-
Calcineurin inhibitor-related hyperkalemia is caused by hyporeninemic hypoaldosteronism and fludrocortisone is an effective treatment: Report of a case series and review of the literatureno
Graphical Abstract
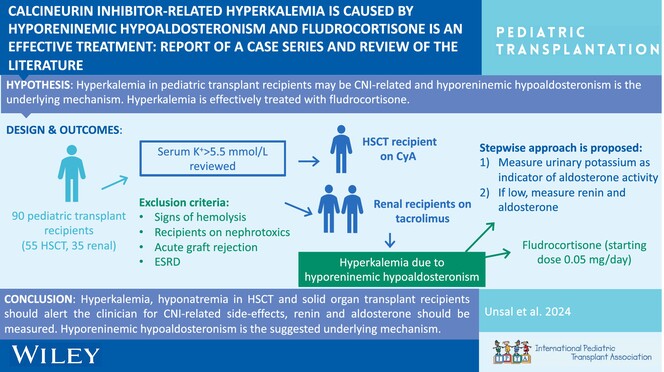
Hyperkalemia and hyponatremia in HSCT and solid organ transplant recipients should alert the clinician for CNI-related side effects; renin and aldosterone should be measured. Hyporeninemic hypoaldosteronism is the suggested underlying mechanism.
-
Alemtuzumab induction is associated with decreased hospitalization rates in pediatric kidney transplant: A UNOS data review for safety and outcomes with common induction regimensno
Graphical Abstract
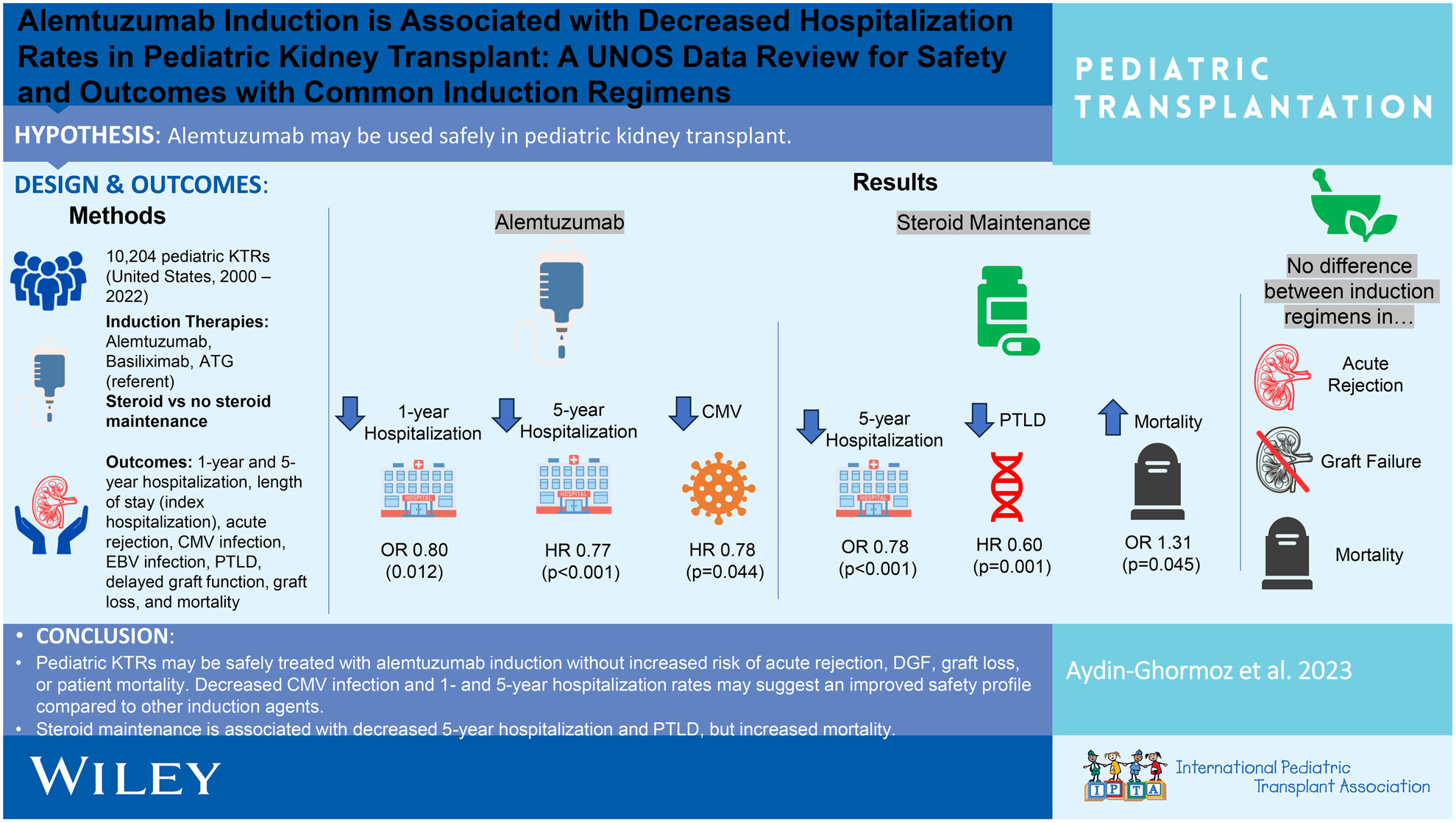
Pediatric KTRs may be safely treated with alemtuzumab induction without increased acute rejection, delayed graft function, graft loss, or patient mortality, but with decreased CMV infection and 1 and 5 years hospitalization rates. Steroid maintenance is associated with decreased 5 years hospitalization and PTLD, but increased mortality.
