Journal list menu

 Issue
IssueANZ Journal of Surgery: Volume 92, Issue 6
1292-1580June 2022
Export Citations
Download PDFs
ISSUE INFORMATION
EDITORIALS
Promoting good practice before, during and after transfers
- Pages: 1296-1297
- First Published: 10 June 2022
Dialogue and understanding equals effective communication
- Pages: 1298-1299
- First Published: 10 June 2022
PERSPECTIVES
Surgical inter-hospital transfers: life saver or resource drainer?
- Pages: 1300-1301
- First Published: 10 June 2022
Hepato-pancreato-biliary fellowship training in Australia and New Zealand: reflections and perspectives
- Pages: 1302-1303
- First Published: 10 June 2022
Is it time to re-embrace the art of common bile duct exploration?
- Pages: 1304-1305
- First Published: 10 June 2022
COVID-19 vaccine hesitancy in vascular surgery patients: insights from an Aotearoa New Zealand Centre
- Pages: 1306-1307
- First Published: 10 June 2022
Computational biomechanics: a potential new tool for the vascular surgeon in personalized management
- Pages: 1308-1311
- First Published: 10 June 2022
SPECIAL ARTICLES
Factors influencing interhospital transfer delays in emergency general surgery: a systematic review and narrative synthesis
- Pages: 1314-1321
- First Published: 18 April 2022

Gaps in emergency surgical coverage in regional and rural locations are managed with interhospital transfers, despite inferior outcomes. A systematic review of the contemporary literature was performed and identified a paucity of knowledge on factors influencing interhospital transfer delays. More robust prospective cohort studies were recommended.
Predictors of interhospital transfer delays in acute surgical patient deaths in Australia: a retrospective study
- Pages: 1322-1331
- First Published: 03 April 2022
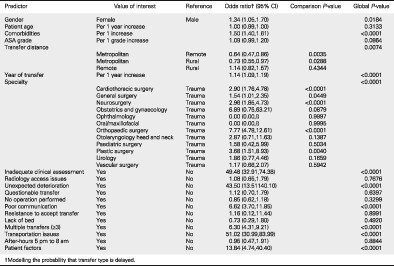
Surgical admissions between 01/01/2010 and 18/08/2020 were extracted from the Australian and New Zealand Audit of Surgical Mortality database and association between transfer type (delayed/prompt) and various predictors were investigated. Modifiable predictors of transfer delay identified were inadequate clinical assessment, poor communication and multiple transfers.
REVIEW ARTICLES
The hepatoprotective effect from ischemia-reperfusion injury of remote ischemic preconditioning in the liver related surgery: a meta-analysis
- Pages: 1332-1337
- First Published: 02 December 2021

The RIPC group had significantly lower postoperative ALT, AST and bilirubin level than the control group. The RIPC was evaluated to have a strong hepatoprotective effect from ischemia-reperfusion injury in the liver related surgery.
Pharmacological prevention of post-operative pancreatitis: systematic review and meta-analysis of randomized controlled trials on animal studies
- Pages: 1338-1346
- First Published: 22 December 2021
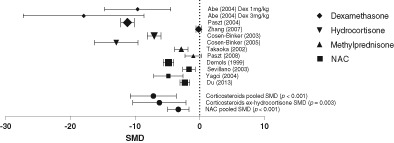
Postoperative pancreatic fistula (POPF) remains a significant complication of pancreatic resection with recent evidence showing a strong association between perioperative pancreatitis and the subsequent development of POPF. We present a systematic literature review and meta-analysis of the prophylactic treatment with corticosteroids or n-acetyl cysteine (NAC) of induced pancreatitis in animal models.
Procedure-specific morbidity of pancreatoduodenectomy: a systematic review of incidence and risk factors
- Pages: 1347-1355
- First Published: 24 January 2022
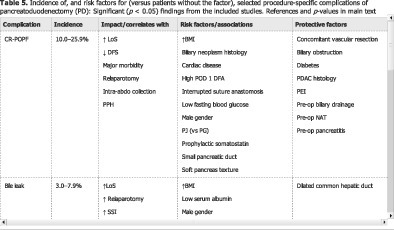
This article consolidates the recent evidence on the incidence of, and risk factors for, preselected procedure-specific complications of pancreatoduodenectomy. An in-depth understanding of these will guide the consenting process and allow surgeons to consider their operative technique.
