


All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Absolute CD3+ T-Cell Counts After Anti-Thymocyte Globulin: Impact on Graft and Infectious Outcomes in Pediatric Kidney Recipientsno
Graphical Abstract
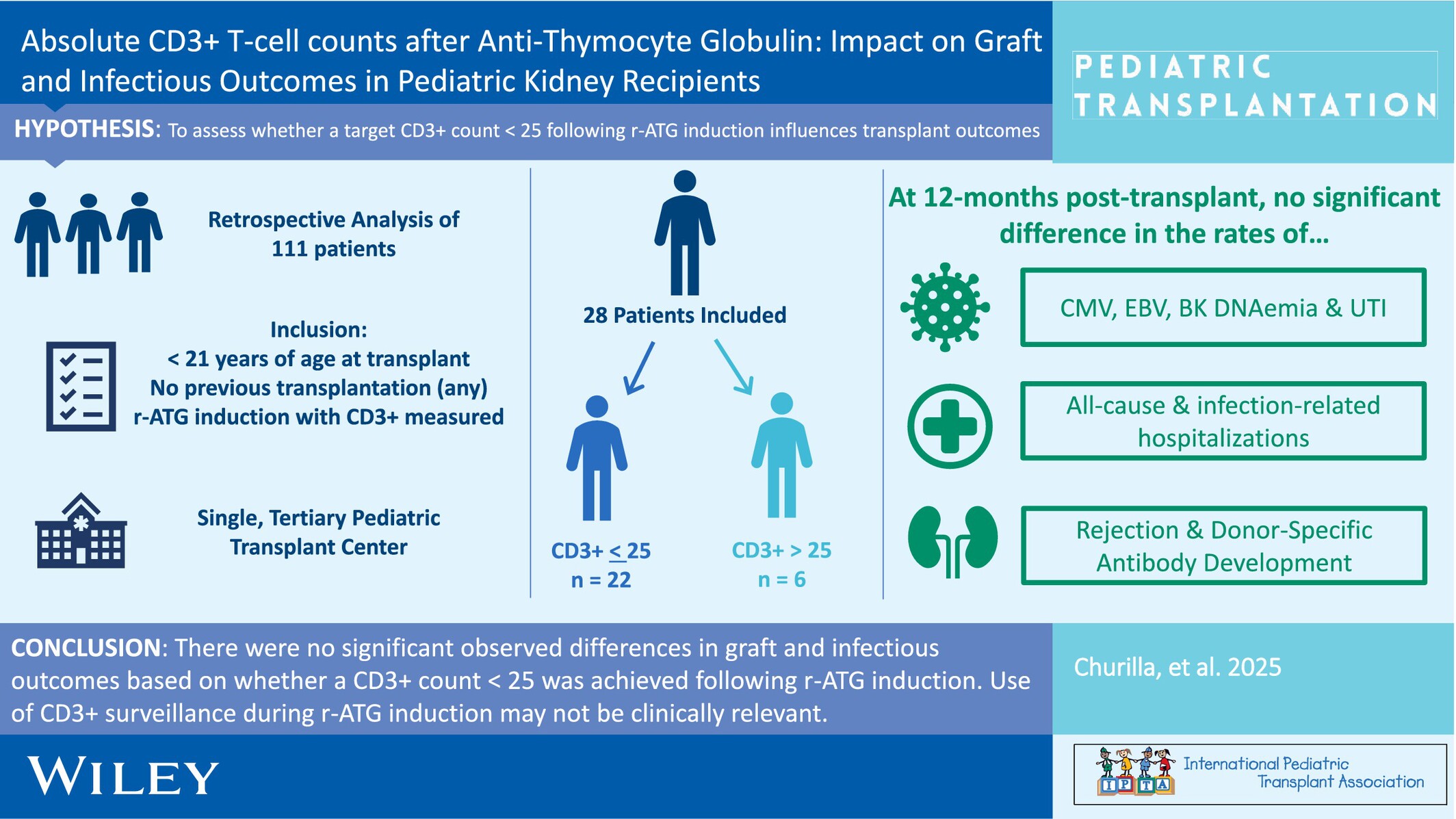
When pediatric kidney transplant recipients were compared based on the achievement (or not) of a CD3+ T-cell count < 25 cells/mm3 following rabbit anti-thymocyte globulin induction, there were no differences in infectious or graft outcomes by 12-months post-transplant.
-
Low Incidence of Rejection and De Novo Donor-Specific Antibody Formation Following COVID-19 Vaccination or Infection Among Pediatric Kidney Transplant Recipientsno
Graphical Abstract
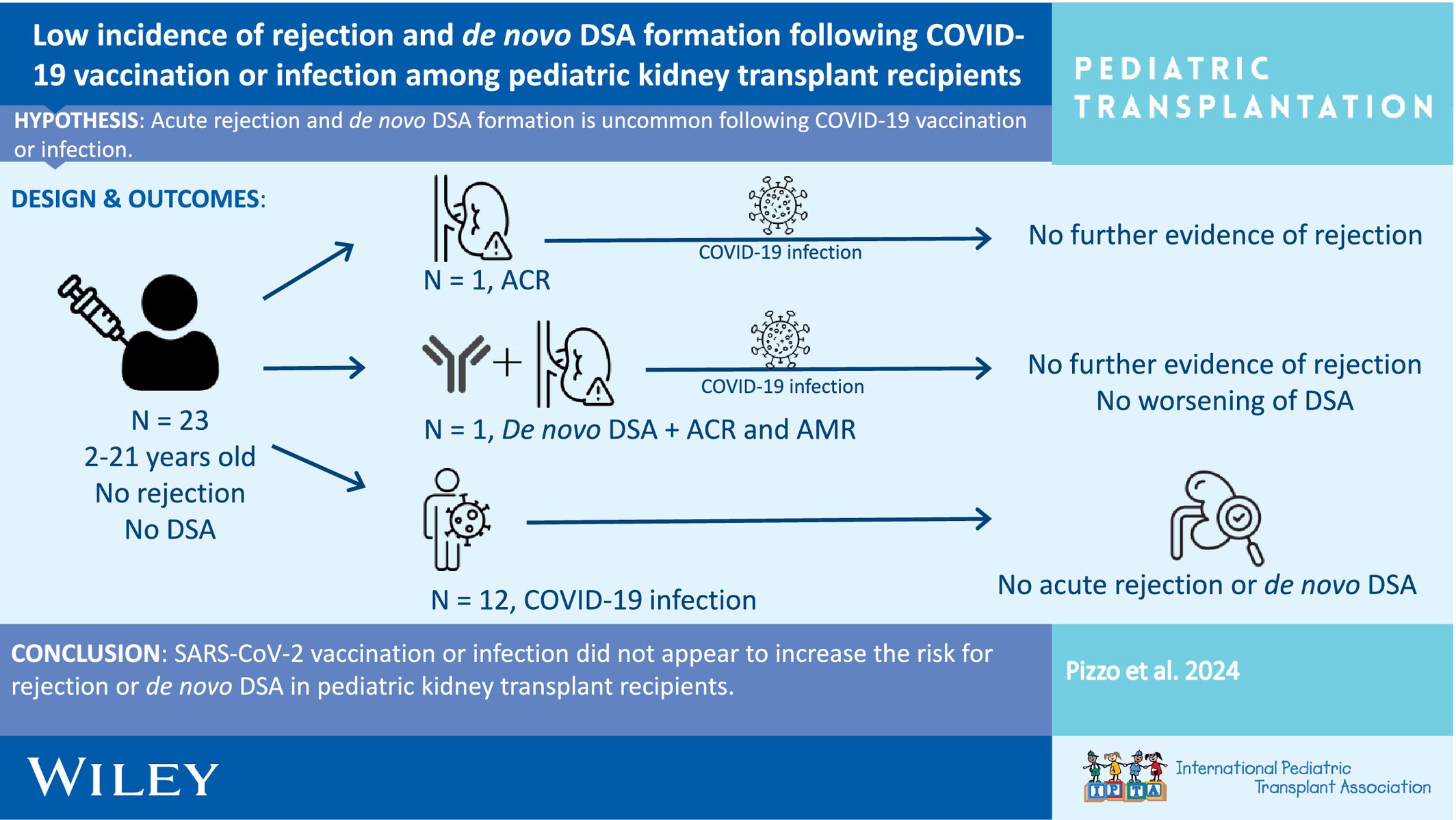
