


All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Pneumocystis jiroveci Pneumonia Infections in Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
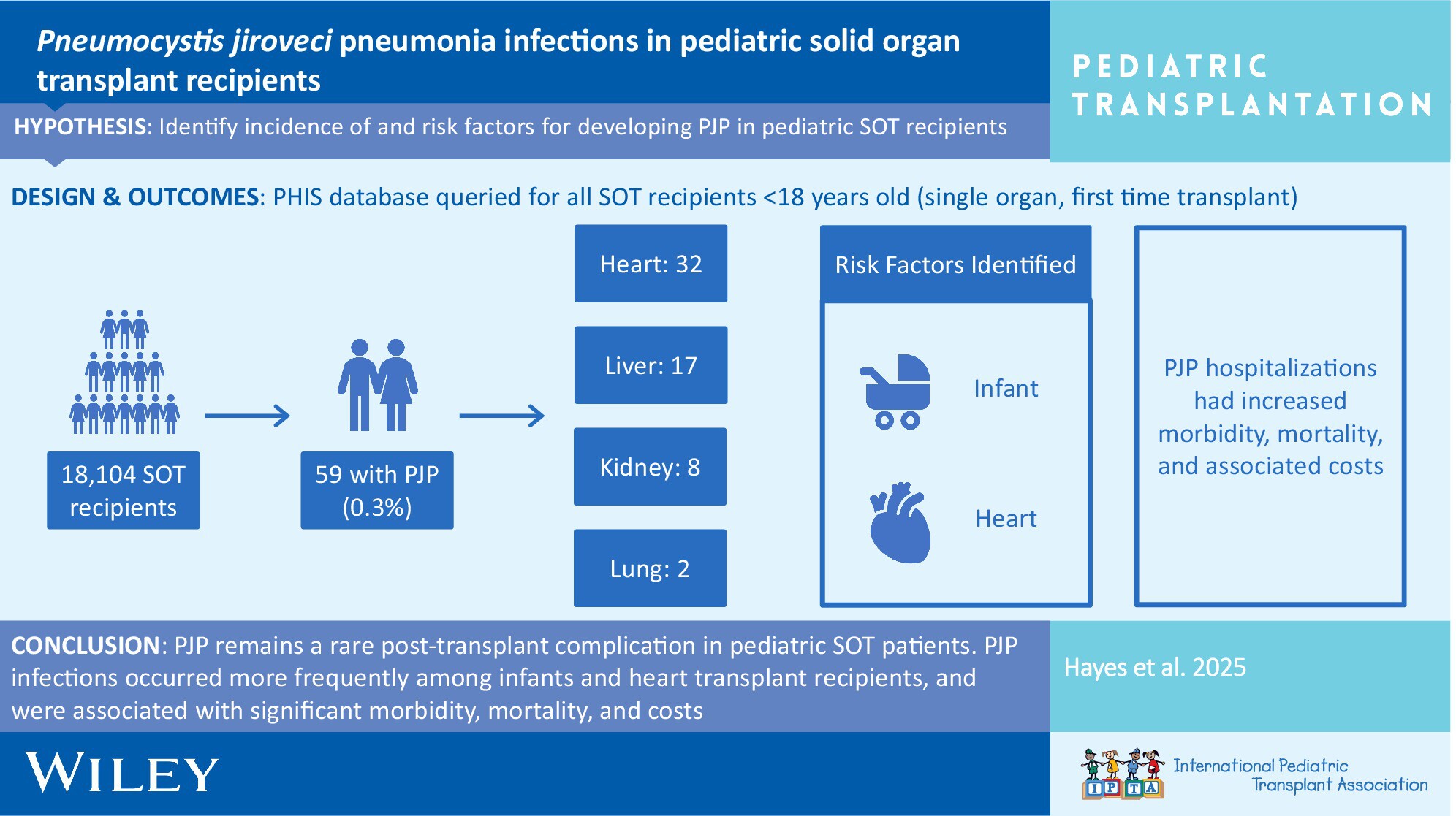
In the current era, PJP remains a rare post-transplant complication in pediatric SOT patients. PJP infections are associated with significant morbidity, mortality, and costs. Risk factors for PJP are young age at transplant and heart transplantation. An assessment of individual risk factors should be regularly performed to optimize prevention strategies.