Defining an optimal surveillance strategy for patients following choledochal cyst resection: results of a systematic review
- Pages: 1356-1364
- First Published: 17 May 2022
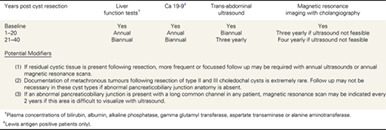
A systematic review was undertaken to define the optimal surveillance protocol for metachronous cancer following choledochal cyst resection. We propose annual liver function tests, Ca 19-9 measurement and two yearly ultrasound assessment for 20 years post cyst resection, with two yearly liver function testing, Ca 19-9 measurement and three yearly ultrasound assessment thereafter.
The human enteric nervous system. Historical and modern advances. Collaboration between science and surgery
- Pages: 1365-1370
- First Published: 11 April 2022
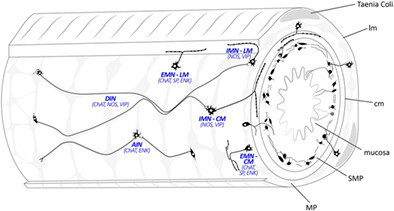
There are considerable advantages and opportunities for surgeons and trainee surgeons in conducting a period of research allied with basic scientists. Such clinicians are well placed to define relevant clinical questions, provide human material and translate the techniques derived in experimental animals to human subjects. This is review illustrates how this has been achieved in the study of the nervous system that controls gut motility.
PERIOPERATIVE CARE
Can you hear me? Analysis of a Queensland patient-initiated escalation process and the importance of communication in surgical care
- Pages: 1371-1376
- First Published: 02 March 2022
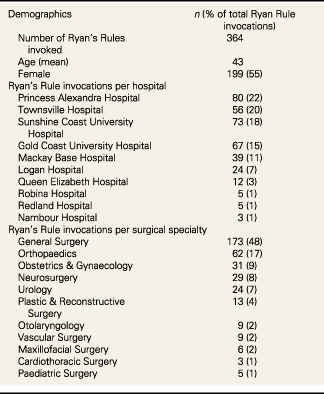
This is a review of a Queensland-based novel patient-initiated escalation process on surgical patients. The study demonstrates that poor communication is the underlying cause of the majority of patient escalations and that the majority of case are resolved with consultation between patient and surgical teams.
Can the alcohol withdrawal scale be applied to post-operative patients?
- Pages: 1377-1381
- First Published: 01 November 2021
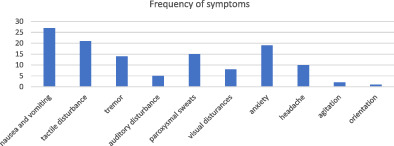
Alcohol withdrawal scales are commonly used in hospitalized inpatients for diagnosing and managing alcohol withdrawal. These scales have only ever been validated in acute detoxification units. Our investigation shows a false positive rate of 18% for the commonly used CIWA-Ar scale based on a prospective study of symptoms in patients at no significant risk of alcohol withdrawal. We call for caution in using alcohol withdrawal scales on surgical wards.
Does implementation of and adherence to enhanced recovery after surgery improve perioperative nutritional management in colorectal cancer surgery?
- Pages: 1382-1387
- First Published: 18 March 2022
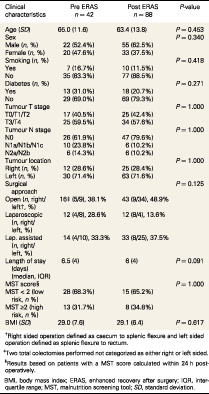
Clinical characteristics of the cohort pre-ERAS and post-ERAS implementation.