This study investigated the incidence of allograft rejection and de novo donor-specific antibody formation following COVID-19 vaccination or infection among pediatric kidney transplant recipients.
-
Meeting the Challenges of Post-Transplant Lymphoproliferative Disorders After Liver Transplantation in Children: A Proposed Diagnostic and Management Algorithmno
Graphical Abstract
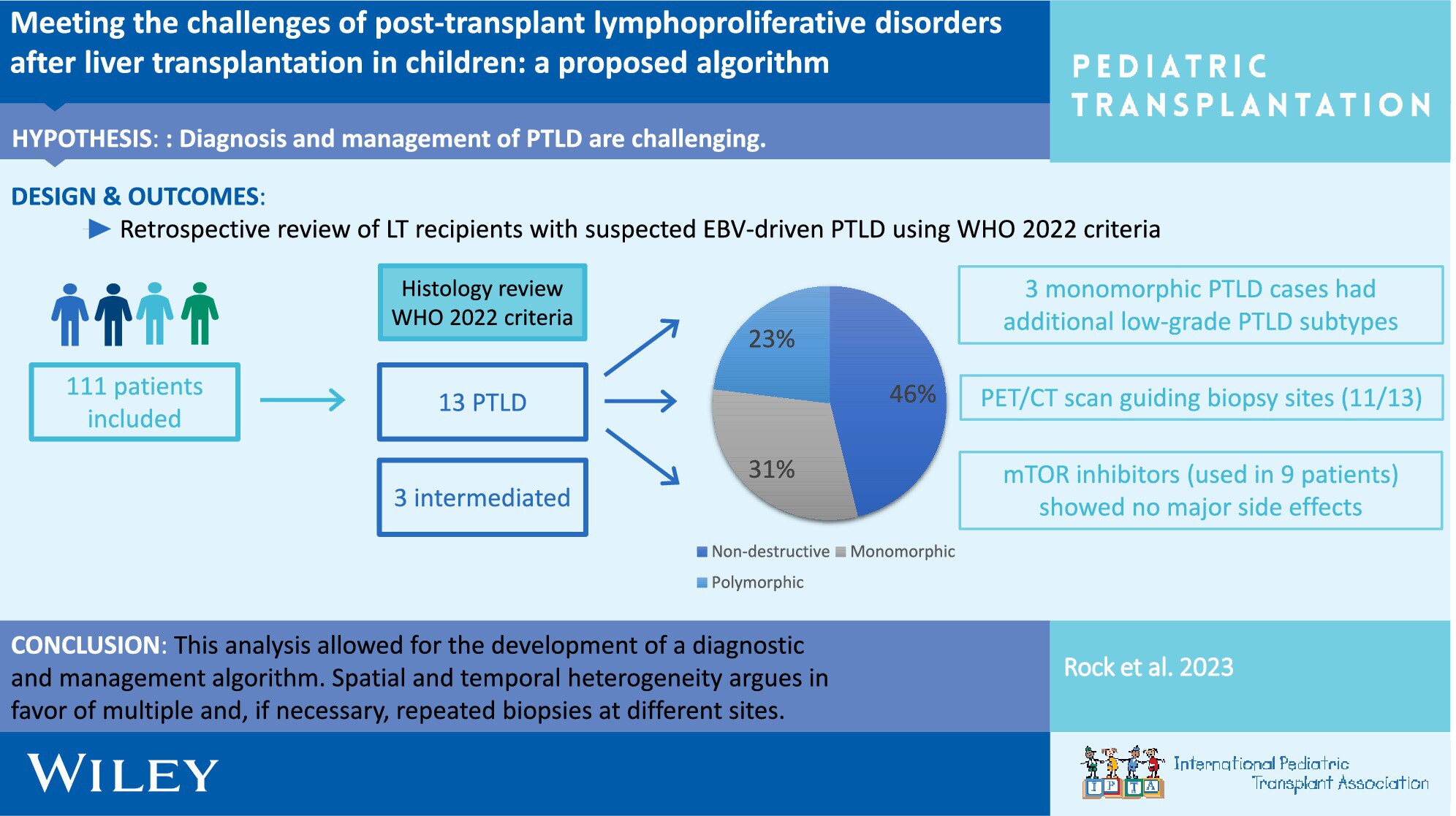
After review of suspected EBV-driven Post-Transplant Lymphoproliferative Disorders (PTLD), according to the WHO 2022 criteria, the incidence was 11.7% in our cohort. Non-destructive PTLD was the most common subtype. Spatial/temporal heterogeneity required multiple biopsies. mTOR inhibitors were well tolerated. A diagnostic algorithm was developed to enhance the management of PTLD.