-
Association of Neutropenia With Valganciclovir Prophylaxis Dosing Practices Within Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
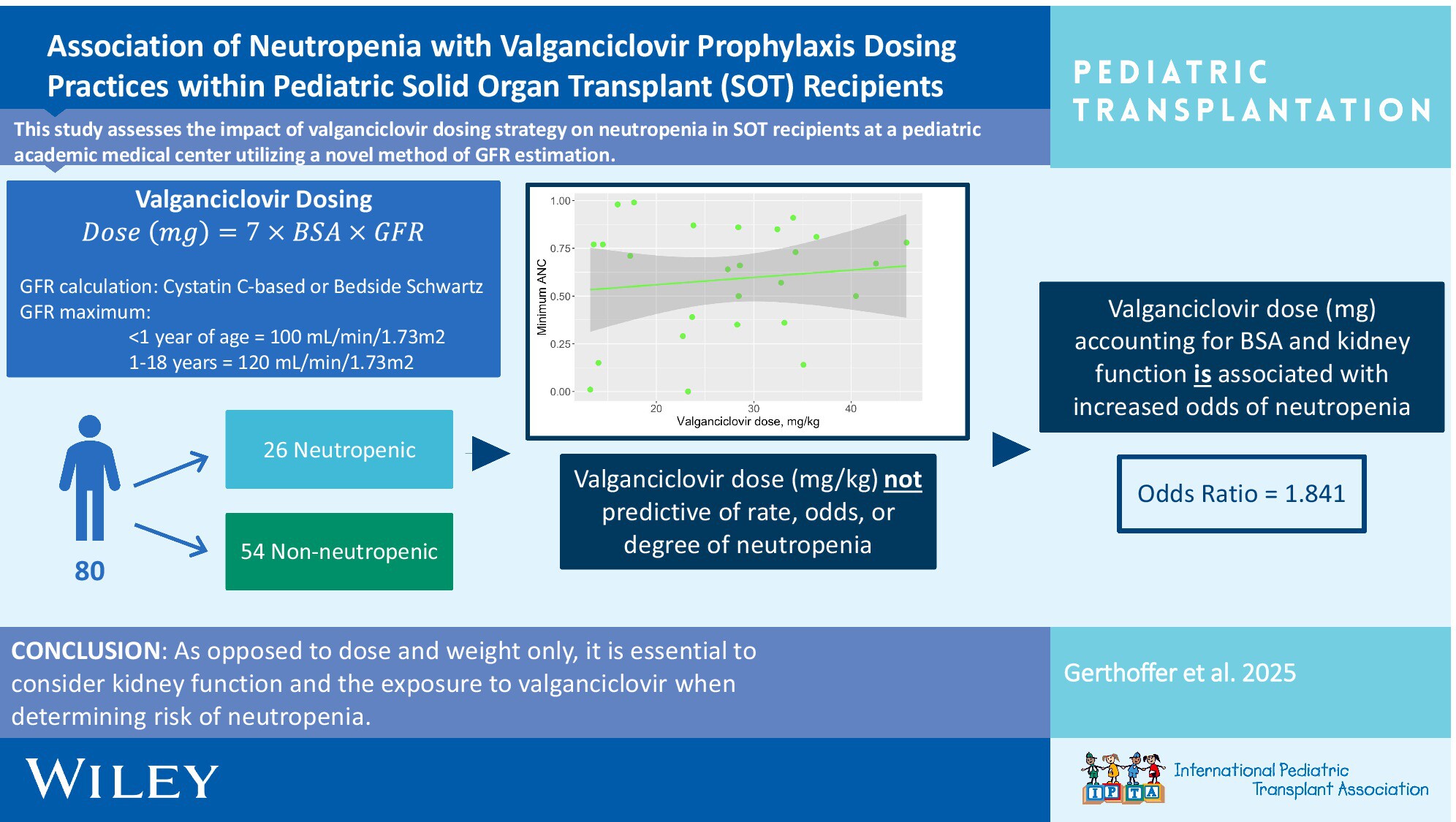
It is crucial to consider kidney function and the exposure to valganciclovir vs. dose alone when determining the risk of neutropenia in pediatric solid organ transplant recipients. Utilizing BSA-based dosing, Cystatin C-based GFR estimation, and appropriate upper limits of GFR for age was associated with a lower rate of neutropenia.
