Cutaneous larva migrans in early infancy: A Ugandan case report
Abstract
Helminths are an important cause of worm infestation in low-income countries. The majority spread with soil to skin contact. In unusual patients presenting below 1 year, treatment can be challenging. The disease can be self-limiting; however, treatment is believed to reduce progression to more serious disease. Here, we present a case of a 3-month-old with cutaneous larva migrans.
1 INTRODUCTION
Cutaneous larva migrans (CLM) is a clinical syndrome consisting of an erythematous migrating linear or serpiginous cutaneous track.1
This creeping eruption most frequently occurs as a result of human infection with the larvae of the dog or cat hookworms, Ancylostoma braziliense or Ancylostoma caninum; it also may be caused by larvae of other animal parasites that are not natural human parasites.2 Cutaneous larva migrans also occurs with infective filariform larvae of human hookworms Ancylostoma duodenalis and Necator americanus.
Hookworm infections are common in the tropics and subtropics. The prevalence of hookworm infection is highest in sub-Saharan Africa. Individuals at greatest risk include travelers, children, swimmers, and laborers whose activities bring their skin in contact with contaminated soil.3
Eggs are passed in the stool, mature into larvae that penetrate the skin on human contact and are carried through the blood vessels to the lungs, where they penetrate into the pulmonary alveoli, ascend the bronchial tree to the pharynx, and are swallowed. The larvae reach the small intestine, where they reside and mature into adults, which attach to the intestinal wall. The larvae produce an inflammatory reaction along the cutaneous tract of their migration, which may continue for weeks, pulmonary involvement occurs, and intestinal colonization.4 This results in allergic severe pulmonary symptoms and anemia and chronic nutritional impairment.
Treatment with anthelminthic therapy is helpful for relieving symptoms and reducing the likelihood of bacterial superinfection. However, the available options are usually contraindicated in infants or hard to find. In this report, we present a different treatment approach in a case of a 3-month-old infant with CLM.
2 CASE DESCRIPTION
2.1 Clinical history
Male infant, 3 months of age who was well prior to this incident as reported by the mother, presented with a thread-like path below the skin on the left part of the abdomen. The mother noticed the lesion while bathing the child, and by the time of the clinic visit, it had persisted for 24 h. The lesion had not moved during this time. Mother reported an outing with the child to the garden the previous morning with an estimated 4 h of stay during which time the child had been placed on bare ground. The child had been restless during sleep hours but was still able to breastfeed and had no cough or fever. Mother had not applied anything to the lesion by the time of the clinic visit.
2.2 Clinical examination
2.2.1 General examination
Good general condition, irritable, respiratory rate of 28 cycles per minute, pulse rate 93 b/m regular and synchronous in both arms, axillary temperature 37.0°C. No pallor of the conjunctiva, sclera anicteric, no palpable lymphadenopathy and no pedal edema. Weight of 4.8 kg appropriate for age.
2.2.2 System examination
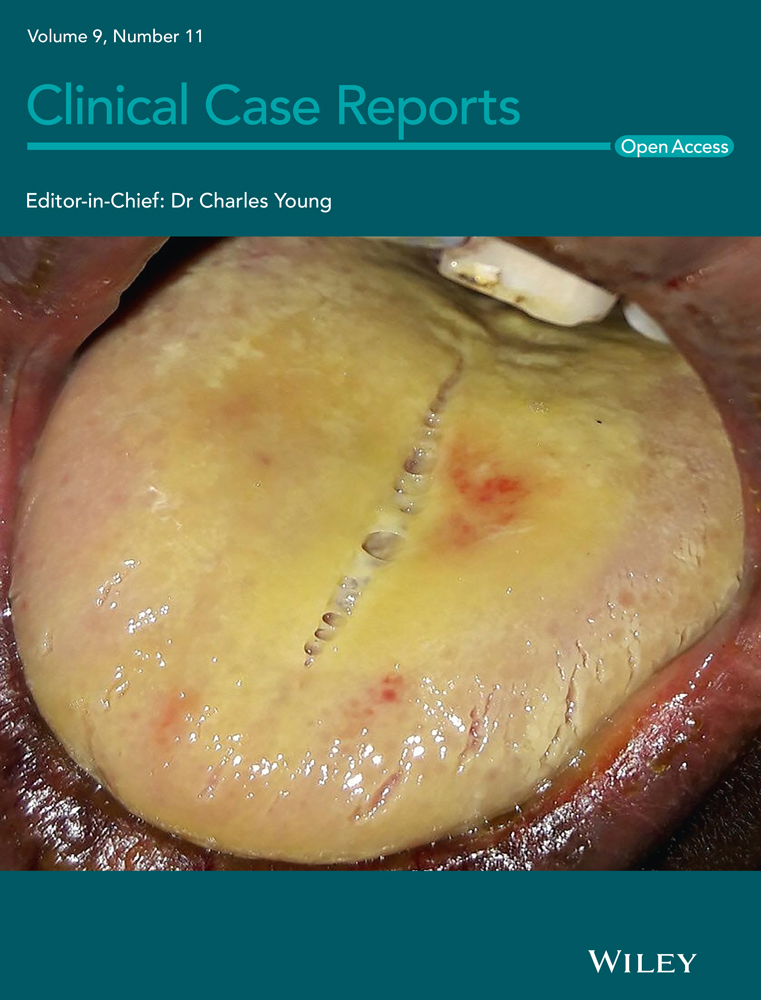
The abdomen was of normal distension, moving with respiration. There was a single raised, thread-like serpiginous lesion, stationary, with erythema, about 32 cm in length on the left lateral abdomen (lumbar region). No entry point could be identified. Abdomen was soft with no palpable organomegaly. An anal examination revealed no abnormalities.