-
Evaluating Activated Regulatory T Cells as a Biomarker of Chronic Allograft Inflammation in Pediatric Kidney Transplant Recipientsoa
Graphical Abstract
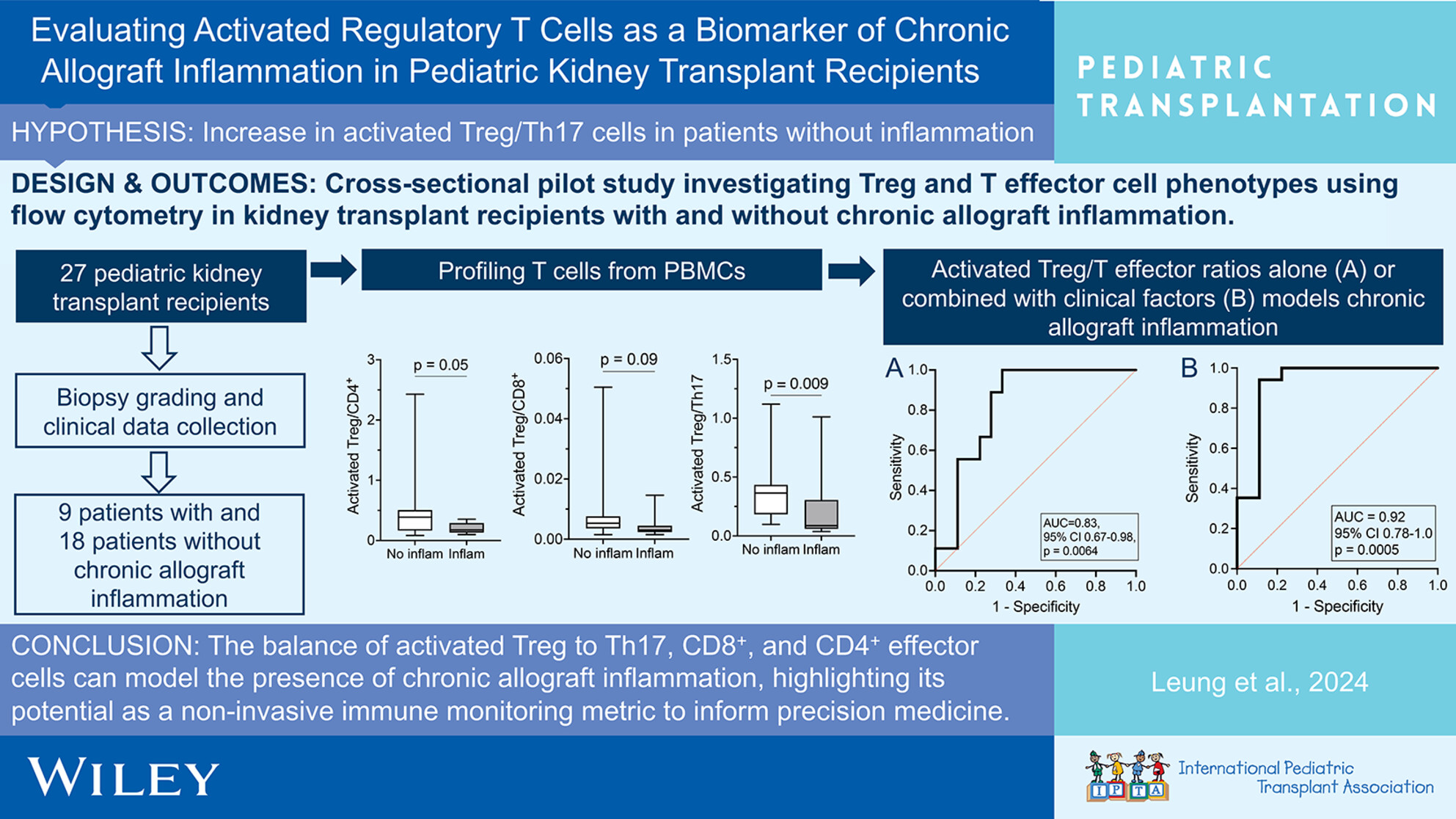
The balance between activated Treg/T effector cells demonstrates potential as a minimally invasive immune monitoring metric that can be used to help identify chronic allograft inflammation in pediatric kidney transplant recipients. Identifying patients with chronic allograft inflammation can help inform earlier intervention and precision medicine.
-
Post-Liver Transplantation–Burkitt Lymphoma in Children: A Single-Center Study of Clinical Characteristics, Treatment, and Outcomesno
Graphical Abstract
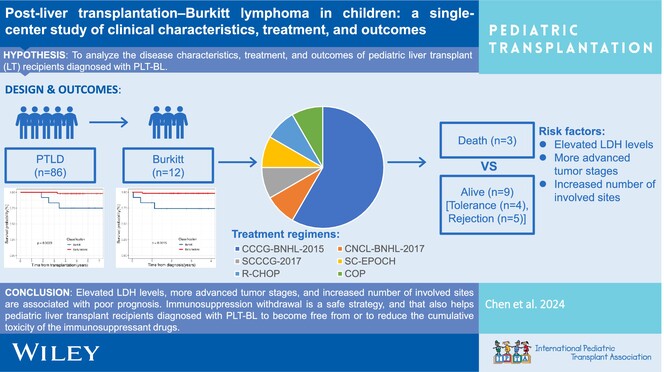
Elevated LDH levels, advanced tumor stages, and increased number of involved sites are associated with poor prognosis in post-liver transplantation–Burkitt lymphoma (PLT-BL). Immunosuppression withdrawal is a safe strategy, and that also helps pediatric LT recipients diagnosed with PLT-BL to become free from or to reduce the cumulative toxicity of the immunosuppressant drugs.
