


All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Pediatric Organ Donation: 16-Year Experience of PICU/ICU of a Third Level Hospital in Portugal, 2006–2021no
Graphical Abstract
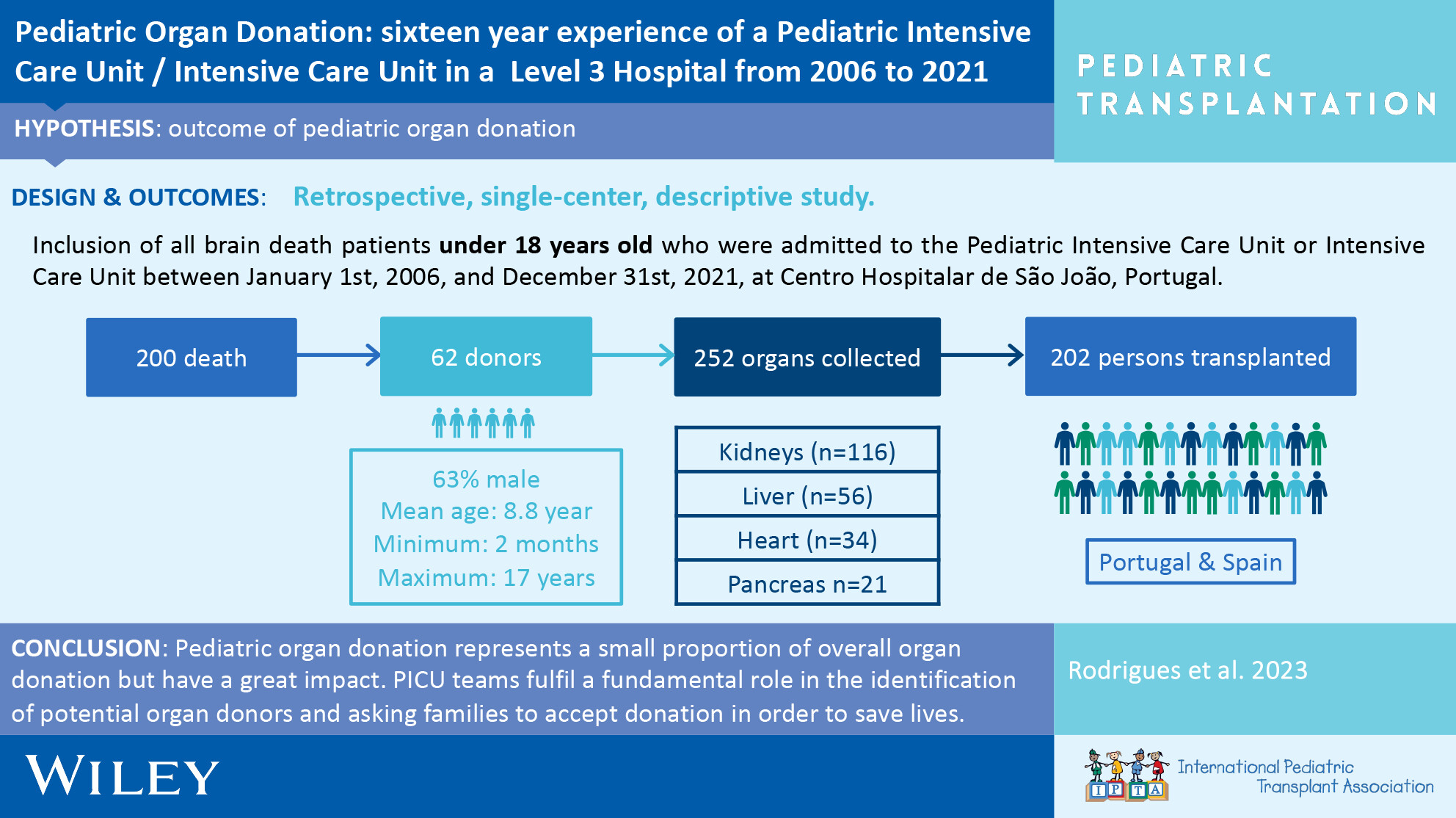
Although pediatric organ donation represents a small proportion of overall organ donation, children and adolescents make a significant contribution to the pool of donated organs. In this study 252 solid organs were collected from children and adolescent. Two hundred and two recipients benefited from 62 pediatric organ donors, with a recipient/donor ratio of 3.3.
-
Cardiovascular Risk in Pediatric Renal Transplant Recipientsno
Graphical Abstract

The low incidence of cardiovascular changes in the population studied confirms the benefit of transplantation for the cardiovascular health of children. Only 4% of sample had an LV mass Z-score ≥ 2.0. After multivariate analysis, only gender, serum triglyceride, and serum renalase concentration remained significantly associated with LV mass.