-
Changes in thoracic radio density after living donor liver transplantationno
Graphical Abstract
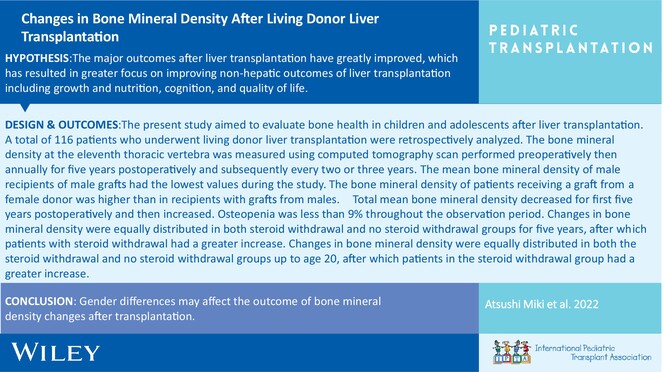
Abstract of changes in thoracic radio density after living donor liver transplantation
-
Pregnancy after transplant in the older adolescent: Anticipatory guidance for the pediatric providernoCollections: Special Issue on Adolescence and Transplantation
Graphical Abstract
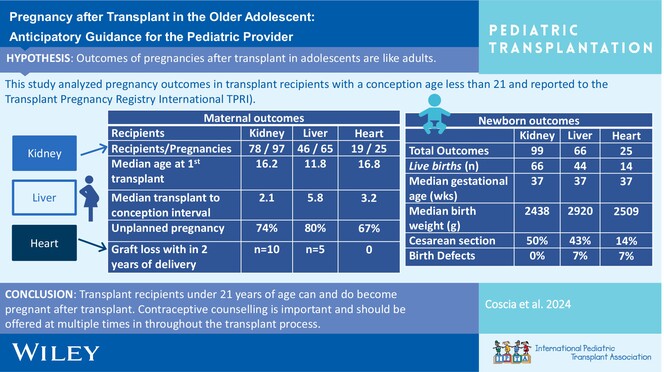
This manuscript will provide a brief review of current recommendations for contraception for adolescent and young adult solid organ transplant recipients, a short review of immunosuppression and pregnancy exposure, overview of outcomes in recipients who had a pregnancy before age 21 years, and pregnancy outcomes in the general transplant population.
-
COVID-19 disease in children and adolescents following allogeneic hematopoietic stem cell transplantation: A report from the Turkish pediatric bone marrow transplantation study groupno
Graphical Abstract
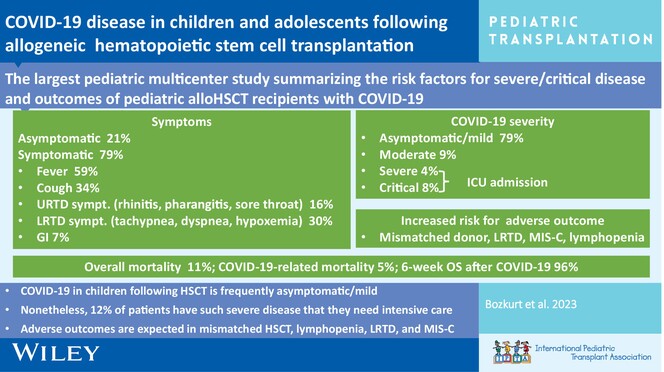
COVID-19 in children following HSCT is frequently asymptomatic/mild. Nonetheless, 12% of patients have such severe disease that they need intensive care. Adverse outcomes are expected in mismatched HSCT, lymphopenia, LRTD, and MIS-C.
-
Long-term outcomes of two-dose alemtuzumab induction in pediatric kidney transplantationoa
Graphical Abstract
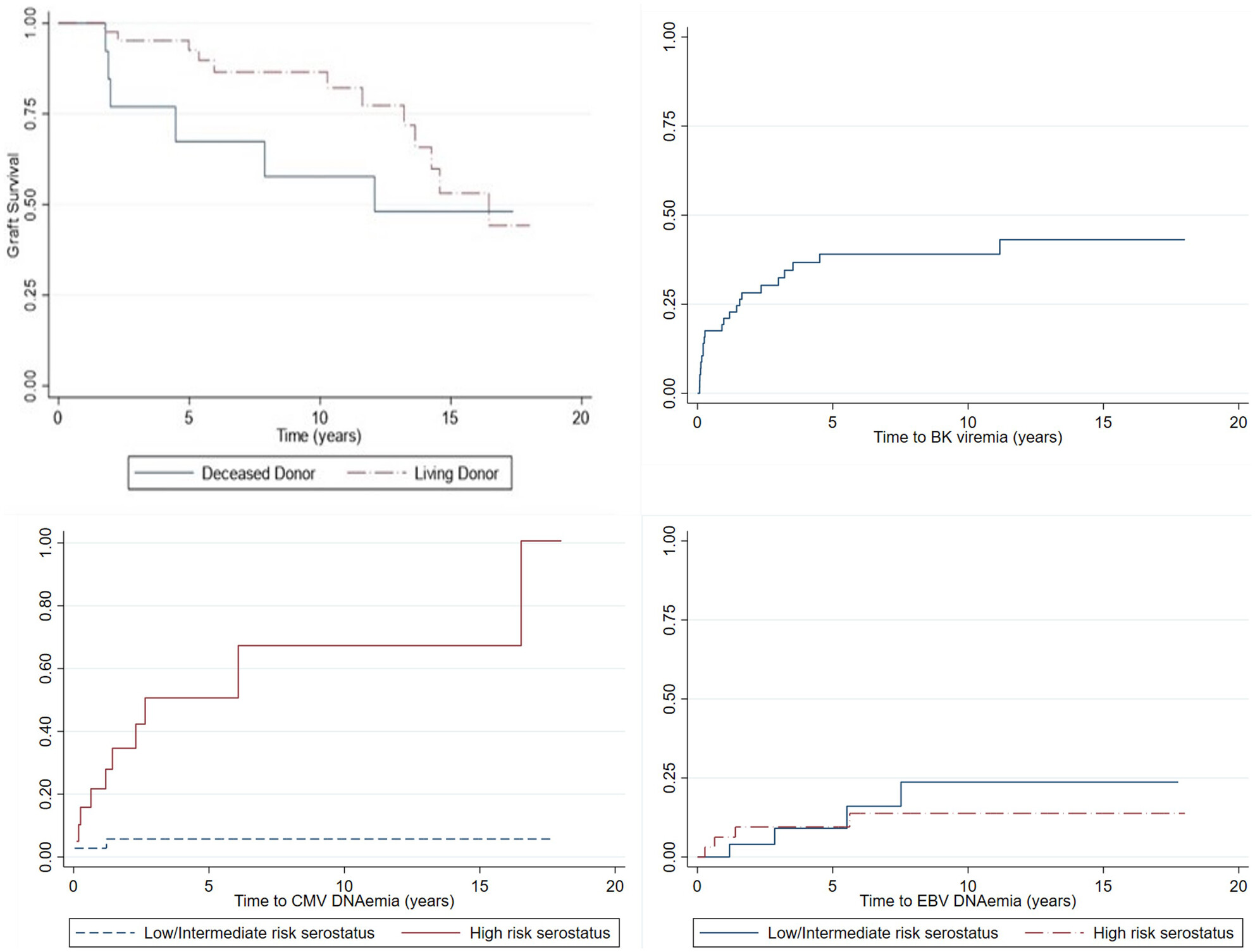
Pediatric kidney transplant recipients given two doses of alemtuzumab induction immunosuppression, with steroid-free maintenance immunosuppression, had a ten-year living-donor graft survival of 86.5% and a deceased donor graft survival of 57.7%. The incidence of viral infections was similar to that reported in other cohorts, and growth improved after transplant.