Do you have any questions? An analysis of question asking patterns in surgical outpatient consultations
- Pages: 1388-1393
- First Published: 30 March 2022
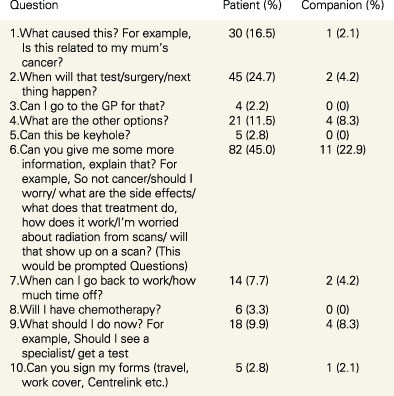
Number and percentages of consultations where the 10 most-commonly asked questions were asked by patient (number of consultations = 182) or companion (number of consultations = 48)
Changing the routine: a move to patient initiated follow up to improve surgical outpatient clinic
- Pages: 1394-1400
- First Published: 16 April 2022
Historically patients have often been followed up routinely for benign anorectal conditions, which places a large strain on outpatient clinic resources. Patient initiated follow up instead puts the onus on the patient to arrange further appointments if they need further input. Protocolising clinic visits allows for guidelines to follow so that every patient gets equal and quality care.
OTOLARYNGOLOGY HEAD AND NECK SURGERY
Paediatric tonsillectomy and adenotonsillectomy in a rural setting: a retrospective study over a period of 6-years
- Pages: 1401-1406
- First Published: 28 March 2022
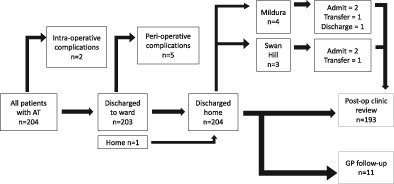
Flowchart of patients and complications in this patient cohort.
Outcomes after definitive treatment for head and neck angiosarcoma
- Pages: 1407-1414
- First Published: 09 May 2022
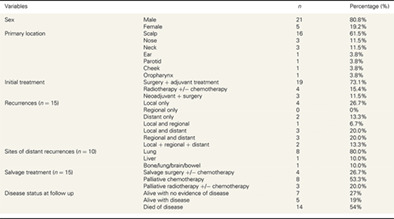
HN-AS is a slowly progressive disease with poor survival. Patients treated with surgery and adjuvant radiotherapy in this series had better outcomes compared with those treated with chemoradiotherapy alone.
Use of telemedicine consultations in head and neck cancer: patient perceptions, acceptability and accessibility
- Pages: 1415-1422
- First Published: 01 May 2022
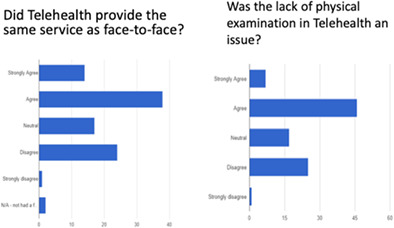
This study demonstrated an overwhelming satisfaction and support for the use of telemedicine appointments in the head and neck surgical oncology setting. This should reassure clinicians that telemedicine is feasible, acceptable and accessible. Telemedicine has benefits in combating COVID-19 as well as increasing accessibility for regional and rural patients, potentially reducing the burden on patients, families and health systems.
ENDOCRINE SURGERY
Selective laryngoscopy before thyroidectomy: a risk assessment
- Pages: 1423-1427
- First Published: 11 April 2022
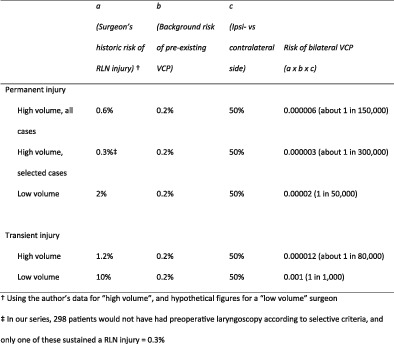
Patients presenting for thyroidectomy may have an unrecognised pre-existing vocal cord palsy (VCP) which raises the danger of bilateral VCP if such a patient sustains an injury to the RLN on the sole functioning side. Part of the rationale for routine preoperative laryngoscopy is to eliminate such a risk. This article endeavours to quantify the potential risk so surgeons can decide if preoperative laryngoscopy is warranted, either routinely or selectively.
Preoperative serum calcitonin may improve initial surgery for medullary thyroid cancer in patients with indeterminate cytology
- Pages: 1428-1433
- First Published: 12 April 2022
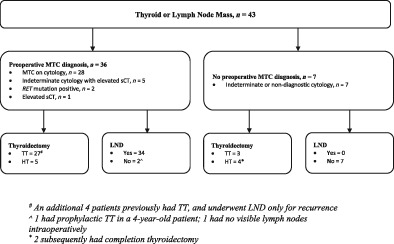
Medullary thyroid cancer is a challenging and rare diagnosis. There are conflicting recommendations as to the use of sCT between different guidelines and so we hoped to identify the utility of serum calcitonin as a biomarker for possible MTC.