-
Impact of Pharmacogenomic Testing in Pediatric Heart and Kidney Transplantno
Graphical Abstract
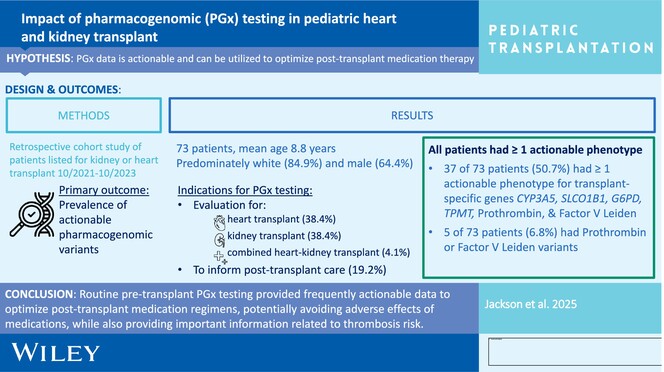
Routine pretransplant PGx testing provides frequently actionable data to optimize posttransplant medication regimens, potentially avoiding adverse effects of medications including tacrolimus, azathioprine, HMG-CoA reductase inhibitors, and dapsone, while also providing important information related to thrombosis risk for VTE prophylaxis.
-
The Impact of Reduced Immunosuppression on Alloimmunity: A Retrospective Study of Pediatric Kidney Transplant Recipientsoa
Graphical Abstract
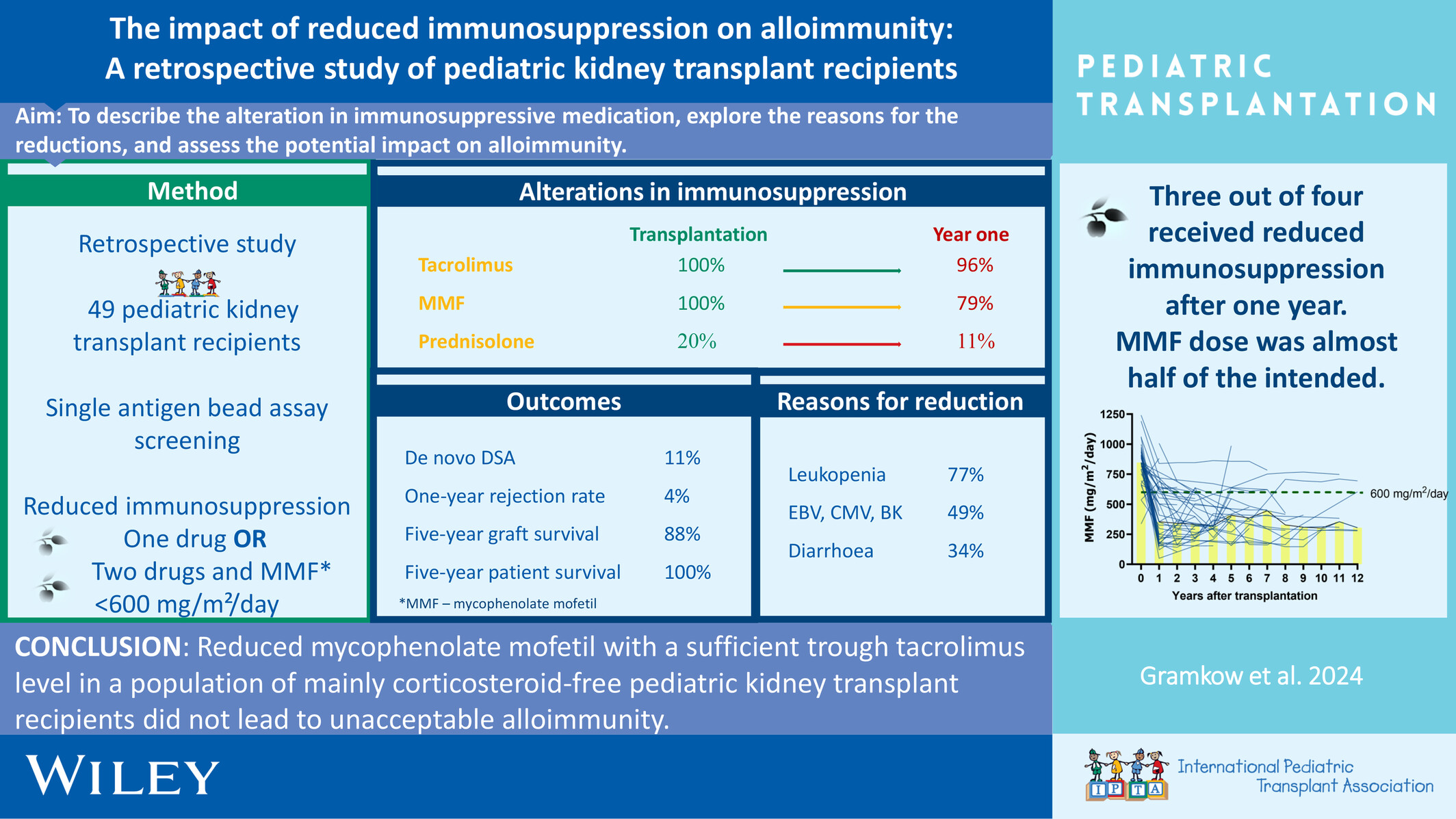
Reduced mycophenolate mofetil with a sufficient trough tacrolimus level in a population of mainly corticosteroid-free pediatric kidney transplant recipients did not lead to unacceptable alloimmunity.