-
Long-term outcome of pediatric renal transplantation with donors younger than 6 yearsno
Graphical Abstract
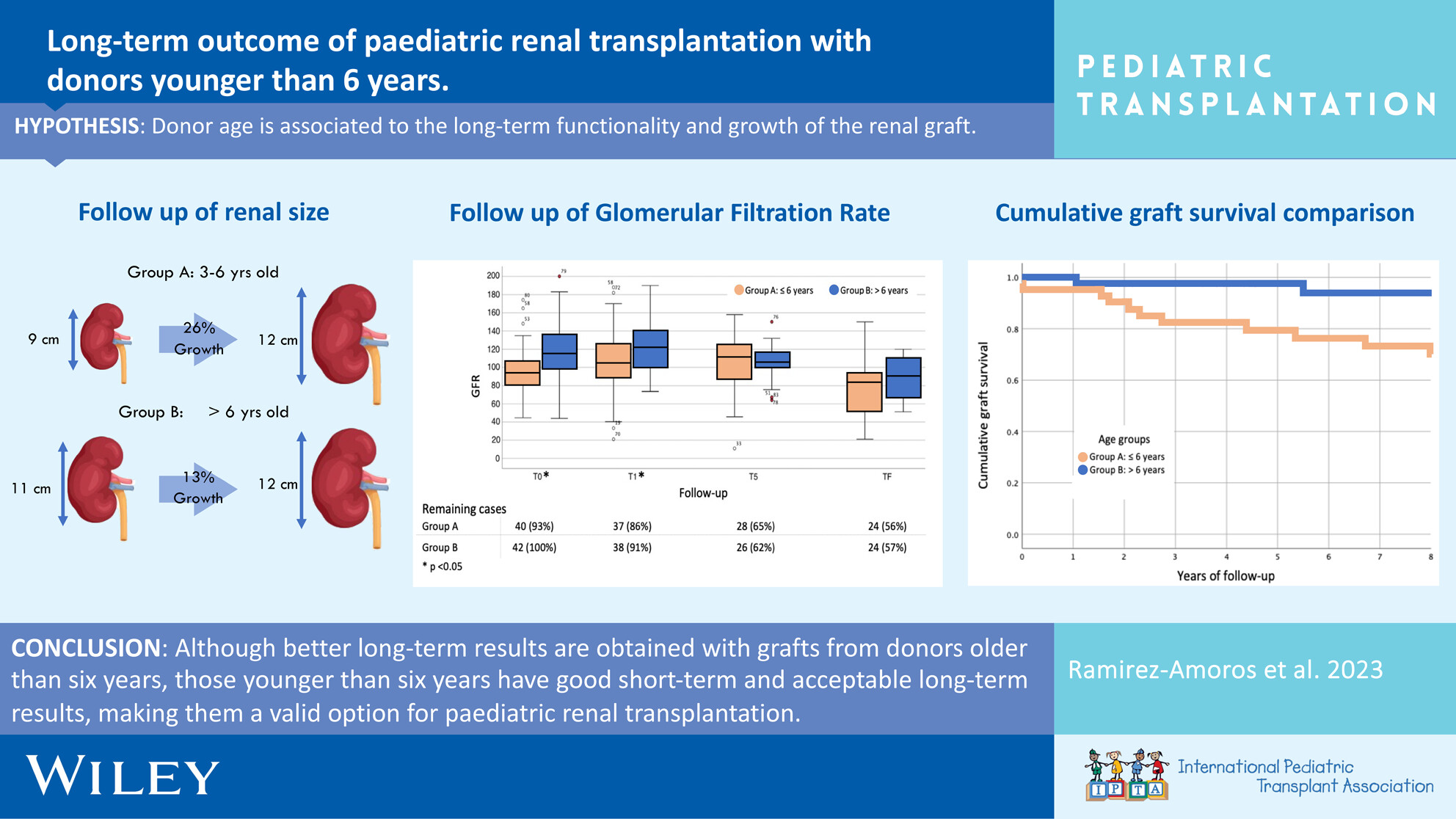
Donor age is associated to the long-term functionality and growth of renal grafts in pediatric transplantation. Although better long-term results are obtained with grafts from donors older than 6 years, those younger than 6 years have good short-term and acceptable long-term results, making them a valid option for pediatric renal transplantation.
