All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Absolute CD3+ T-Cell Counts After Anti-Thymocyte Globulin: Impact on Graft and Infectious Outcomes in Pediatric Kidney Recipientsno
Graphical Abstract
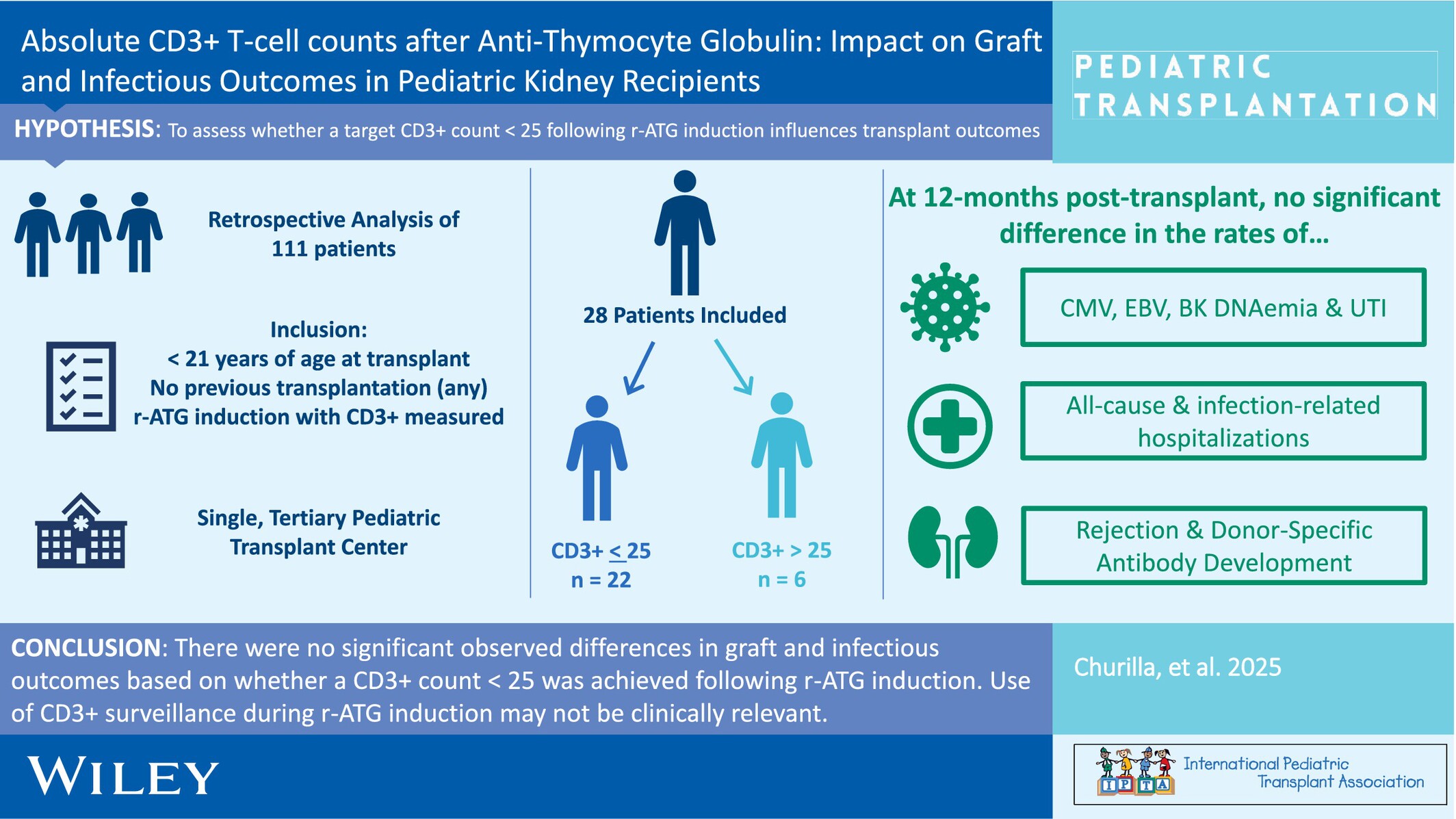
When pediatric kidney transplant recipients were compared based on the achievement (or not) of a CD3+ T-cell count < 25 cells/mm3 following rabbit anti-thymocyte globulin induction, there were no differences in infectious or graft outcomes by 12-months post-transplant.