-
The Consequences of HLA Screening in the Prevention of Graft-Versus-Host Disease in Living Donor Liver Transplantationno
Graphical Abstract
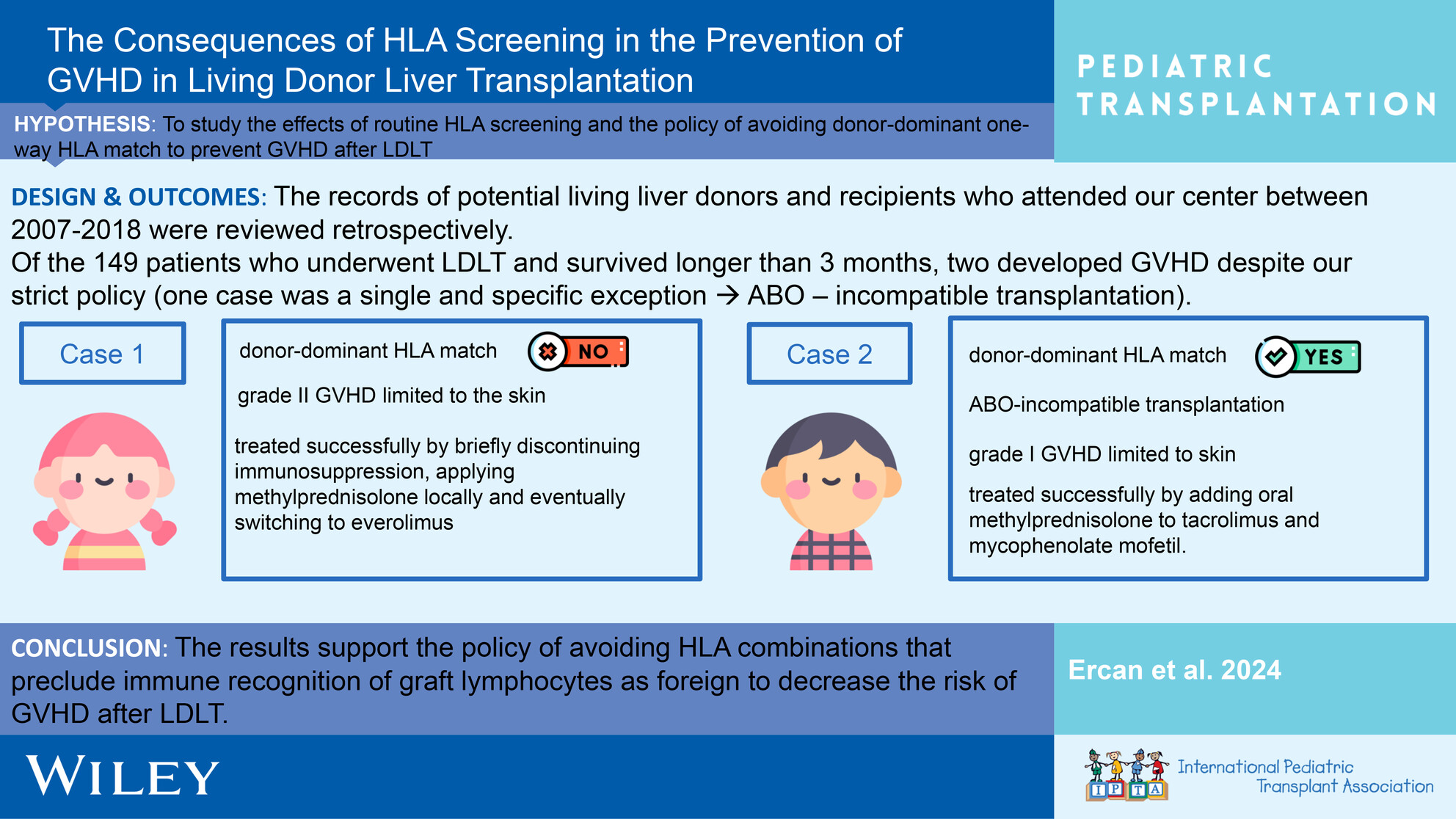
The results support the policy of avoiding HLA combinations that preclude immune recognition of graft lymphocytes as foreign to decrease the risk of GVHD after living donor liver transplantation.
-
Current Status and Outcomes of Living Donor Liver Transplantation for Pediatric Acute Liver Failure: Results From a Multicenter Retrospective Study Over Two Decadesno
Graphical Abstract
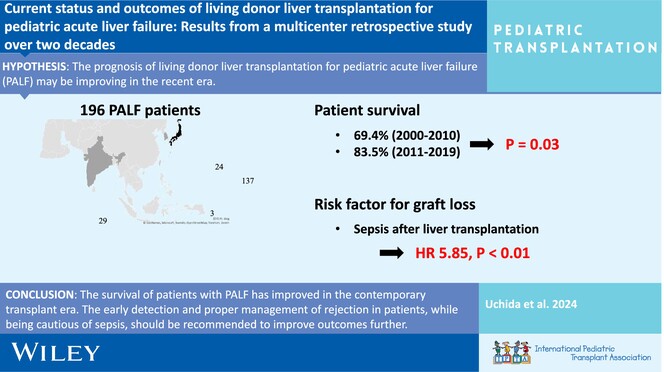
This study describes the prognosis for pediatric patients with acute liver failure by transplant era and shows improved outcomes in recent era due to the advancement in perioperative management and surgical techniques.
-
Comparison of Long-Term Outcomes Achieved With Live Donor and Split Deceased Donor Liver Grafts in Pediatric Liver Transplantationoa
Graphical Abstract
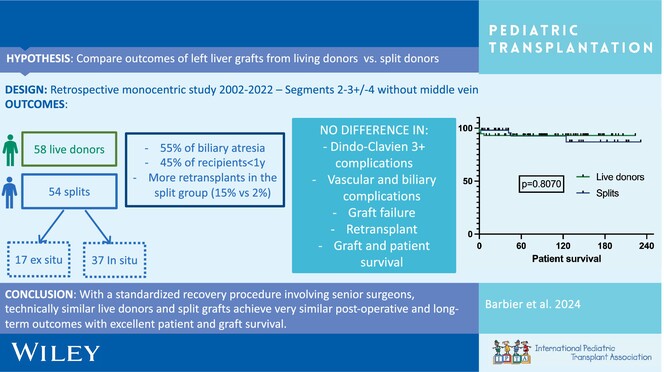
Left lobe split deceased grafts can achieve the same outcomes as live donor grafts and should be considered in an intention-to-split policy to decrease time on the waiting list for young children when a live donor is not available.