BREAST SURGERY
Incidental findings on single-photon emission computed tomography/computed tomography (SPECT/CT) lymphoscintigraphy in breast cancer: the proposed Westmead SPECT/CT incidental findings classification
- Pages: 1434-1439
- First Published: 31 March 2022

Male breast cancer: a Singapore perspective
- Pages: 1440-1446
- First Published: 25 April 2022
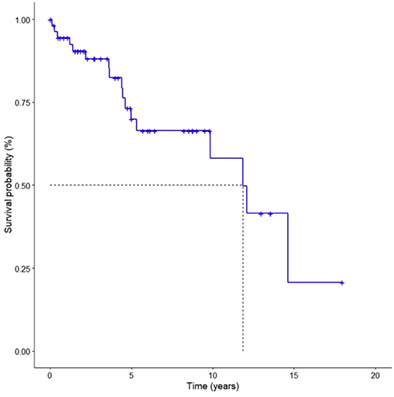
Overall survival of MBC patients.
COLORECTAL SURGERY
Does deep neuromuscular blockade provide improved outcomes in low pressure laparoscopic colorectal surgery? A single blinded randomized pilot study
- Pages: 1447-1453
- First Published: 10 January 2022
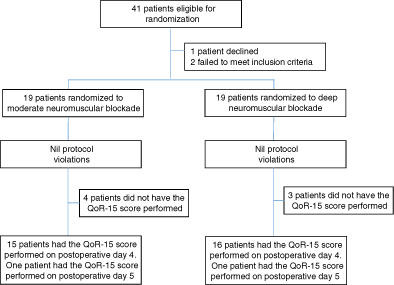
Flow diagram of patients.
Oncological results in rectal cancer patients with a subcentimetre distal margin after laparoscopic-assisted sphincter-preserving surgery
- Pages: 1454-1460
- First Published: 27 January 2022
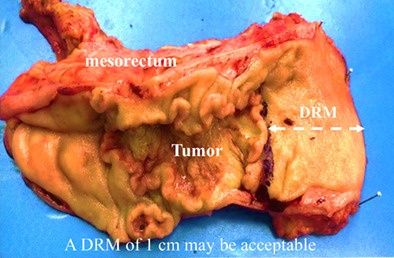
The optimal distal resection margin (DRM) has been debated in sphincter-saving surgery for patients with low-lying rectal cancers. We analysed the impact of a DRM of 1 cm on local recurrence and long-term survival for patients who underwent sphincter-preserving surgery. No matter whether patients received neoadjuvant therapy, a DRM of 1 cm may be acceptable.
The health-related quality of life changes following surgery in patients with colorectal cancer: a longitudinal study
- Pages: 1461-1465
- First Published: 18 March 2022
Patient-reported outcome measures have been used to measure health-related quality of life in surgical oncology. While physical aspects are affected in the short term by colorectal cancer surgery, clinically significant improvement in emotional wellbeing are reported early (2 to 4 weeks post-surgery).
Comparison of two-stage and three-stage surgery for obstructing left-sided colon cancer
- Pages: 1466-1471
- First Published: 31 March 2022
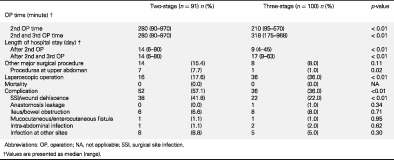
A decompressing stoma can be constructed as bridge to elective surgery in left-sided obstructive colon cancer. Simultaneous tumour resection and stoma reversal carries a higher rate of wound complication compared with tumour resection followed by stoma reversal in separate surgeries. However, issues such as the location of the tumour and diverting stoma, along with the need to resect other upper abdominal organs, should all be considered when deciding the stages of operation.
A comparison of extracorporeal side to side or end to side anastomosis following a laparoscopic right hemicolectomy for colon cancer
- Pages: 1472-1479
- First Published: 11 April 2022
This study aimed to investigate whether an extracorporeal side-to-side (SS) or end-to-side (ES) stapled anastomosis impacts short- and long-term outcomes after an oncological laparoscopic right hemicolectomy. In a 1040 patient cohort, the type of extracorporeal stapled anastomosis had minimal impact on morbidity and survival outcomes; however, a side to side stapled anastomosis is more likely to be a faster operation with a higher postoperative ileus rate.