-
Norovirus Management and Outcomes in a Multicenter Pediatric Kidney Transplant Populationoa
Graphical Abstract
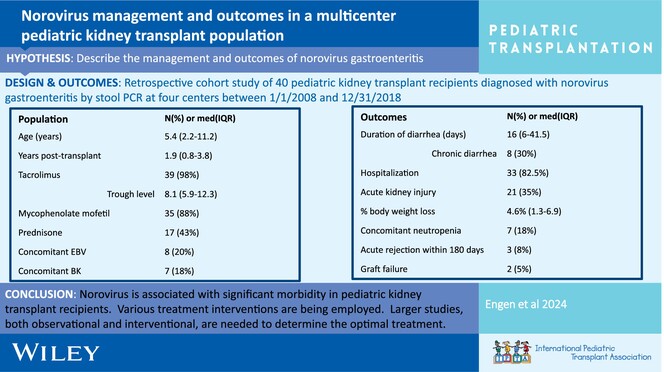
Post-transplant norovirus diarrhea persists for a median of 16 days (IQR 6–41.5 days) with 30% of patients developing chronic diarrhea. Morbidity is high, including AKI in 53% of patients, reduction in immunosuppression 20%, and acute rejection in 8% within 6 months of diagnosis.
-
Treatment outcome at the pediatric stem cell transplantation center in Syria: A single-center experienceno
Graphical Abstract
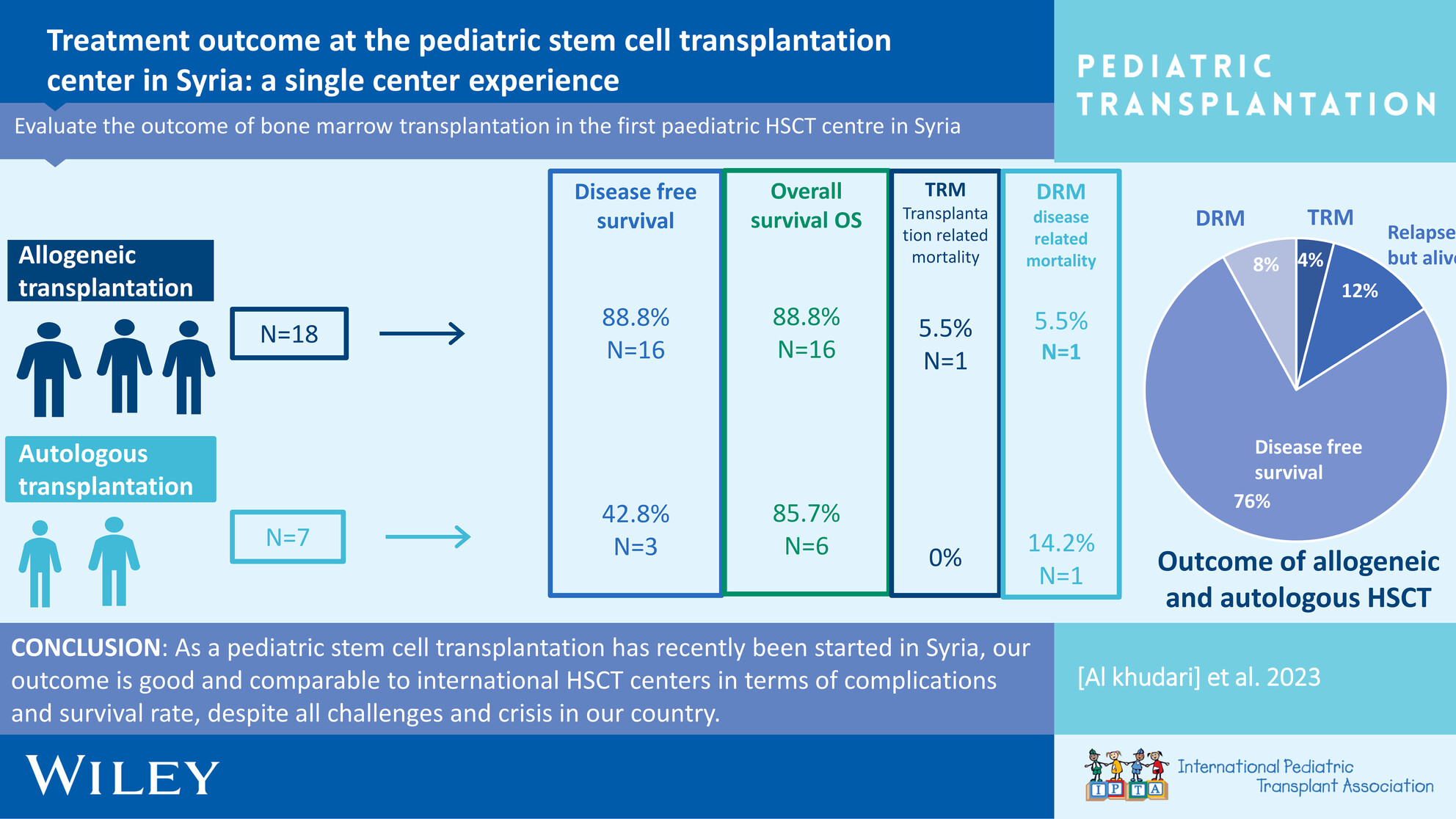
In autologous patients, transplant-related mortality (TRM) was 0%, with 4 (57%) experiencing disease relapse, resulting in the death of one patient. Additionally, 3 (42.8%) of patients remain alive under second-line management. The overall survival rate was 6 (85.7%), and the disease-free survival rate was 16 (88%). In allogeneic patients, TRM was 5.5% (1/18). One allogeneic patient experienced disease relapse and subsequently died. The overall survival rate and disease-free survival rate were 16 (88%). The objective of this study was to assess the outcomes of pediatric hematopoietic stem cell transplantation (HSCT) patients who have undergone transplantation thus far.