-
Long-Term Amino Acid Homeostasis, Neurodevelopmental and Growth Profiles Following Liver Transplantation in Maple Syrup Urine Diseaseno
Graphical Abstract
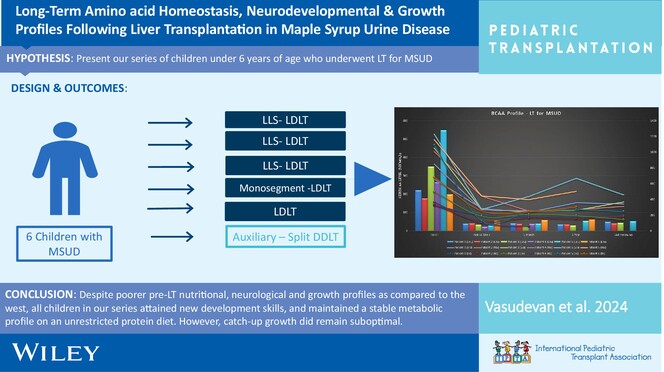
We present our series of LT for MSUD, highlighting their neurodevelopmental profiles and growth aspects within the socio-economic-cultural constraints prevalent in the Indian subcontinent. Despite poorer pre-LT profiles, all children attained new development skills and maintained a stable metabolic profile on an unrestricted protein diet. However, catch-up growth remained suboptimal.
-
Long-Term Outcomes of Living Donor Liver Transplantation for Methylmalonic Acidemiano
Graphical Abstract
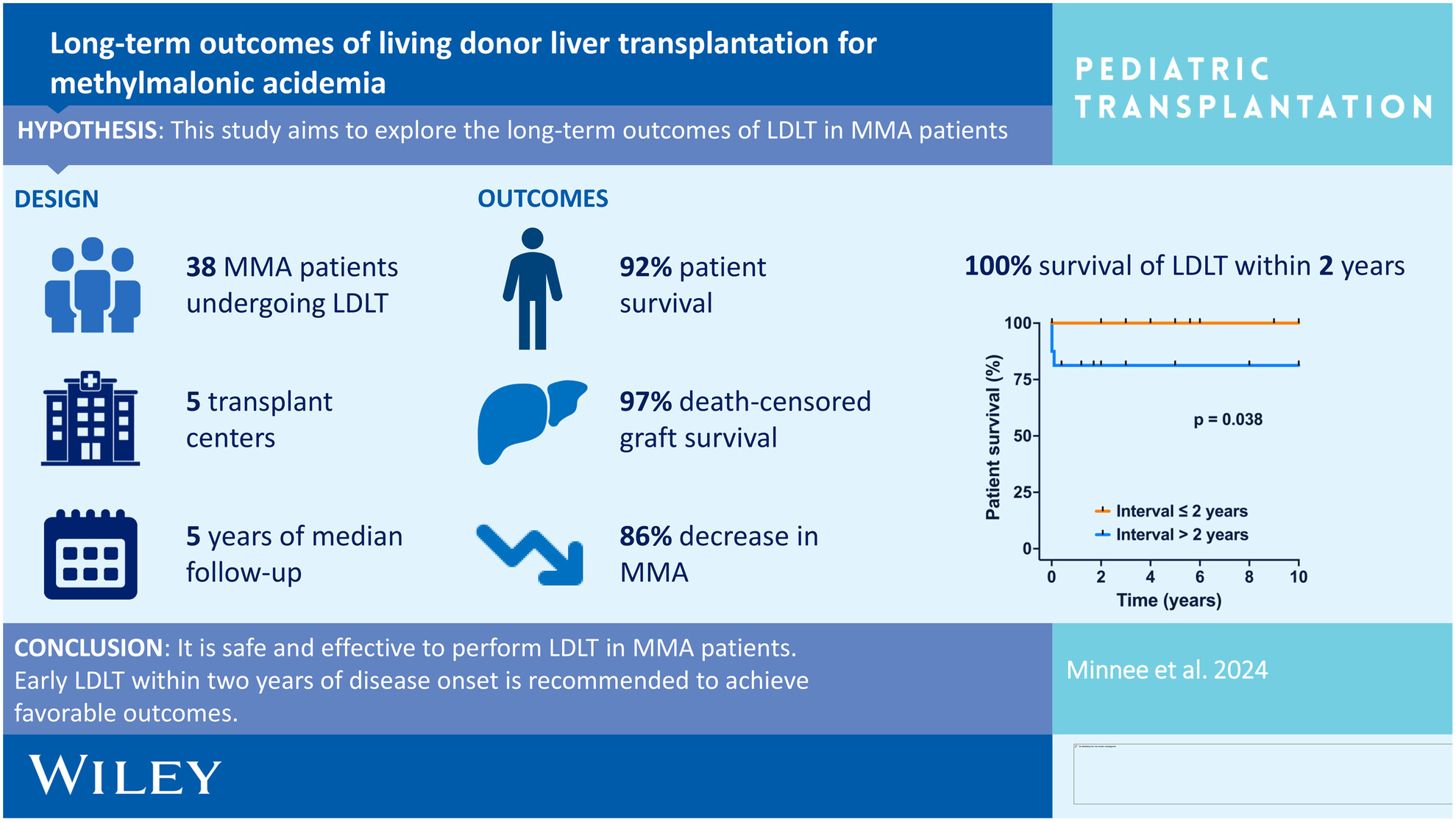
It is safe and effective to perform LDLT in MMA patients. Early LDLT within 2 years of disease onset is recommended to achieve favorable outcomes.