-
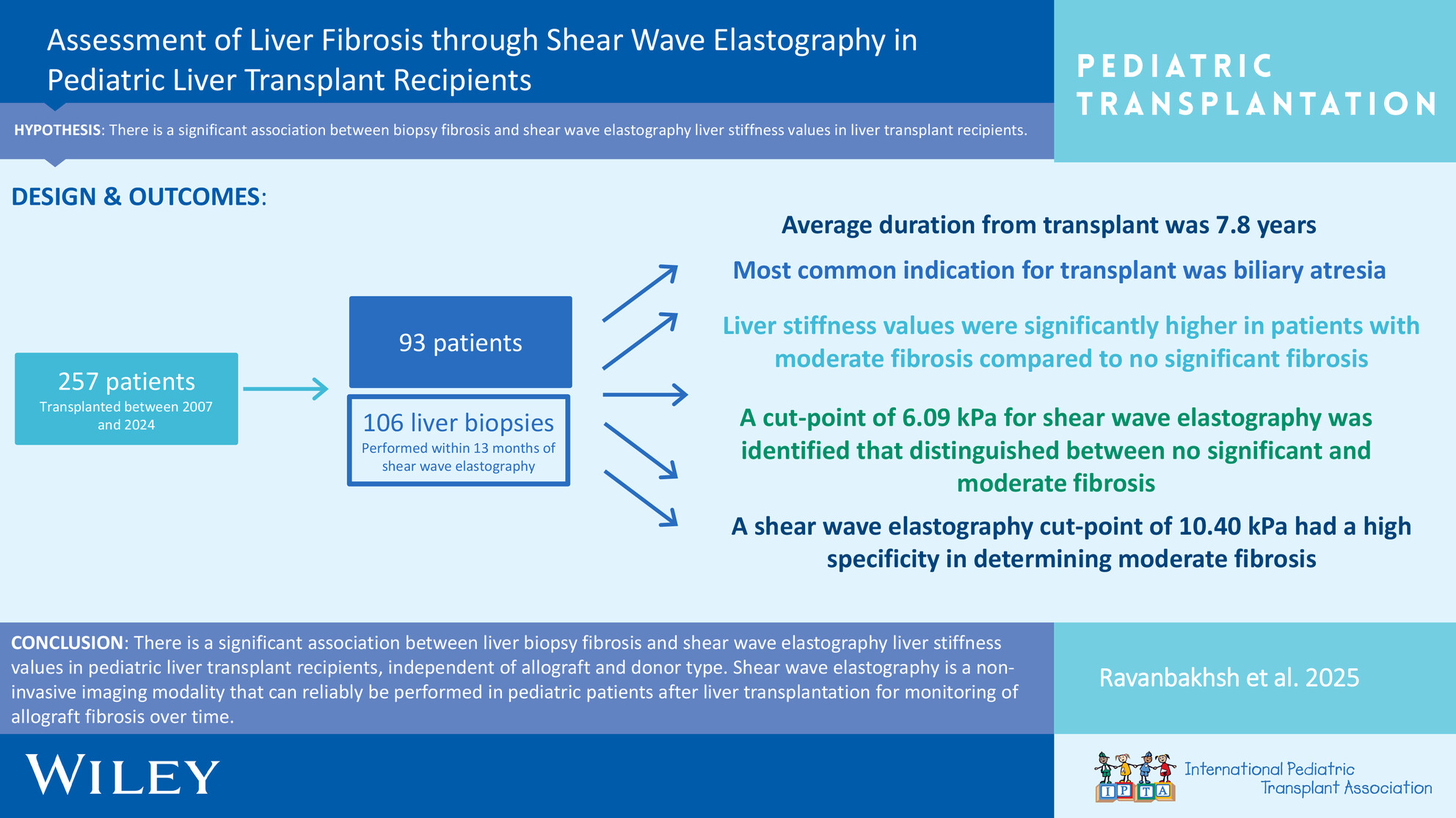
Liver Transplantation in Primary Hyperoxaluria: A Single-Center 10-Year Experienceno
Graphical Abstract
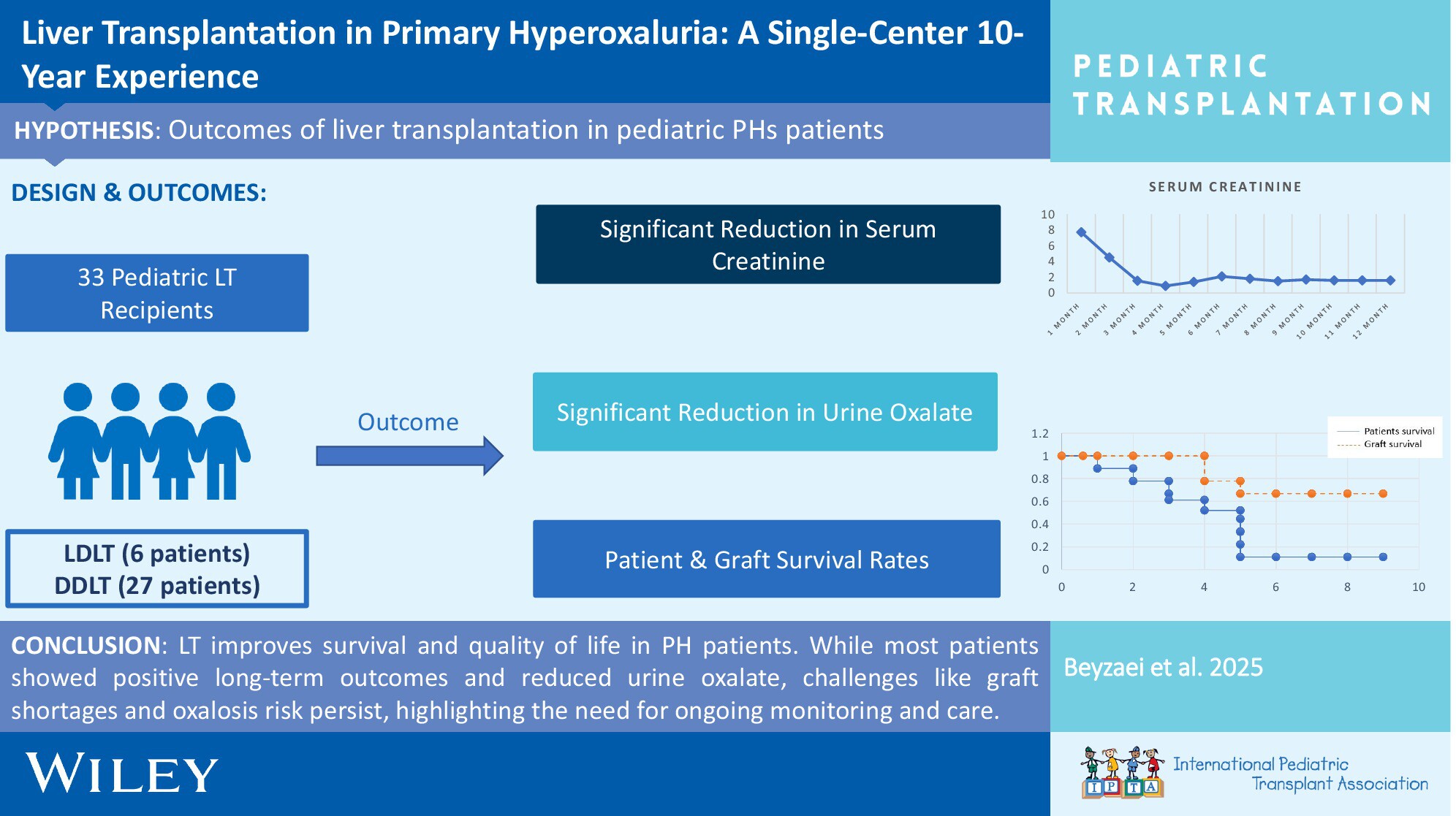
Liver transplantation (LT) significantly improves survival and quality of life for children with primary hyperoxaluria (PH), with favorable long-term outcomes observed in most patients. Despite reductions in urine oxalate levels, challenges such as graft shortages and renal graft loss persist, underscoring the need for ongoing monitoring and care.