-
Calcineurin inhibitor-related hyperkalemia is caused by hyporeninemic hypoaldosteronism and fludrocortisone is an effective treatment: Report of a case series and review of the literatureno
Graphical Abstract
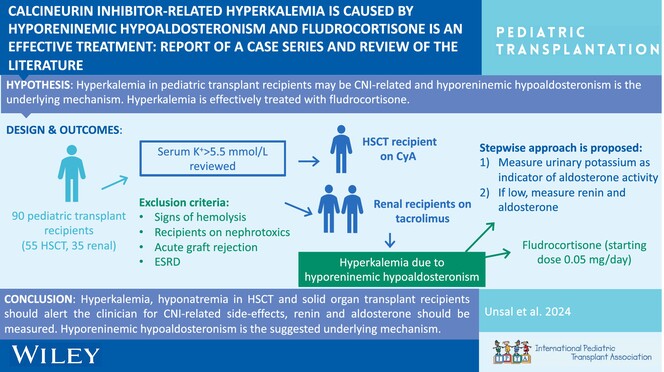
Hyperkalemia and hyponatremia in HSCT and solid organ transplant recipients should alert the clinician for CNI-related side effects; renin and aldosterone should be measured. Hyporeninemic hypoaldosteronism is the suggested underlying mechanism.
-
Pregnancy after transplant in the older adolescent: Anticipatory guidance for the pediatric providernoCollections: Special Issue on Adolescence and Transplantation
Graphical Abstract
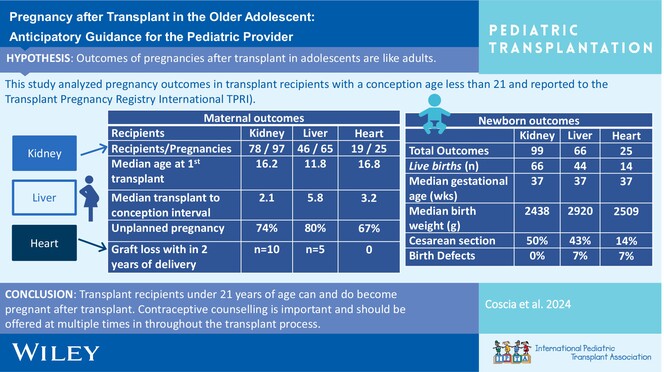
This manuscript will provide a brief review of current recommendations for contraception for adolescent and young adult solid organ transplant recipients, a short review of immunosuppression and pregnancy exposure, overview of outcomes in recipients who had a pregnancy before age 21 years, and pregnancy outcomes in the general transplant population.