-
A novel approach to reducing hepatotoxicity related to fungal prophylaxis in pediatric lung transplant recipientsno
Graphical Abstract
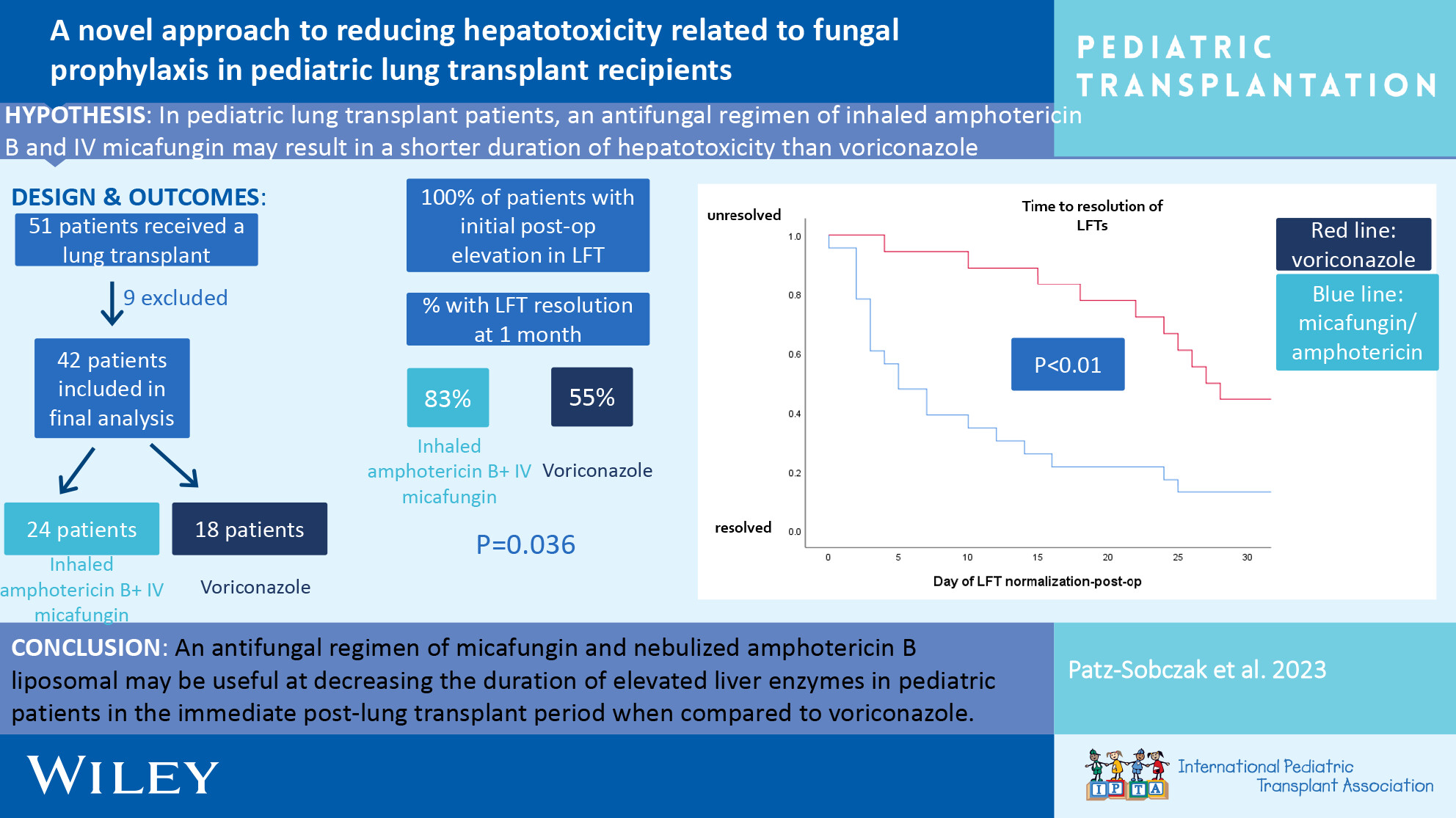
An antifungal regimen of micafungin and nebulized amphotericin B liposomal may be useful at decreasing the duration of elevated liver enzymes in pediatric patients in the immediate post-lung transplant period when compared to voriconazole monotherapy.
-
Let's get physical: Aerobic capacity, muscle strength, and muscle endurance after pediatric heart transplantationoa
Graphical Abstract
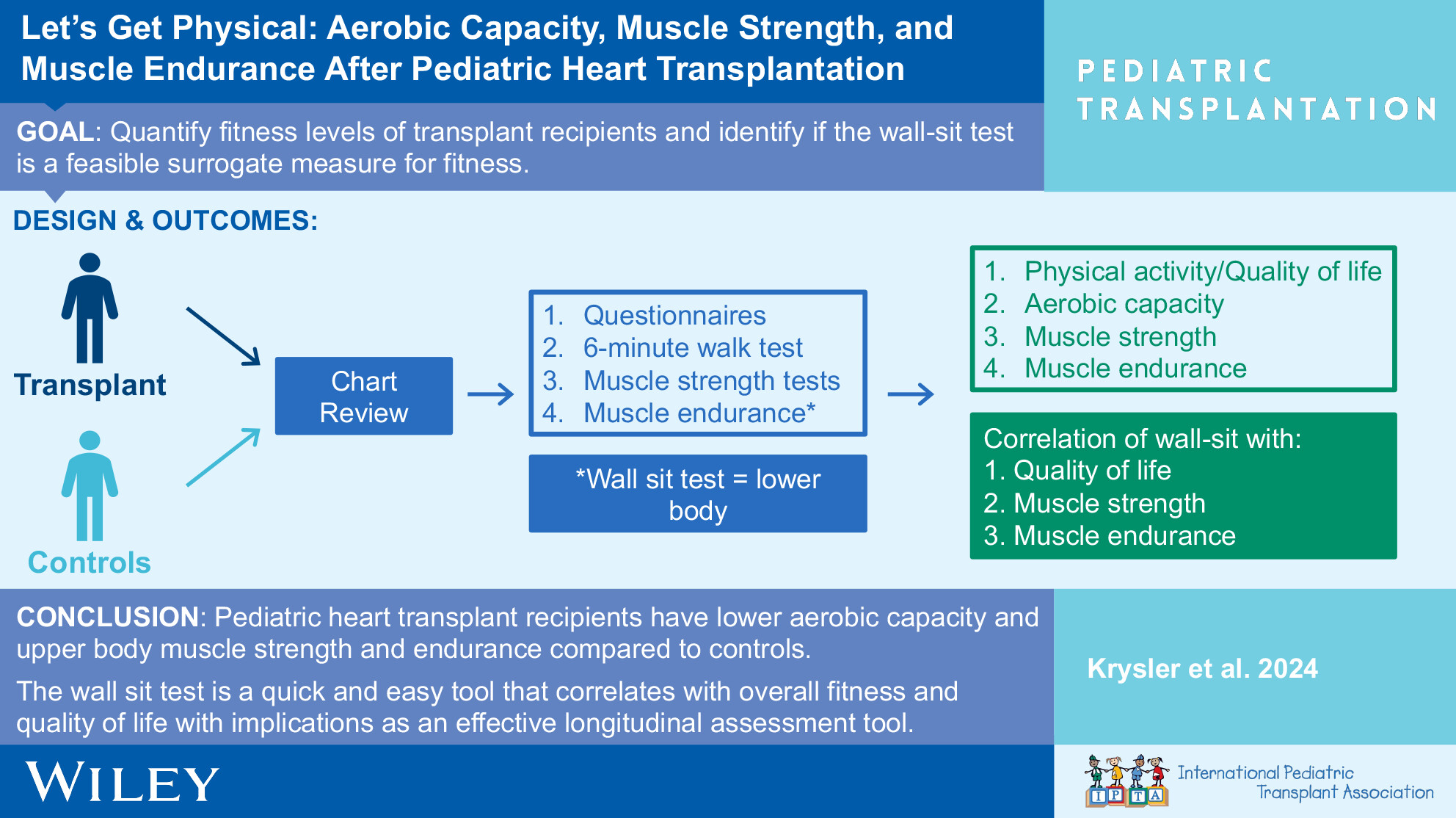
Assessment of pediatric heart transplant recipients demonstrated lower aerobic capacity and upper body muscle strength and endurance compared to healthy children. Our study suggests the wall sit test is a quick, easy tool that correlates with overall fitness and quality of life which could be utilized in clinical and research settings.