-
Elastography—The New Standard in the Assessment of Fibrosis After Pediatric Liver Transplantation?oa
Graphical Abstract
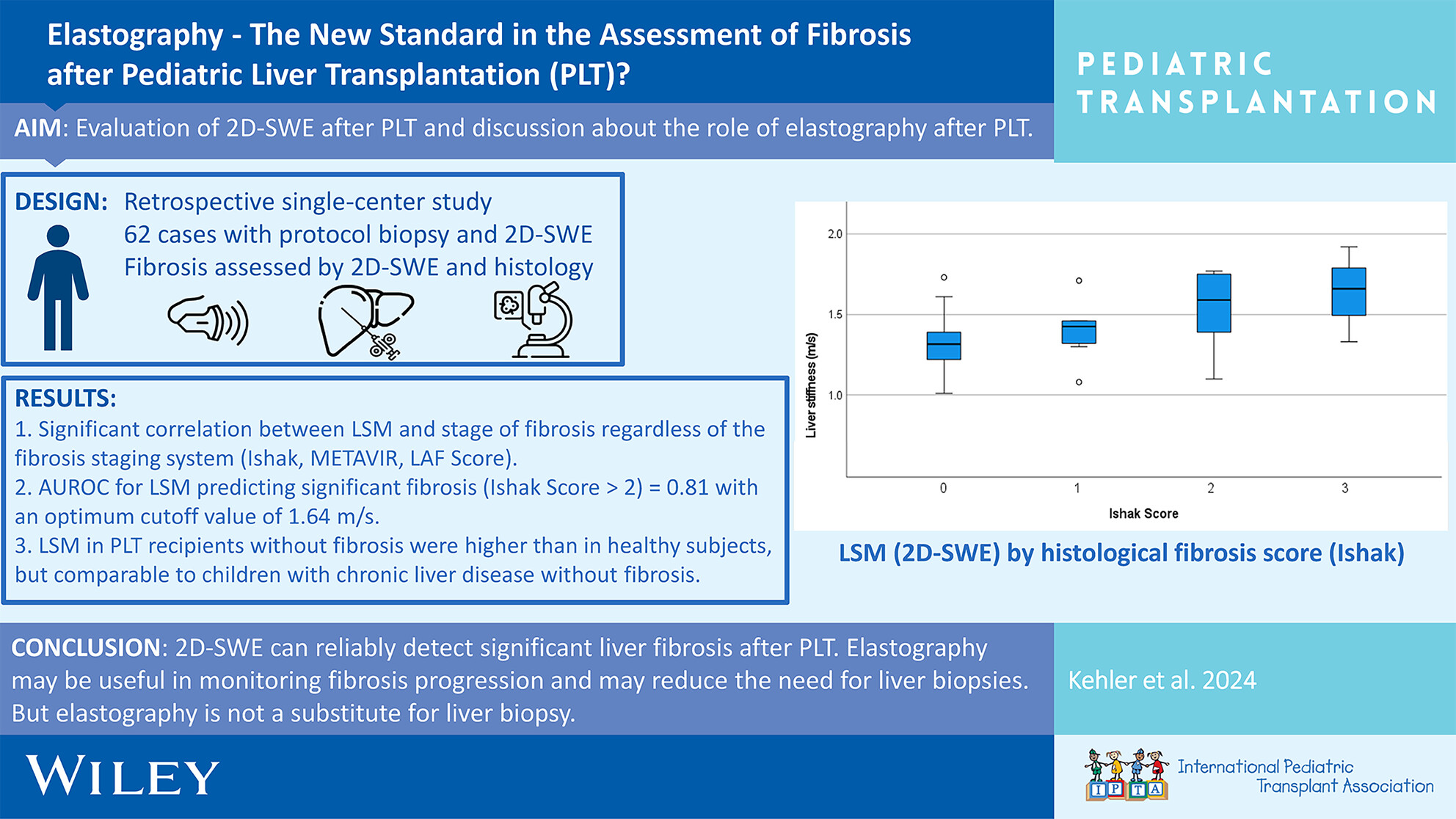
2D-SWE reliably detects significant liver graft fibrosis in pediatric liver transplant recipients, including split-liver cases. This non-invasive method shows promise for improving long-term outcomes and reducing the need for surveillance biopsies, though it does not replace the necessity of liver biopsies.
-
Surgical Site Infections After Pediatric Liver Transplantation—Impact of a Change in Perioperative Prophylactic Antibiotic Protocoloa
Graphical Abstract
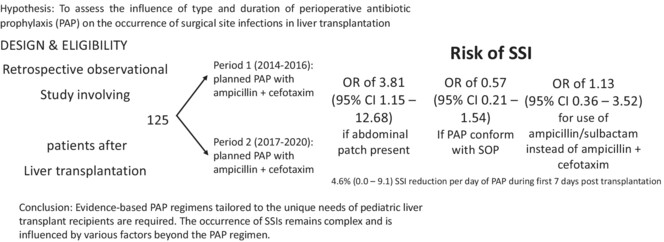
This retrospective observational study in patients following liver transplantation showed an increased risk of SSI if abdominal patch is present. Choice of perioperative prophylaxis was not associated with risk reduction but duration of perioperative antibiotic prophylaxis slightly lowered the risk of SSI within the first 7 days.