-
Incidence and Management of Posttransplantation Lymphoproliferative Disorder After Pediatric Solid Organ Transplantation: The Norwegian Experienceno
Graphical Abstract
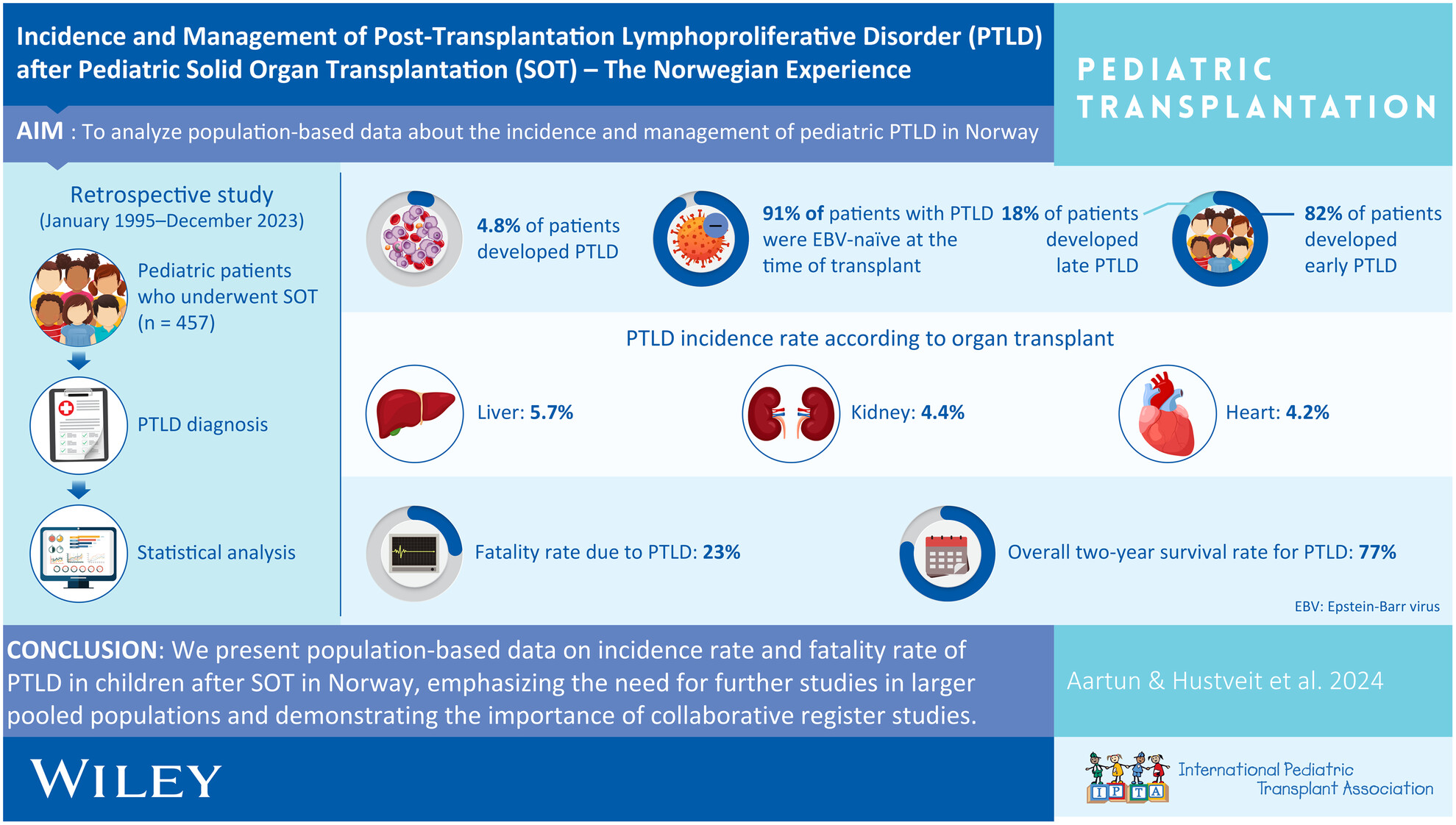
This retrospective quality assurance study aimed to investigate the incidence and management of pediatric PTLD among all 457 pediatric solid organ transplant recipients In Norway since 1995. We found a PTLD incidence rate of 4.8% (kidney 4.4%, liver 5.7%, and heart 4.2%) and a fatality rate of 23%.
-
The Impact of Reduced Immunosuppression on Alloimmunity: A Retrospective Study of Pediatric Kidney Transplant Recipientsoa
Graphical Abstract
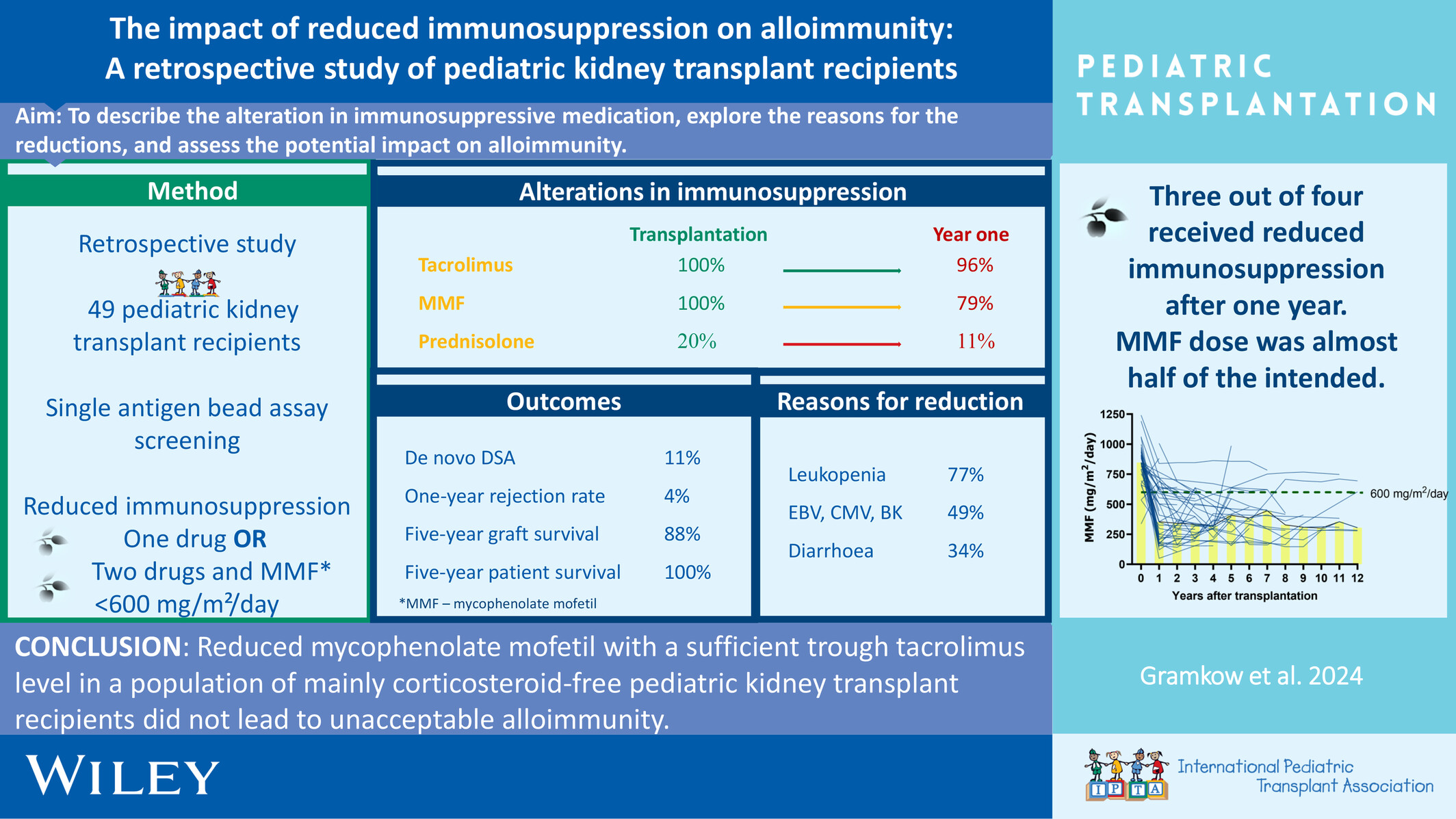
Reduced mycophenolate mofetil with a sufficient trough tacrolimus level in a population of mainly corticosteroid-free pediatric kidney transplant recipients did not lead to unacceptable alloimmunity.