-
Haploidentical hematopoietic stem cell transplantation with busulfan, cyclophosphamide, and fludarabine conditioning for X-linked adrenal cerebral leukodystrophyno
Graphical Abstract
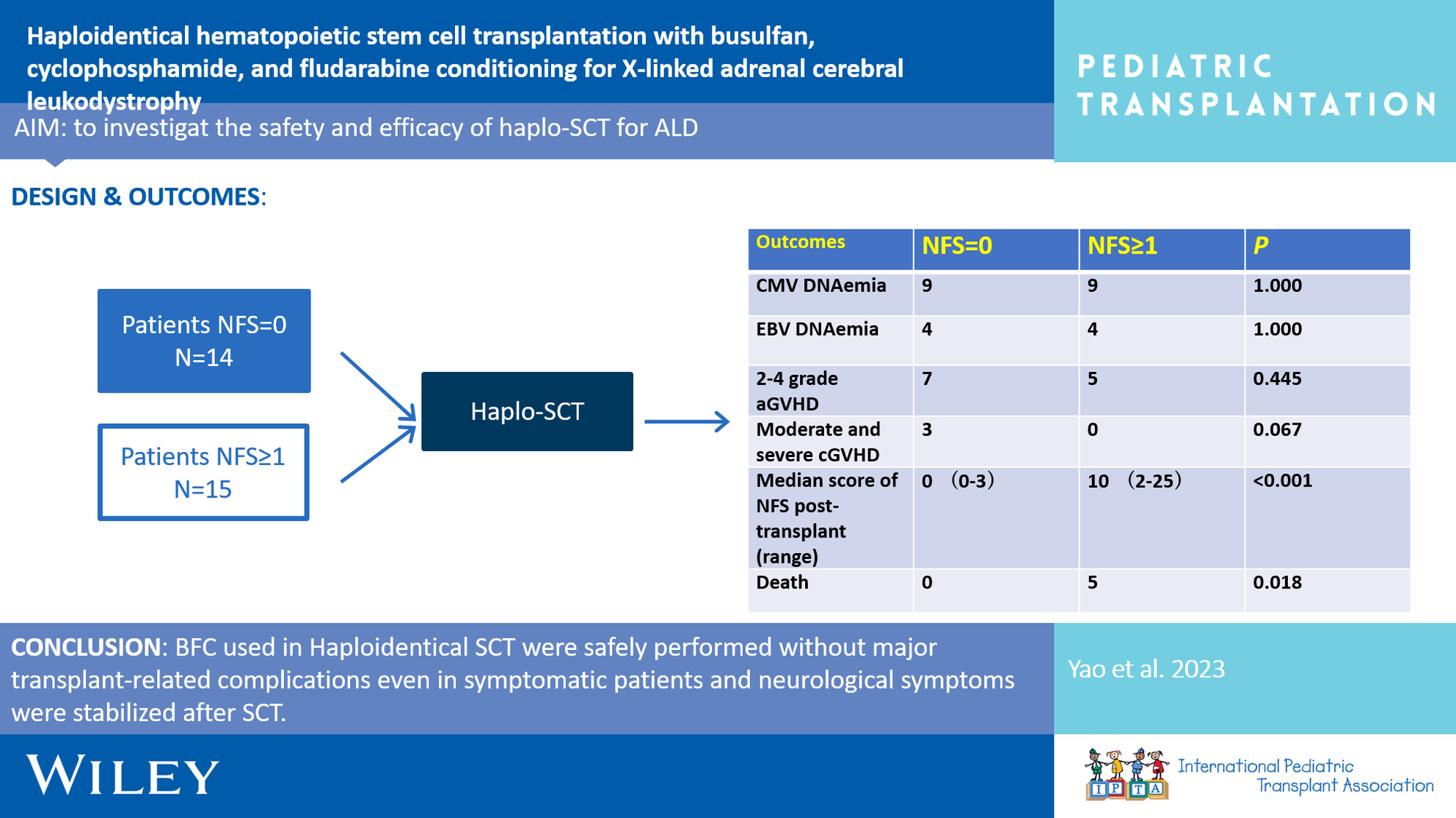
BFC regimen used in haploidentical SCT was administered safely without major transplant-related complications even in symptomatic patients, and neurological symptoms were stabilized after SCT.