-
What Italian PICU Healthcare Providers Think About Donation After Cardiocirculatory Determination of Death: A National Surveyno
Graphical Abstract
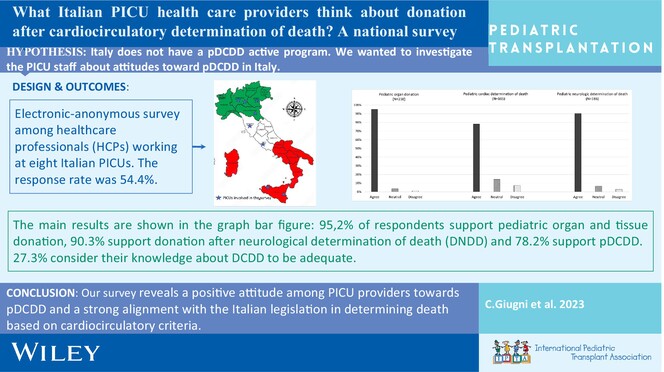
Italy lacks an active pDCDD program. To gauge acceptance and anticipate reactions, we surveyed PICU staff attitudes before its launch. Despite limited knowledge, respondents expressed positive attitudes toward pDCDD, supporting Italian legislation on cardiocirculatory death determination and the “dead donor role.”
-
Constructing an Intent-to-Treat Score Index to Predict Survival Outcomes in Pediatric Liver Transplant Recipientsno
Graphical Abstract
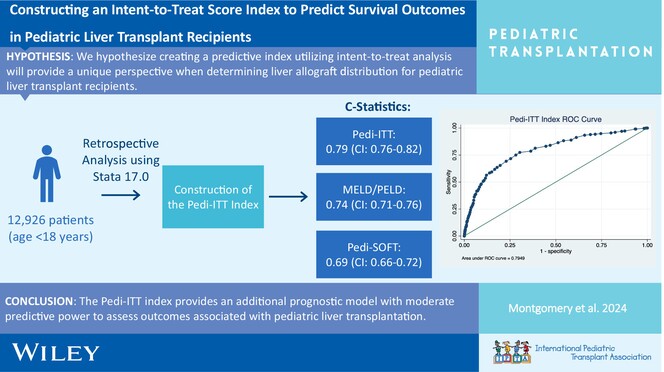
The Pedi-ITT index includes 12 factors found to be significant in predicting intent-to-treat survival for pediatric liver transplant recipients. Our index has a moderate predictive value with a c-statistic of 0.79 as compared to the MELD/PELD and Pedi-SOFT score indices, which had c-statistics of 0.74 and 0.69, respectively.