Chest examination was clear, and heart sounds 1 and 2 were heard with no added sounds (Figure 1).

2.3 Laboratory investigation
Stool analysis was negative for ova or larvae.
Complete blood count was not done.
2.4 Management, outcome, and follow-up
10% albendazole applied topically twice daily for 7 days. Three 400 mg tablets were crushed and mixed in the measured 12 g of petroleum jelly.
There was no further change in the position of the lesion 3 days after treatment initiation; lesion disappeared completely by 7 days.
Mother counseled on hygiene.
3 DISCUSSION
Soil-transmitted helminth infections are among the most common infections worldwide and affect the poorest and most deprived communities.5 A countrywide description of the distribution of soil-transmitted helminths in Uganda is reported, based on data for 20 185 school children from 271 schools. The overall prevalence of Ascaris lumbricoides, Trichuris trichiura, and hookworm was 6.3%, 5.0%, and 43.5%, respectively.6
The global strategy for the control of soil-transmitted helminthiasis is based on regular anthelminthic treatment as one of the four pillars.7
The preferred treatment is ivermectin (200 mcg/kg orally once daily for 1 or 2 days).8 Safety data on the use of ivermectin in infants less than 15 kg are still limited,9 and the drug is thus not part of the WHO recommendations for treatment of helminths below the above weight category.
Albendazole (400 mg orally with a fatty meal for 3 days) is an alternative treatment. In 2002, a WHO Informal Consultation concluded that albendazole and mebendazole are safe for administration to children aged 12 months and older. There are no data on the use of these drugs in children aged under 12 months. Therefore, children under 12 months of age should not be treated (unless indicated by a physician in a clinical setting).10
Some guidelines include the use of mebendazole in children as young as 6 months.11 A double-blind, placebo-controlled, randomized trial by Motressor et al., 2002 in children under 24 months showed no statistical significance in the incidence of adverse effects in the treatment and control groups receiving mebendazole (500 mg).12 WHO recommends 200 mg in children below 24 months.13
Topical agents are an alternative treatment option, though they can be difficult to obtain. A case report of CLM treatment using topical anti-helminth therapy in an infant 2 months of age supports this approach.14 We treated our patient with clinic made 10% albendazole from three 400 mg tablets mixed in measured 12 g of petroleum jelly. This was done because of limited data on the use of anti-helminth therapy in infants less than 6 months and the need to reduce side effects. This agrees with a case report by Eric Caumes et al.15 on the efficacy of albendazole ointment on cutaneous larva migrans in two young children.16
4 CONCLUSION
Cutaneous larva migrans is a commonly encountered entity in sub-Saharan Africa. However, limited data exist on the safety of existing anti-helminthic therapy in the management of infants especially those below 6 months. Available options are also scarce to find in a low-resource-limited setting posing a challenge to the management of these cases. We presented a case of a 3-month-old infant who attained complete resolution of a cutaneous larva migrans using topical albendazole therapy.
ACKNOWLEDGEMENT
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
Eria Muwanguzi wrote this case report. Mubaraka Kayiira, Derrick Kasozi, and Enos Kigozi assisted in writing the discussion.
ETHICAL APPROVAL
Verbal consent was given by the mother, and the identity of both the mother and baby remains concealed.
CONSENT
Published with written consent of the patient.
Open Research
DATA AVAILABILITY STATEMENT
The data of the child can be found at Luuka Health Centre 4, Luuka.