-
Effect of pre-emptive rituximab on EBV DNA levels and prevention of post-transplant lymphoproliferative disorder in pediatric kidney transplant recipients: A case series from the pediatric nephrology research consortiumno
Graphical Abstract
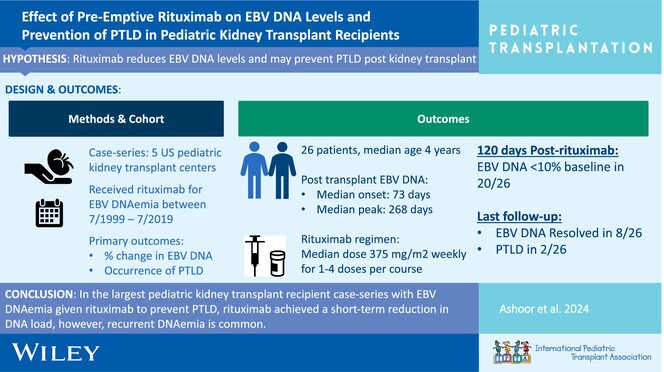
In the largest pediatric kidney transplant recipient case series with EBV DNAemia given rituximab to prevent PTLD, rituximab achieved a short-term reduction in DNA load; however, recurrent DNAemia is common.
-
Kidney transplant in pediatric gut transplant recipients – Technical challenges and outcomesno
Graphical Abstract
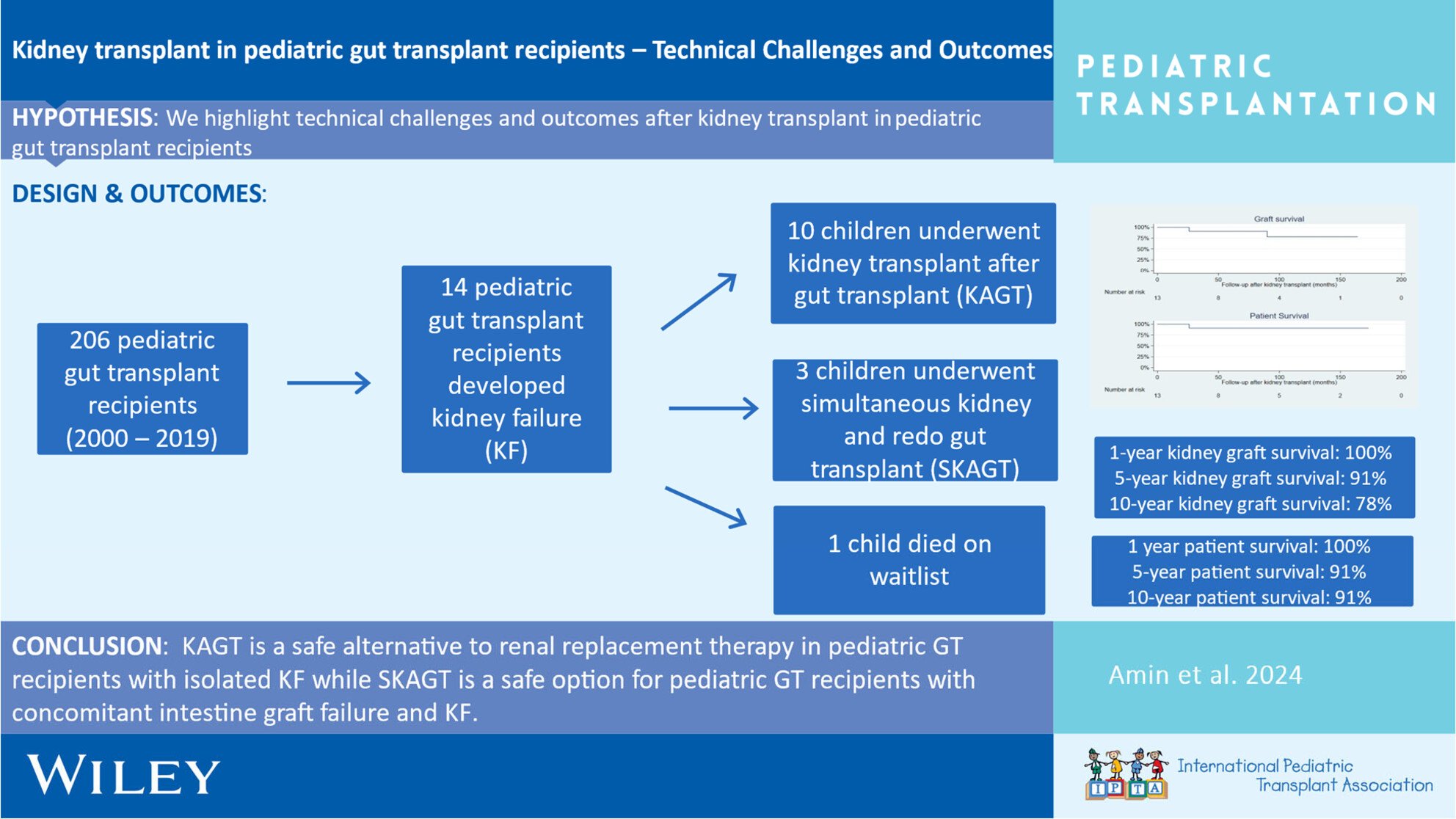
Excellent short- and long-term kidney transplant graft, gut transplant graft, and patient survival can be achieved through meticulous surgical technique and multidisciplinary peri-operative management of pediatric kidney after gut transplant recipients.