-
Treatment Strategies for Bile Leak Following Pediatric Liver Transplantationno
Graphical Abstract
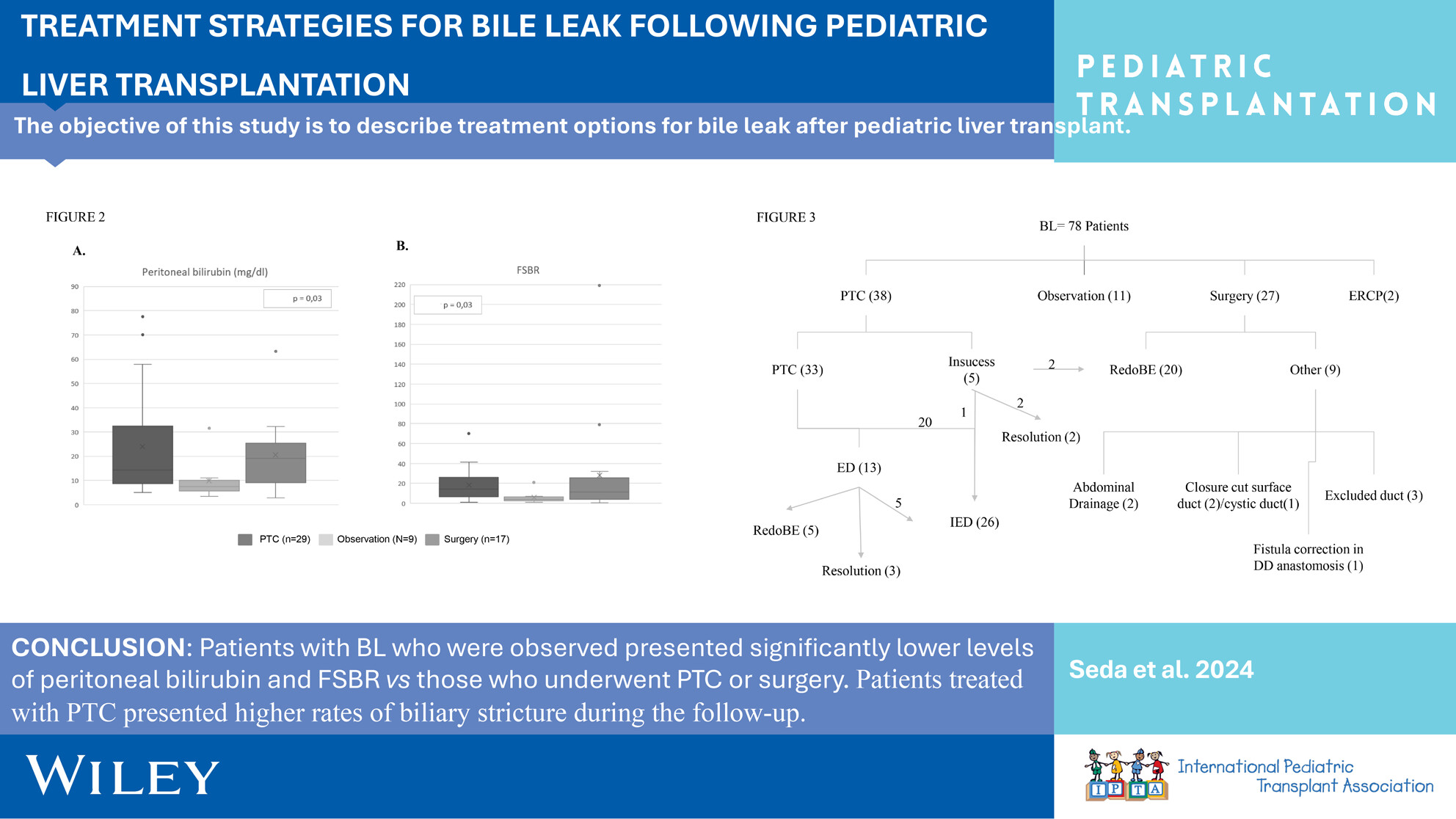
Patients with bile leak who were observed presented significantly lower levels of peritoneal bilirubin and peritoneal fluid-to-serum bilirubin ratio versus those who underwent percutaneous transhepatic cholangiography (PTC) or surgery. Patients treated with PTC presented higher rates of biliary stricture during the follow-up.
-
Kidney Transplantation in ≤15 kg Children: Outcomes and Prognostic Indicators—A Review of the Organ Procurement and Transplantation Databaseoa
Graphical Abstract
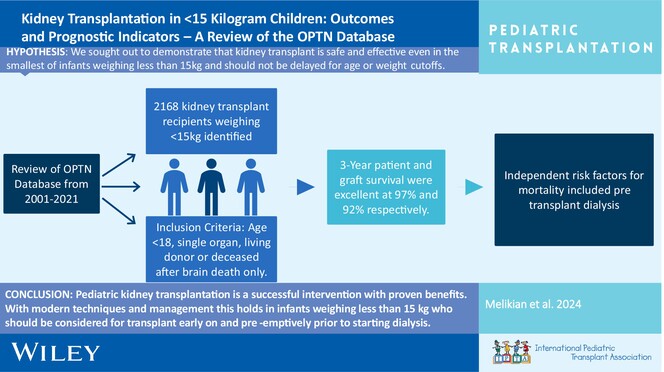
Pediatric kidney transplantation is a successful intervention with proven benefits. With modern techniques and management, this holds in infants weighing <15 kg who should be considered for transplant early on and if possible prior to starting dialysis.
-