-
Norovirus Management and Outcomes in a Multicenter Pediatric Kidney Transplant Populationoa
Graphical Abstract
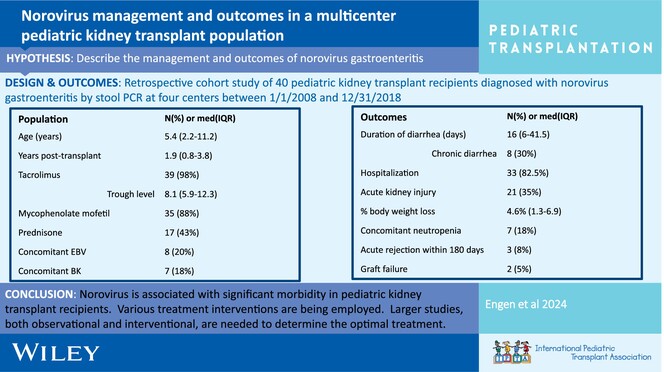
Post-transplant norovirus diarrhea persists for a median of 16 days (IQR 6–41.5 days) with 30% of patients developing chronic diarrhea. Morbidity is high, including AKI in 53% of patients, reduction in immunosuppression 20%, and acute rejection in 8% within 6 months of diagnosis.
-
BK polyomavirus DNAemia, allograft rejection, and de novo donor-specific antibodies after lowering target tacrolimus levels in pediatric kidney transplant recipientsno
Graphical Abstract
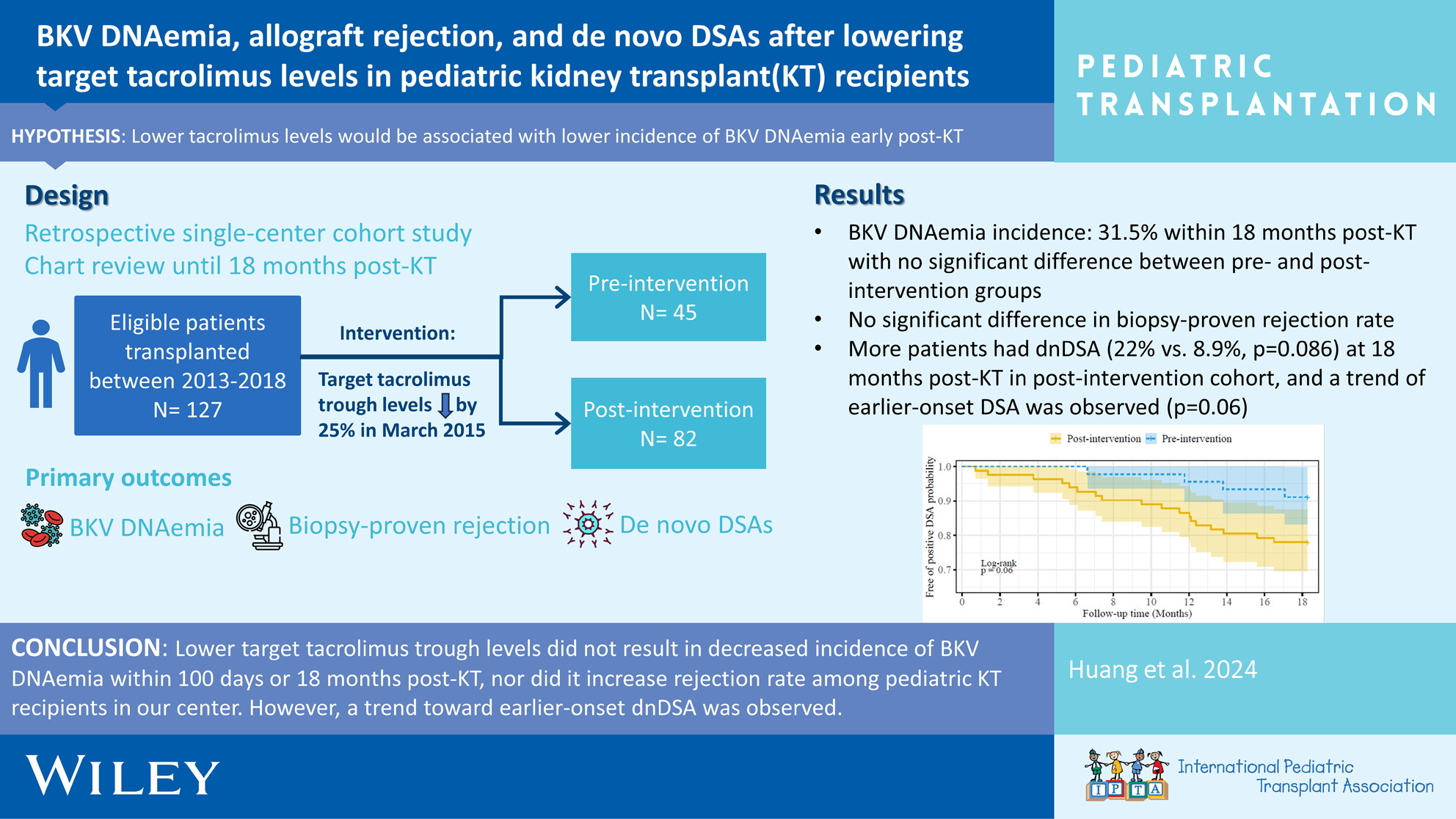
Early BKV DNAemia is common post-pediatric kidney transplant, especially in younger ages, with ~30% incidence within 18 months post-transplant. Favorable outcomes are achieved with (1) frequent monitoring of viremia and (2) timely reduction of immunosuppressive medications, which must be balanced against risk of rejection and development of HLA antibodies.
