Delayed presentation of congenital rectal stenosis associated with Down's syndrome and hypothyroidism: Case report
Funding information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. No competing financial interests exist
Abstract
Rectal stenosis is a rare variety of rectal atresia. A membrane separates the rectum from the anal canal in the presence of a normal anus. We report a case of rectal stenosis associated with Down's syndrome and hypothyroidism in whom rectal stenosis was diagnosed at the age of 17 years.
1 INTRODUCTION
Rectal atresia is a rare type of anorectal malformation (ARM) that constitutes 1%–2% of the ARM.1 Rectal stenosis or type-I rectal atresia is the rarest type of rectal atresia. It is defined as an atresia with a central holed septal defect.1, 2 In most cases of rectal stenosis, the anus is normally located and the stenosis is usually 1–2 cm deep with the presence of a dilated upper rectum. The lower part of the rectum empties into a narrow anal canal.3 There are also a report of combined rectal atresia and stenosis.4 A case of rectal stenosis associated with imperforate anus and recto-prostatic urethral fistula has also been reported.5 However, in most published literatures on rectal atresia or stenosis, the presentations were early in lives and there were few associated anomalies.1, 6, 7 We report a case of delayed presentation of congenital rectal stenosis at an age of 17 years who had associated Down's syndrome and hypothyroidism.
2 CASE REPORT
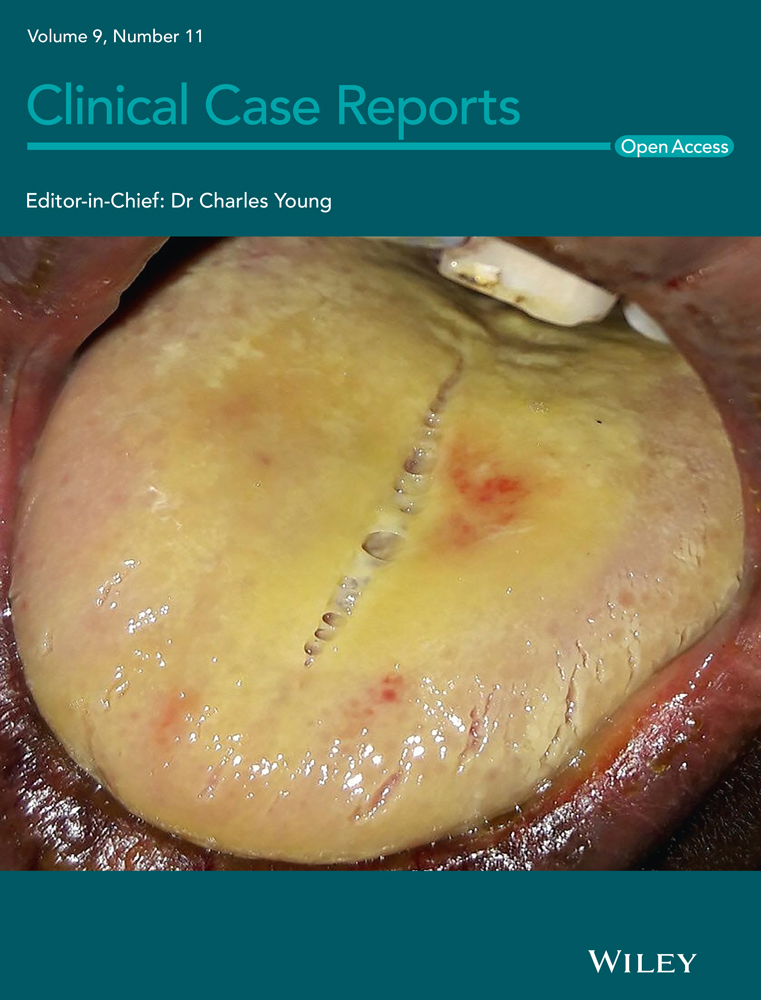
A 17-year-old girl from non-consanguineous parents of a lower middle-class family presented with a history of recurrent constipation since her early childhood. Prenatal ultrasound did not show any abnormality. Meconium passed within 24 h of life, and there was no history of post-natal rectal probing. She developed features of constipation after weaning at about 6 months of age and visited several doctors since then. Eventually, she was diagnosed as a case of Down's syndrome and hypothyroidism by a pediatrician at the age of 1 year and was put on thyroxin. Her constipation had been managed with dietary measures and enemas. During early childhood, she used to pass stool every 2–3 days, but the interval gradually increased to 5–6 days later on. During the later years, she did not pass stool without enema or laxatives. She used to pass small volume, hard stool in pieces that sometimes became liquid after taking enema or laxatives. With increasing age, she developed reluctant to feed, often remained withdrawn and sad. She was referred to a pediatric surgeon at the age of 17 years to address the issue of constipation, when we came into contact of the patient. She did not pass stool for the last 9 days at the time of referral. She weighed 35 kg and was 134 cm tall. On general examination, she had a flattened face with a broad nasal bridge, low set ears, a large tongue that frequently protruded out of the mouth, a short neck and a low intellectual ability. The abdomen was slightly distended and mildly loaded with fecal matter. An abdominopelvic ultrasonography revealed no presacral mass, and there were no renal or other abnormalities. Barium enema showed a dilated colon and the lower end of the rectum was located high up with a beak-like appearance (Figure 1A). Digital rectal examination (DRE) and examination under anesthesia revealed a thick diaphragm, about 3 cm from anal verge with a central hole, through which hard fecal matter was visible (Figure 1B). Following preoperative colon preparation, under general anesthesia, the girl was catheterized [Foley catheter] and put on lithotomy position. The rectal mucosa was exposed using two Langenbach retractors and the stenosed part was visualized. (Figure 2A). The thick membrane was got hold with Thoms-Allis tissue forceps and was excised circumferentially using monopolar coagulating diathermy. The gap within the rectal mucosa was repaired by using 3/0 atraumatic polyglactin 910 (Vicryl). Histopathological examination of the diaphragm showed fibro-collagenous and fibrovascular tissue (Figure 2B). During the postoperative period, the patient was kept on nil by mouth for 3 days and the subsequent course was uneventful. She was happy to pass normal frequent stools after a few days.