UROLOGY
Outpatient transperineal prostate biopsy under local anaesthesia is safe, well tolerated and feasible
- Pages: 1480-1485
- First Published: 10 March 2022
Transperineal prostate biopsies can be performed under local anaesthesia safely with excellent patient tolerability. Patient rated pain scores were rated the highest during infiltration of local anaesthetic agent with a median score of 5, dropping to a median pain score of 1 at conclusion of the procedure. Vast majority of patients (85.4%) would opt for a repeat TPB under local anaesthesia should the need for prostate biopsy arise again.
Evaluating the diagnostic role of in-bore magnetic resonance imaging guided prostate biopsy: a single-centre study
- Pages: 1486-1491
- First Published: 28 April 2022
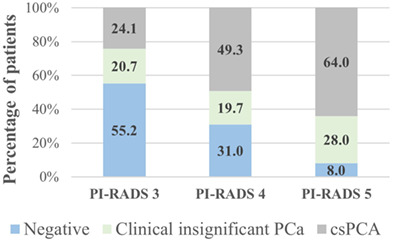
In-bore MRI guided biopsy of the prostate gland provides accurate is safe and feasible method to investigate suspicions of prostate cancer.
The role of intra-operative void score during transurethral resection of prostate as a marker of efficacy: a feasibility study
- Pages: 1492-1497
- First Published: 30 March 2022
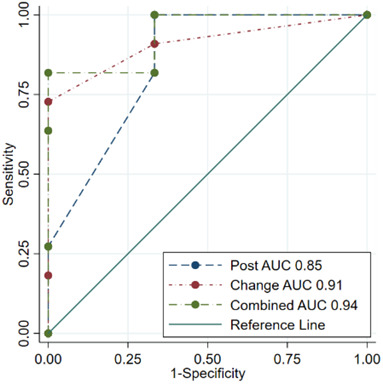
This study assesses the feasibility of a novel intra-operative void scoring technique (Chambers Test). Chambers Test during TURP is simple, reproducible, fast and requires minimal resources. In TURP it may predict successful outcomes by identifying patients who will be catheter free post-operatively as opposed to those who will be catheter dependent despite the procedure.
PROFESSIONAL SKILLS FOR SURGEONS
Applying the ‘three buckets’ theory of situational awareness to surgical training: an updated framework
- Pages: 1498-1501
- First Published: 29 April 2022
HOW TO DO IT
How to do noninflated intracorporeal anastomosis
- Pages: 1502-1503
- First Published: 09 April 2022
We present a modified technique called noninflated intracorporeal ileocolic anastomosis, which maintains the benefits of the intracorporeal technique, but has the advantages of no requirement for laparoscopic suturing.
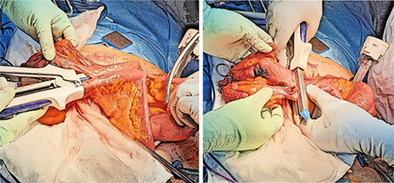
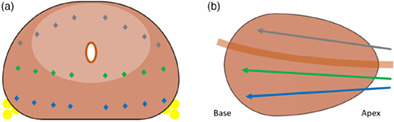
How to do subcostal transversus abdominis plane catheters during midline laparotomy
- Pages: 1504-1505
- First Published: 21 April 2022
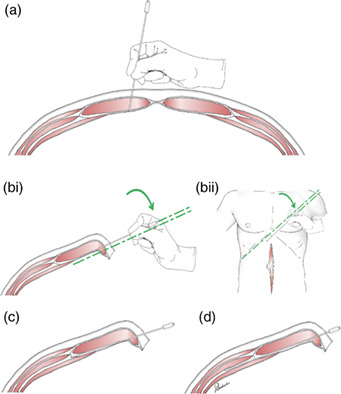
Accessing the transversus abdominis plane during midline laparotomy
IMAGES FOR SURGEONS
Appendiceal torsion: a rare case of acute appendicitis
- Pages: 1508-1509
- First Published: 21 October 2021
Perforated caecal carcinoma within a strangulated inguinal hernia
- Pages: 1512-1513
- First Published: 19 October 2021
Traumatic rupture of a cervical thoracic duct cyst: an unusual presentation of a rare diagnosis
- Pages: 1514-1515
- First Published: 25 October 2021
Idiopathic spontaneous lesser sac haemorrhage possibly due to endometrioma
- Pages: 1516-1518
- First Published: 26 October 2021
Low-grade fibromyxoid sarcoma with high-grade features, a rare finding
- Pages: 1519-1521
- First Published: 28 October 2021
Delayed caecal perforation from amoebic dysentery
- Pages: 1522-1523
- First Published: 19 October 2021
Unusual case of hydatid in the chest, liver and pelvis
- Pages: 1524-1526
- First Published: 21 October 2021
Jejunal diverticulitis miming acute appendicitis and revealing an intestinal non-rotation
- Pages: 1527-1529
- First Published: 21 October 2021