-
The humoral immune response to the BNT 162B2 vaccine in pediatrics on renal replacement therapyno
Graphical Abstract
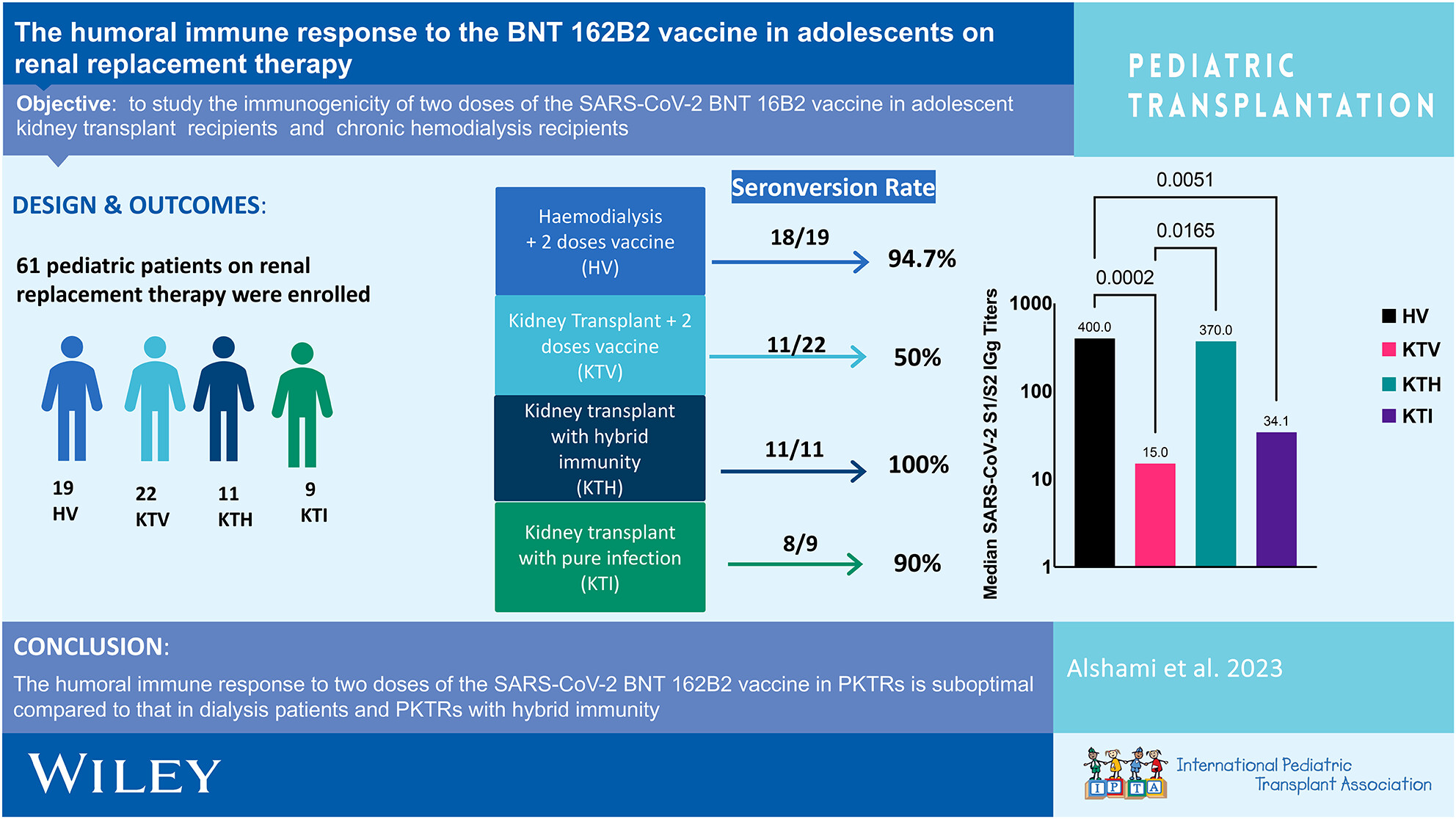
The humoral immune response to two doses of the SARS-CoV-2 BNT 162B2 vaccine in PKTRs is suboptimal compared to that in dialysis patients and PKTRs with hybrid immunity.
-
Leflunomide as adjunct therapy for BK viremia management in pediatric kidney transplant recipientsno
Graphical Abstract
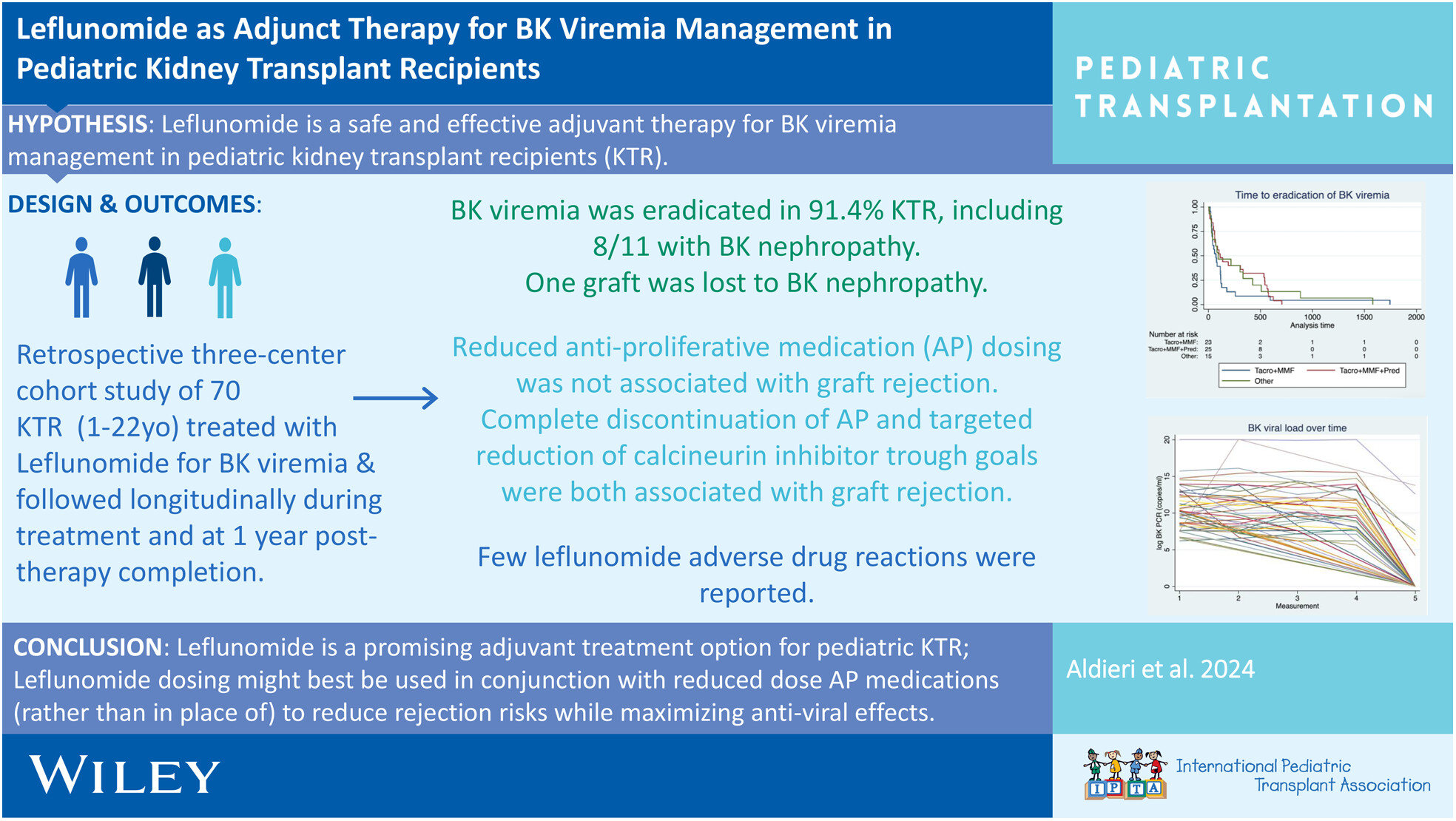
Leflunomide is a promising adjunctive treatment for BK virus eradication and prevention of BK nephropathy, along with IS reduction, particularly anti-proliferative immunosuppression reduction, without significant risk for the development of biopsy-proven rejection in pediatric kidney transplant