3 DISCUSSION
Rectal atresia usually presents in the neonatal period with abdominal distension.7, 8 The median age was reported to be 1 month.1 However, there are sometimes more delay in diagnosis than other types of ARM because of the presence of a normal anus.1 The reasons for delayed presentation in this case might be related to the associated hypothyroidism, which is frequently associated with constipation that might have misled the clinicians not to search for further surgical cause. The socioeconomic status and associated Down's syndrome might also cause a delay in the diagnosis. Moreover, the patient had a normal looking anus and passed stool through it. This might also mislead the clinicians who treated her earlier not to actively search for an anatomical defect in the anorectum and perform a DRE. There have been reports of ARM, a pediatric problem, to present and to be diagnosed primarily in the adulthood around the world. In majority of these cases, there was an abnormal fistulous opening in the vestibule, vagina, or perineum through which they passed stool. The reasons for the delayed presentations in these cases were reported as family negligence, family problem, social taboo, low-economic condition, low level of education, not seeking medical advice, awareness about physical problems only during the time of decision for marriage, and lack of access to medical care.9-16
Evidences suggest that low socioeconomic status influences one's health and morbidity.17 It affects clinical decision making and healthcare delivery as physicians may delay diagnostic testing, prescribe more generic medications, and avoid referral to specialty care for their patients.18 Many parents also ignore minor symptoms because of the anxiety over the affordability of medical care.17 Although, government provides free medical service to a certain extent, it often involves out-of-pocket expenditure. Specialist care is often very expensive. All these contribute to reluctance for seeking medical care and subsequently delay in definitive management and may cause needless suffering as well as poor outcomes from surgical procedures.19-21 Delayed care in ARMs increases the likelihood of having consequences such as chronic constipation, anemia, malnutrition, and fecal impaction and, thus, may influence the efficacy of surgical intervention.19
Associated anomalies with rectal atresia are usually rare; however, sacral, cardiac and renal anomalies have been reported.22, 23 A study from USA reported that a presacral mass was the most common association.24 However, none of the patients in an Indian series had associated presacral mass.7 There has also been a recent report of hypothyroidism with rectal atresia.25 The differential diagnoses of rectal atresia usually include Hirschsprung's disease, intestinal atresia, colonic atresia, and meconium ileus.7
The exact embryogenic process causing this defect is unknown. However, it has been suggested that it may be caused by vascular accidents between 13 and 14 weeks of gestation or an intrauterine infection causing thrombosis of the vessels leading to atresia of the already formed rectum.7 Racial and genetic causes have also been suggested due to a higher incidence in certain regions among consanguineous marriages.1 The upper pouch is a dilated rectum and the lower part is a small anal canal, which is 1–2 cm deep from the normal location of an anus. These two lumens may be separated by a thin membrane or by dense fibrous tissue.3, 8
Rectal stenosis may be suspected if an 8 or 10 Fr feeding tube or size 11 Hegar dilator cannot be inserted into the rectum in the presence of a normal anus. A contrast enema study is very helpful. These patients also should be screened for the presence of a presacral mass.3, 26 Various surgeries have been described to treat rectal atresia and stenosis.1, 7, 27 Usually, rectal atresia is operated through a posterior sagittal approach after a divided colostomy. The anal canal is split longitudinally and a primary anastomosis is performed between the upper pouch and lower anal canal after excision of the membrane that separates the two canals.3, 27 Rectal stenosis may be treated with a Heineke–Mikulicz type repair.1 Rectal stenosis may also be treated with dilatation if presents early. However, restenosis is common with dilatation only.1 In our case, there was delayed presentation and the thick membrane could be approached through the rectum and was excised. Patients with rectal atresia or stenosis usually have an excellent functional prognosis as there are presence of a well-developed anal canal, normal sensation in the anorectum, and normal voluntary sphincters.3, 28
4 CONCLUSION
The late presentation of this patient's rectal stenosis is probably due to her associated conditions of Down's syndrome and hypothyroidism, which masqueraded the actual cause of constipation. The lower socioeconomic status might also be responsible as they did not seek specialist surgical care from a higher center due to financial constraints. A thorough clinical examination, especially DRE, is mandatory in the evaluation of patients with constipation.
ACKNOWLEDGMENTS
Not applicable.
CONFLICT OF INTEREST
None declared.
AUTHORS CONTRIBUTIONS
Tanvir Kabir Chowdhury made substantial contributions in the design, bibliographic search, and drafted the work. Md. Mozammel Hoque contributed to the draft and revision of the manuscript. Mahfuzul Kabir contributed to interpretation of data and revised the work. Tahmina Banu contributed substantially to the conception, patient selection, design, and revision of the work.
ETHICAL APPROVAL
This study was conducted in accordance with the Helsinki Declaration and its latest amendments. Written informed consent was obtained from the parents of the patients and available on demand. This manuscript is not actually submitted for publication elsewhere.
CONSENT
Written informed consent was obtained from the parents of the patients for publication of this case report and accompanying images.
Open Research
DATA AVAILABILITY STATEMENT
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.