-
Safety and infectious outcomes in pediatric kidney transplant recipients after COVID-19 vaccination: A pediatric nephrology research consortium studyno
Graphical Abstract
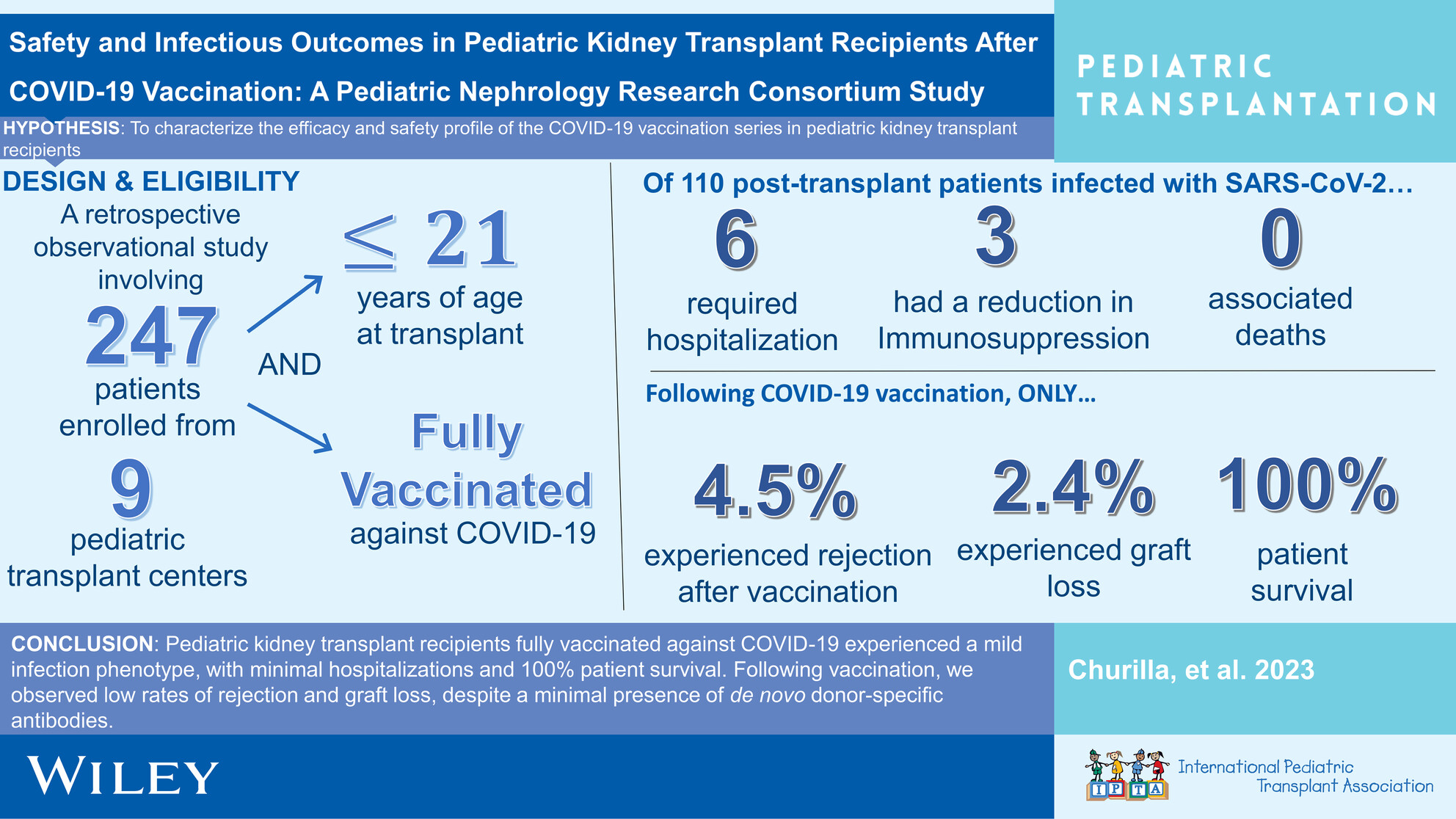
This observational, retrospective investigation demonstrates temporal associations pointing to a reassuring vaccine safety profile and mild SARS-Cov-2 infectious phenotype in pediatric renal transplant recipients fully vaccinated against COVID-19.