recipients. Given the significant risk for the development of biopsy-proven rejection with complete AP discontinuation and CNI reduction in our study cohort, we suggest anti-proliferative reduction, not discontinuation, and judicious reduction in CNI trough goals with close monitoring as a strategy for treatment of BK viremia with concomitant use of leflunomide therapy.
-
mTor-inhibition within the first days after pediatric heart transplantation is a potentially safe option to prevent cardiac allograft vasculopathyoa
Graphical Abstract
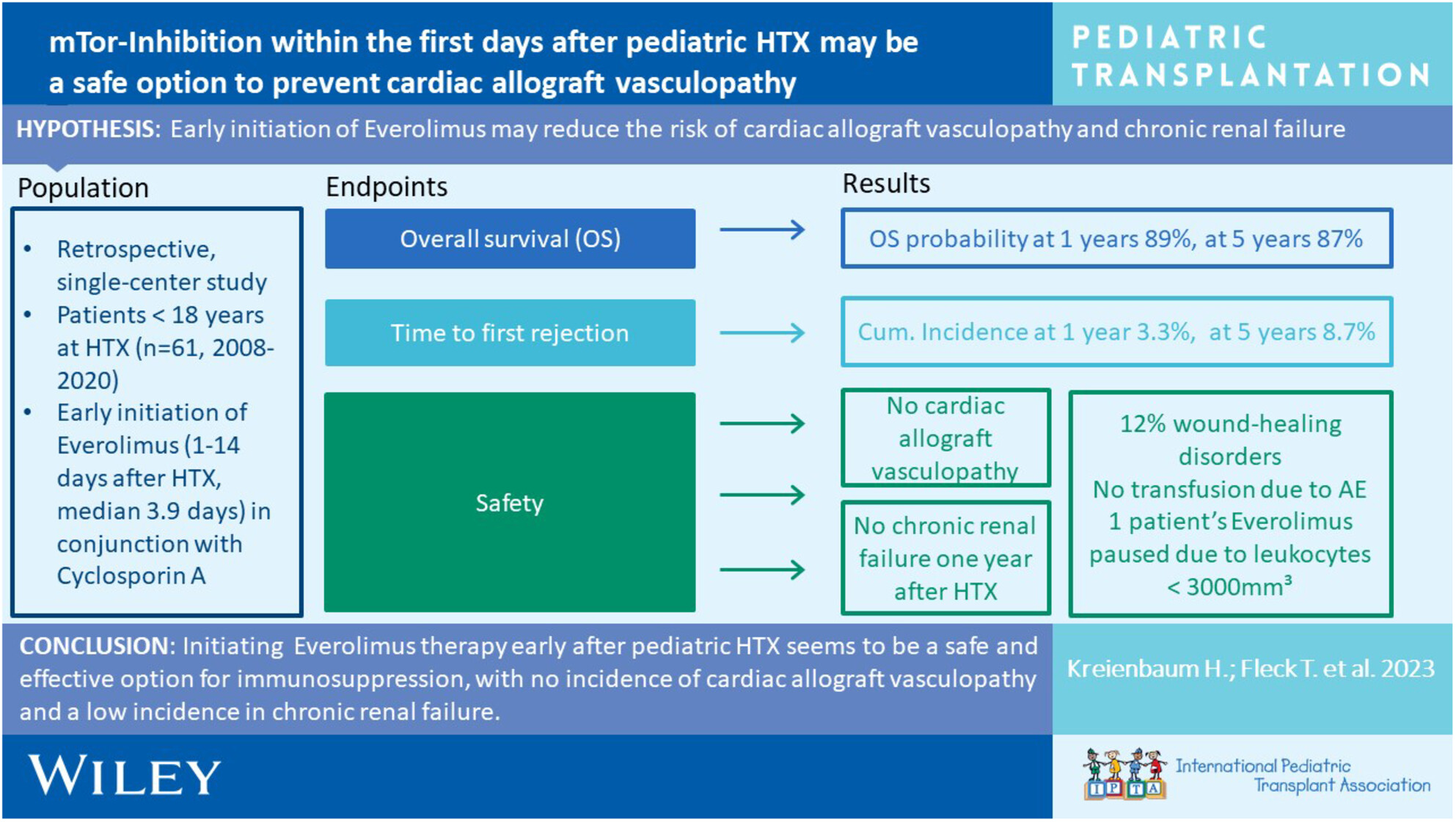
Initiating Everolimus therapy early after pediatric HTX seems to be a safe and effective option for immunosuppression, with no incidence of cardiac allograft vasculopathy and a low incidence in chronic renal failure.