-
The humoral immune response to the BNT 162B2 vaccine in pediatrics on renal replacement therapyno
Graphical Abstract
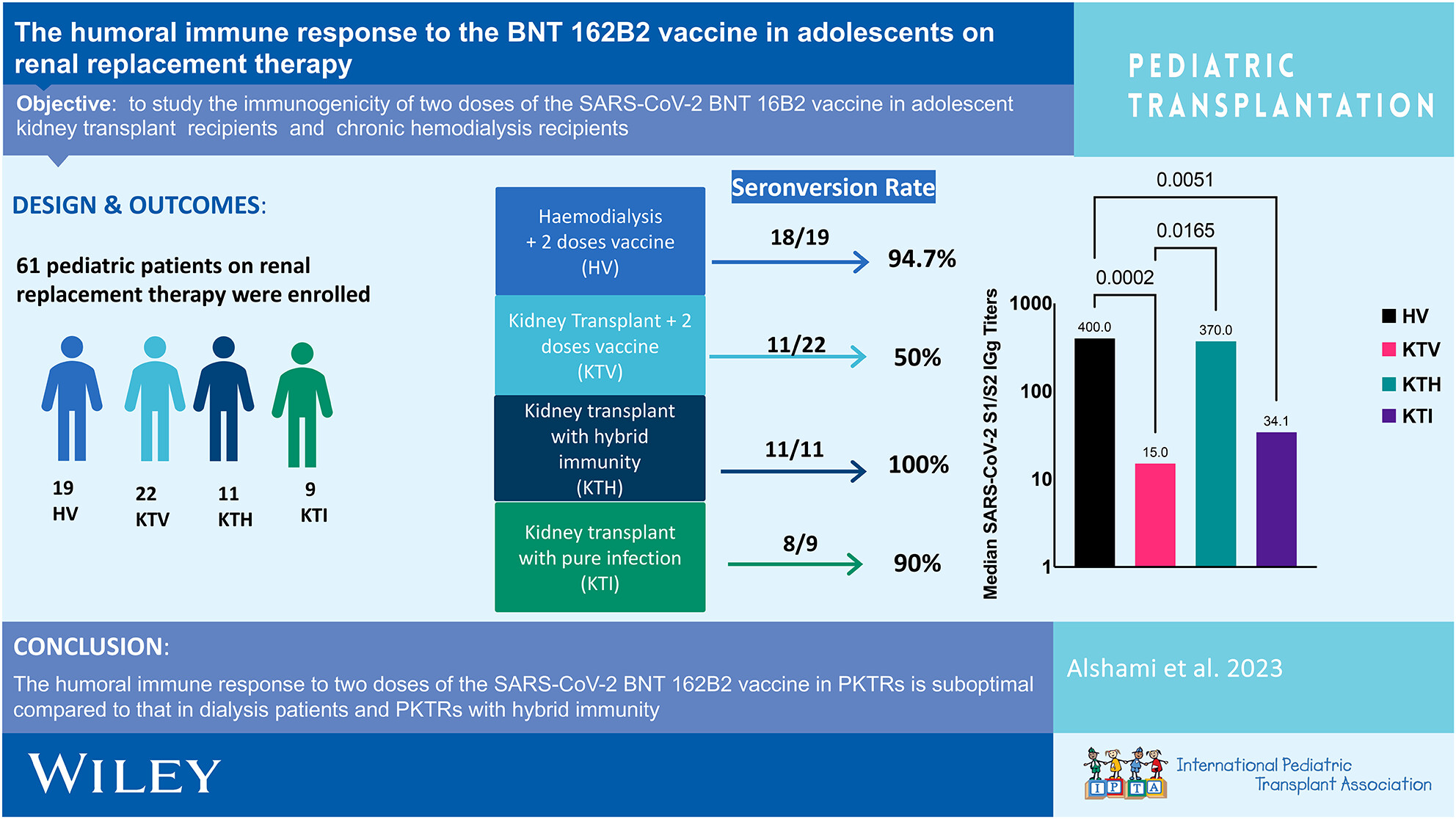
The humoral immune response to two doses of the SARS-CoV-2 BNT 162B2 vaccine in PKTRs is suboptimal compared to that in dialysis patients and PKTRs with hybrid immunity.