Association of HLA B- and T-cell molecular mismatches with HLA antibodies, rejection, and graft survival in pediatric kidney transplantationoa
Graphical Abstract
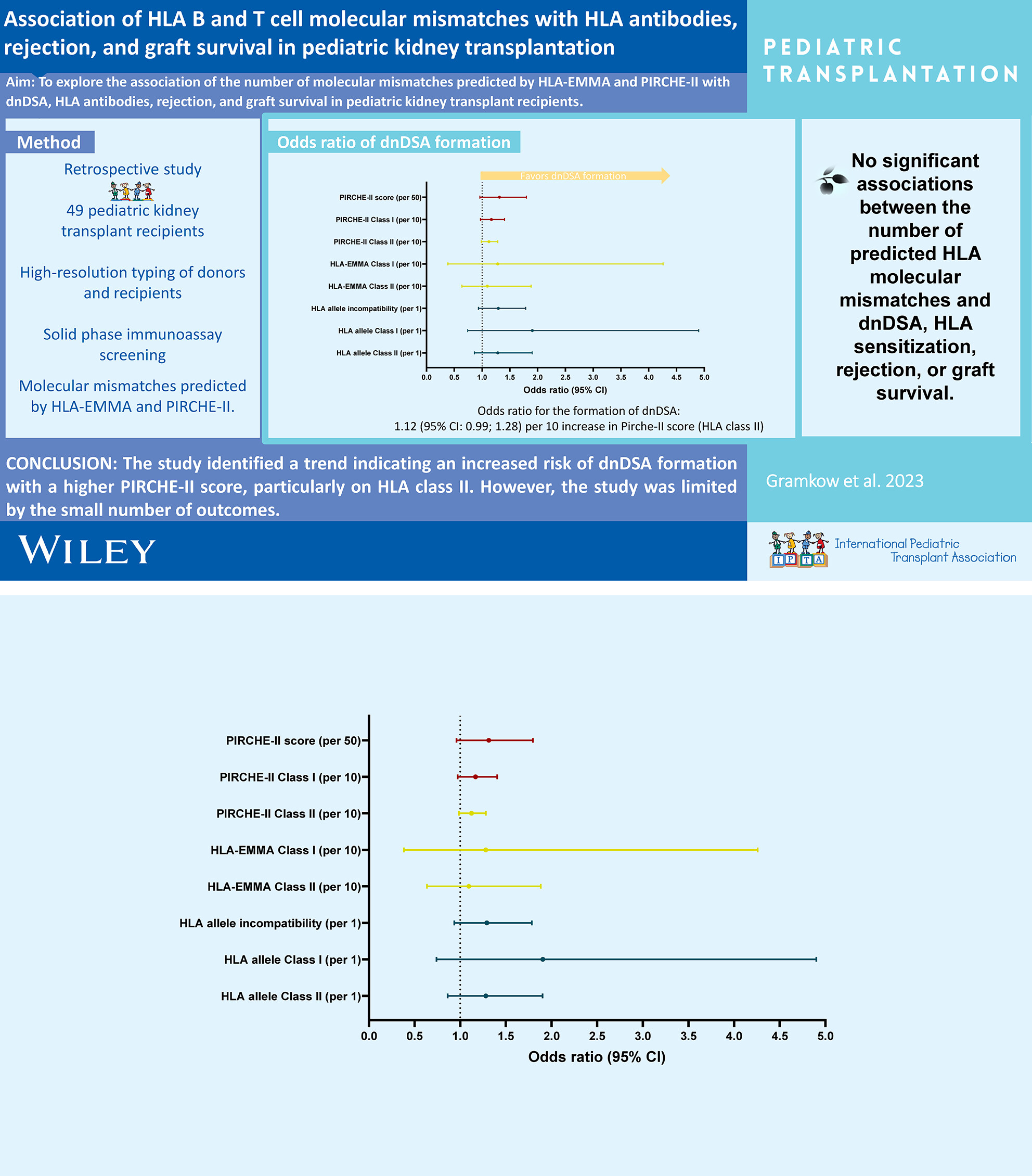
No associations were found between PIRCHE-II or HLA-EMMA and outcomes, but a trend toward increased odds of de novo donor-specific antibody formation with higher PIRCHE-II scores was noted. However, limited outcomes preclude definitive conclusions.
-
BK polyomavirus DNAemia, allograft rejection, and de novo donor-specific antibodies after lowering target tacrolimus levels in pediatric kidney transplant recipientsno
Graphical Abstract
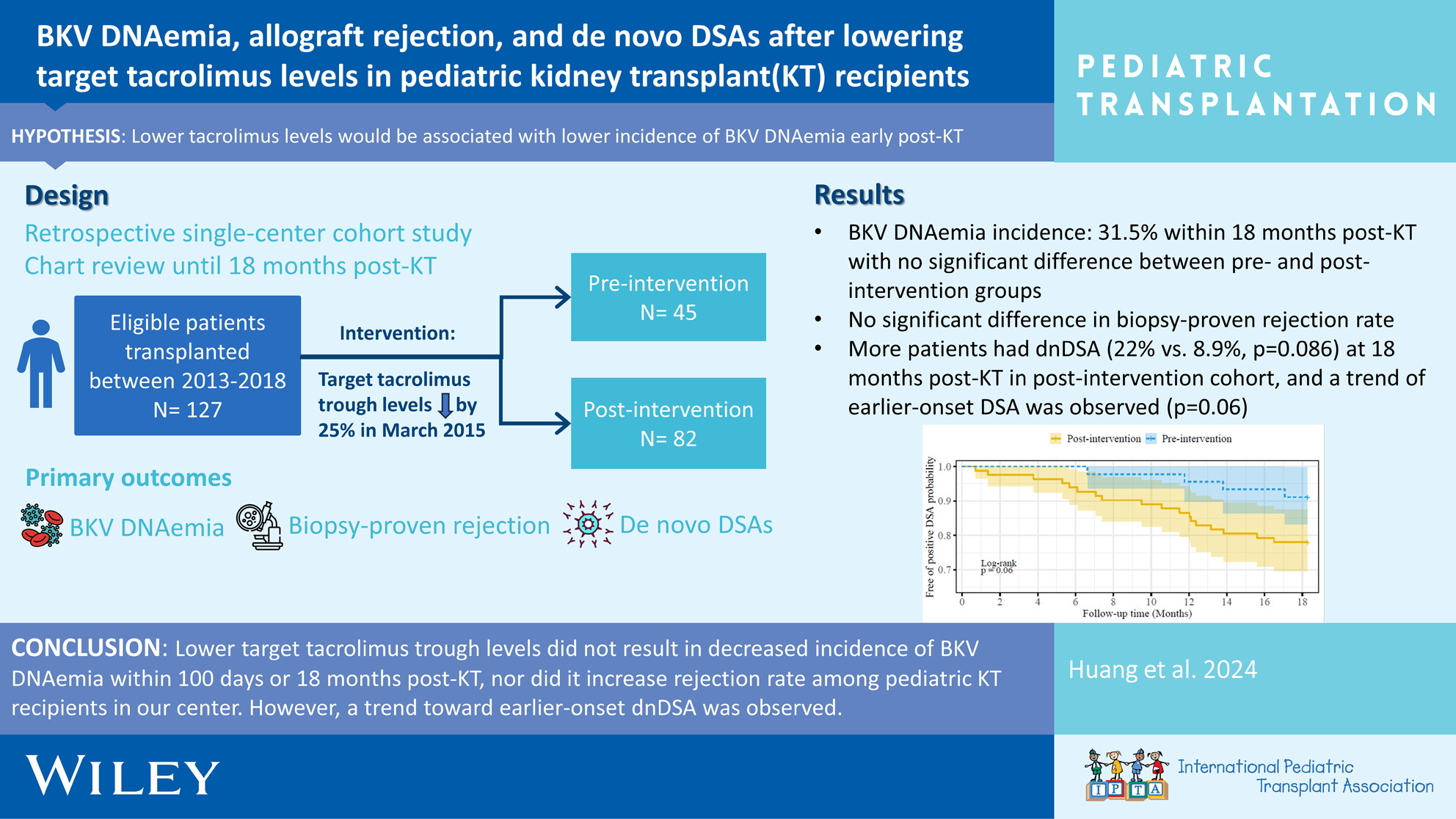
Early BKV DNAemia is common post-pediatric kidney transplant, especially in younger ages, with ~30% incidence within 18 months post-transplant. Favorable outcomes are achieved with (1) frequent monitoring of viremia and (2) timely reduction of immunosuppressive medications, which must be balanced against risk of rejection and development of HLA antibodies.