-
Long-term outcomes of two-dose alemtuzumab induction in pediatric kidney transplantationoa
Graphical Abstract
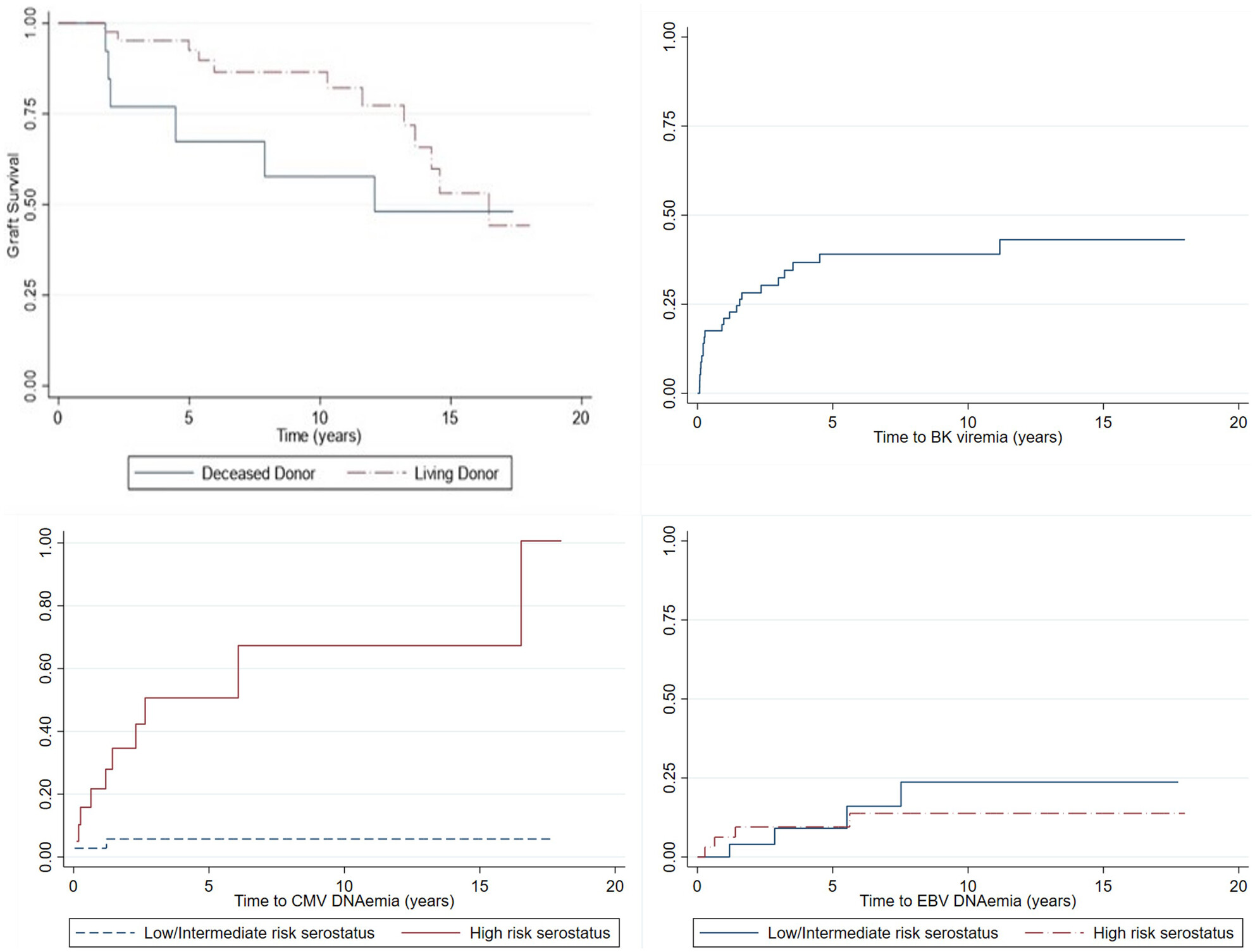
Pediatric kidney transplant recipients given two doses of alemtuzumab induction immunosuppression, with steroid-free maintenance immunosuppression, had a ten-year living-donor graft survival of 86.5% and a deceased donor graft survival of 57.7%. The incidence of viral infections was similar to that reported in other cohorts, and growth improved after transplant.
-
Antibody-mediated rejection in pediatric kidney transplant recipients: A report from the Pediatric Nephrology Research Consortiumno
Graphical Abstract
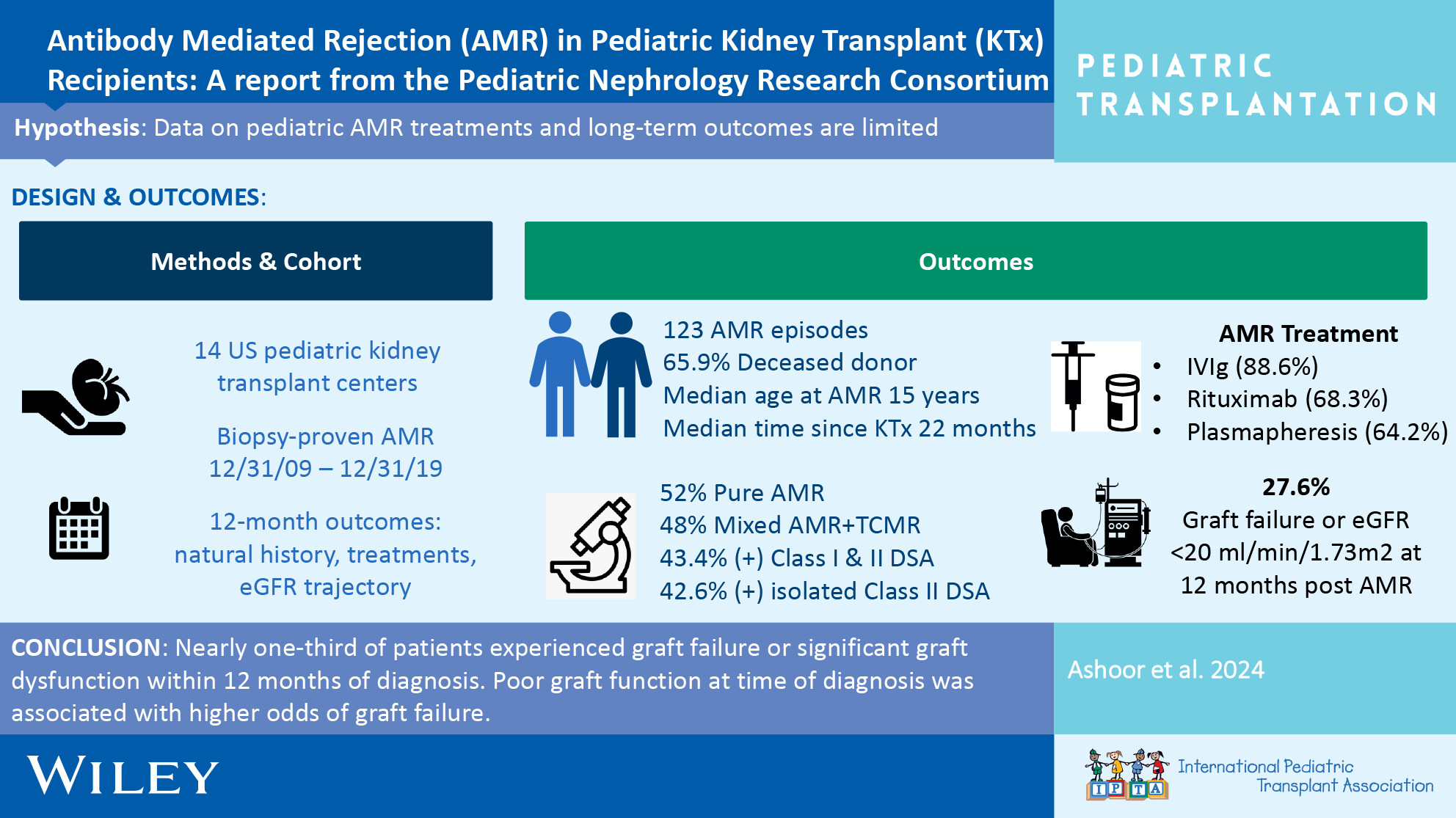
In this large cohort of pediatric kidney transplant recipients with antibody mediated rejection, nearly one-third of patients experienced graft failure or significant graft dysfunction within 12 months of diagnosis. Poor graft function at time of diagnosis was associated with higher odds of graft failure.