Metastatic gastrointestinal stromal tumour of the descending colon: the importance of complete histological assessment prior to operative management
- Pages: 1530-1532
- First Published: 25 October 2021
Malignant melanoma of the heart: ambiguity and surprise
- Pages: 1533-1535
- First Published: 25 October 2021
Reconstructing a chest wall defect with the aid of three-dimensional printed pleural contour
- Pages: 1536-1538
- First Published: 25 October 2021
Surgical management of colocutaneous fistulae in diverticulitis
- Pages: 1542-1544
- First Published: 25 October 2021
Splenic flexure intussusception: a rare complication post colonoscopy
- Pages: 1545-1546
- First Published: 25 October 2021
‘Radical’ gallbladder avulsion due to blunt trauma
- Pages: 1547-1548
- First Published: 01 November 2021
Advanced application of transanal total mesorectal excision in the frozen pelvis: a novel application in a challenging Hartmann's reversal
- Pages: 1549-1550
- First Published: 28 October 2021
Coexistence of aberrant left hepatic artery and duplicated left gastric artery: a potential surgical pitfall
- Pages: 1551-1552
- First Published: 26 October 2021
Extra-peritoneal oligometastatic renal cell carcinoma: atypical pattern of metastasis and novel localization techniques
- Pages: 1553-1555
- First Published: 01 November 2021
Hepatomesenteric trunk: a rare anatomical variation
- Pages: 1556-1557
- First Published: 01 November 2021
Acute testicular pain after laparoscopic appendicectomy: a rare case of provoked bilateral thrombosed varicoceles
- Pages: 1558-1559
- First Published: 01 November 2021
Stones have been known to move: Bouveret's syndrome treated with cholecystolithotomy after previous episode of gallstone ileus
- Pages: 1560-1562
- First Published: 01 November 2021
‘Slip sign’: radiological feature of internal hernia after laparoscopic colorectal surgery – what surgeons and radiologists should be aware of
- Pages: 1563-1564
- First Published: 08 November 2021
Unusual case of an intraneural ganglion cyst of the tibial nerve
- Pages: 1565-1566
- First Published: 01 November 2021
Abnormalities at the colorectal anastomosis: granulation tissue or cancer recurrence?
- Pages: 1567-1568
- First Published: 09 November 2021
Submucosal lipoma causing recto-sigmoid intussusception associated with an incidental gastrointestinal tumour
- Pages: 1570-1572
- First Published: 03 November 2021
Adhesive small bowel obstruction secondary to endoscopic linear stapler post laparoscopic right hemicolectomy
- Pages: 1573-1574
- First Published: 05 November 2021
A case of tubo-ovarian abscess associated diverticulitis managed without bowel resection
- Pages: 1575-1576
- First Published: 09 November 2021
LETTERS TO THE EDITOR
Re: Neuroendocrine tumour within a Meckel's diverticulum
- Page: 1577
- First Published: 10 June 2022
A minimally invasive approach to the management of Boerhaave's: is it feasible? Letter to editor
- Page: 1578
- First Published: 10 June 2022
A case of acute cervical diverticulitis involving the colonic graft for oesophageal atresia
- Page: 1579
- First Published: 10 June 2022
Percutaneous cholangioscopy for the management of intrahepatic calculi in the setting of altered abdominal anatomy
- Page: 1580
- First Published: 10 June 2022
Sign up for email alerts
Journal Information
ANZ Journal of Surgery is published on behalf of the Royal Australasian College of Surgeons.
![]()
ANZ J Surgery Resources