-
Alemtuzumab induction is associated with decreased hospitalization rates in pediatric kidney transplant: A UNOS data review for safety and outcomes with common induction regimensno
Graphical Abstract
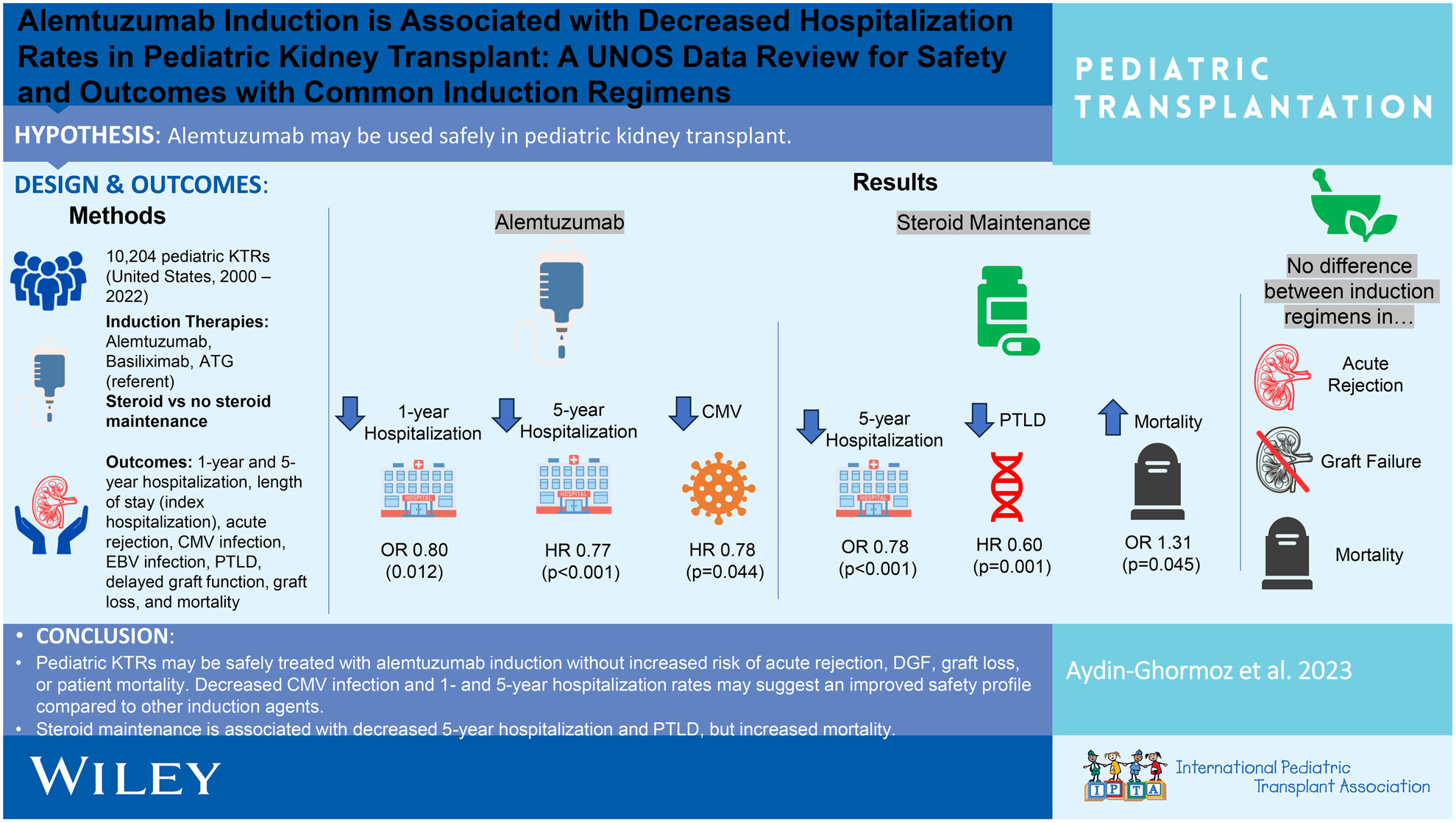
Pediatric KTRs may be safely treated with alemtuzumab induction without increased acute rejection, delayed graft function, graft loss, or patient mortality, but with decreased CMV infection and 1 and 5 years hospitalization rates. Steroid maintenance is associated with decreased 5 years hospitalization and PTLD, but increased mortality.