-
Effect of pre-emptive rituximab on EBV DNA levels and prevention of post-transplant lymphoproliferative disorder in pediatric kidney transplant recipients: A case series from the pediatric nephrology research consortiumno
Graphical Abstract
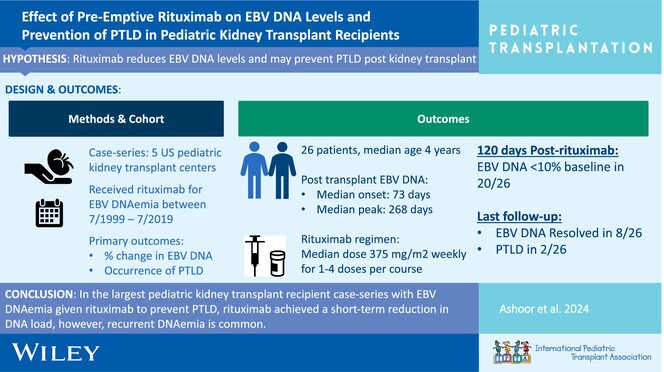
In the largest pediatric kidney transplant recipient case series with EBV DNAemia given rituximab to prevent PTLD, rituximab achieved a short-term reduction in DNA load; however, recurrent DNAemia is common.
-
Leflunomide as adjunct therapy for BK viremia management in pediatric kidney transplant recipientsno
Graphical Abstract
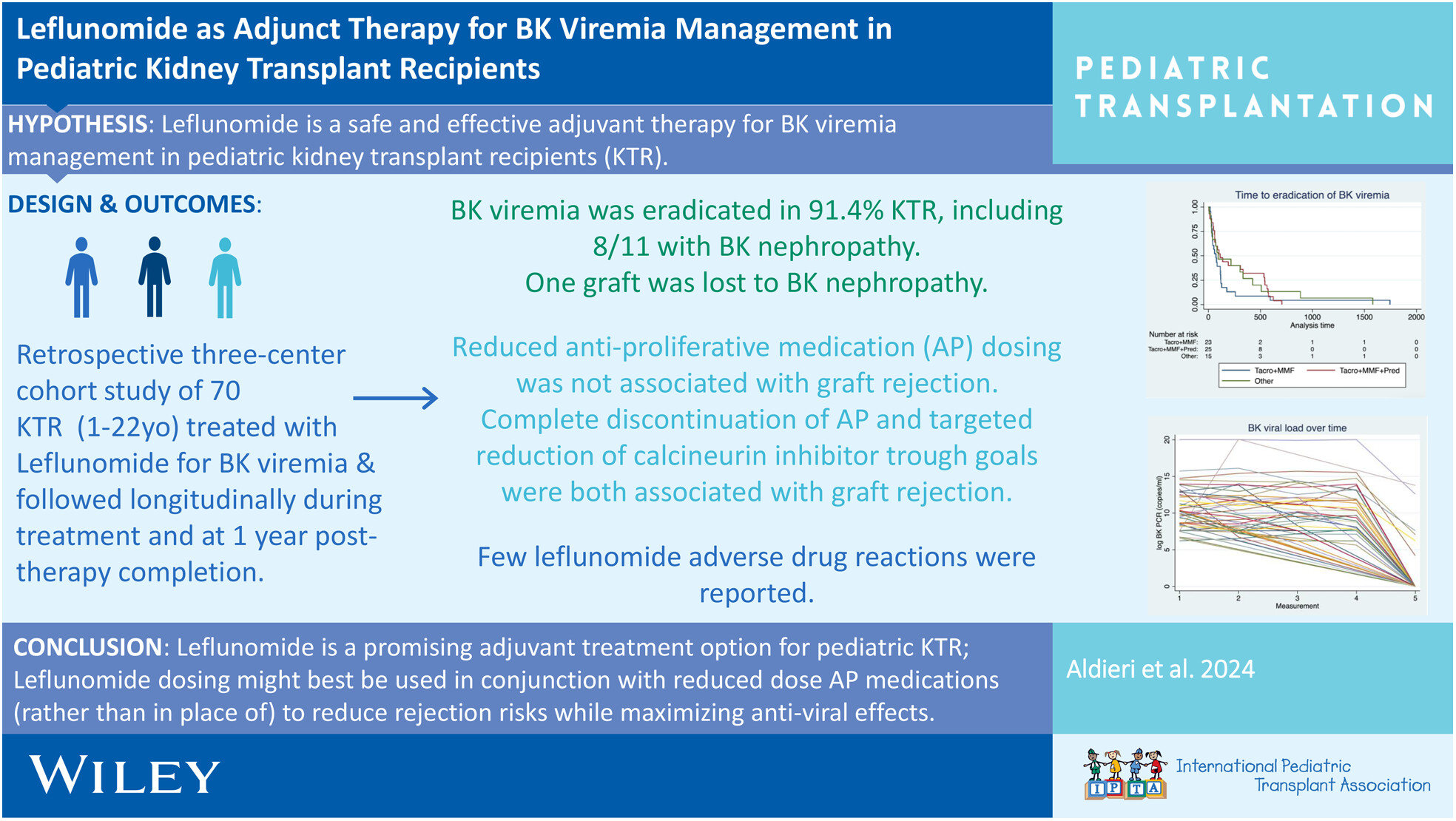
Leflunomide is a promising adjunctive treatment for BK virus eradication and prevention of BK nephropathy, along with IS reduction, particularly anti-proliferative immunosuppression reduction, without significant risk for the development of biopsy-proven rejection in pediatric kidney transplant recipients. Given the significant risk for the development of biopsy-proven rejection with complete AP discontinuation and CNI reduction in our study cohort, we suggest anti-proliferative reduction, not discontinuation, and judicious reduction in CNI trough goals with close monitoring as a strategy for treatment of BK viremia with concomitant use of leflunomide therapy.