-
Combining Acute Kidney Injury Grading and Recovery Mode for Screening in Pediatric Liver Transplantation: A Retrospective Observational Studyno
Graphical Abstract
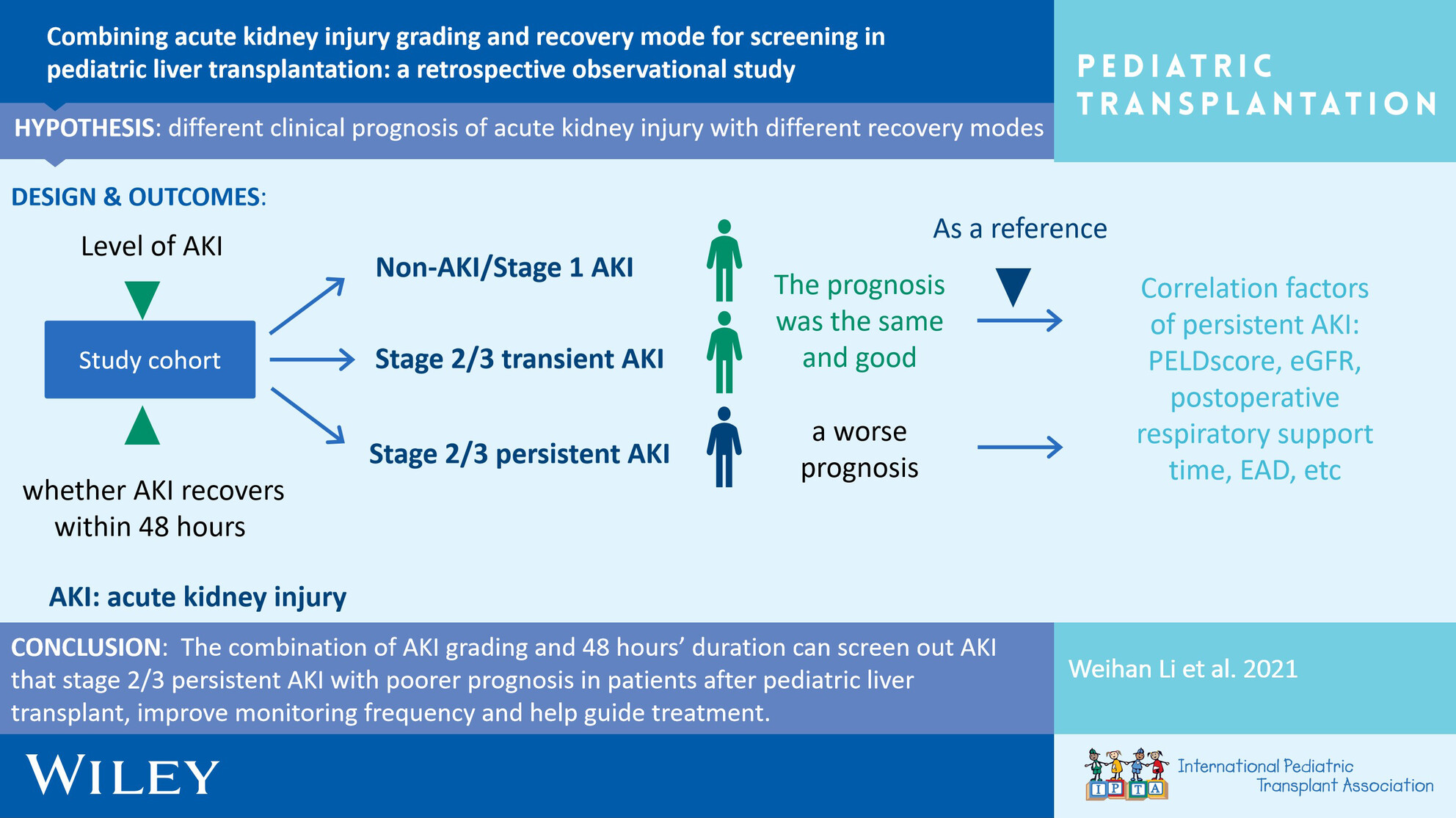
This is a retrospective study to investigate the incidence and clinical prognosis of acute kidney injury and different modes of recovery after pediatric liver transplantation.
-
Absence of Pupillary Reflexes in Pediatric Acute Liver Failure and Neurological Outcome After Liver Transplantationoa
Graphical Abstract
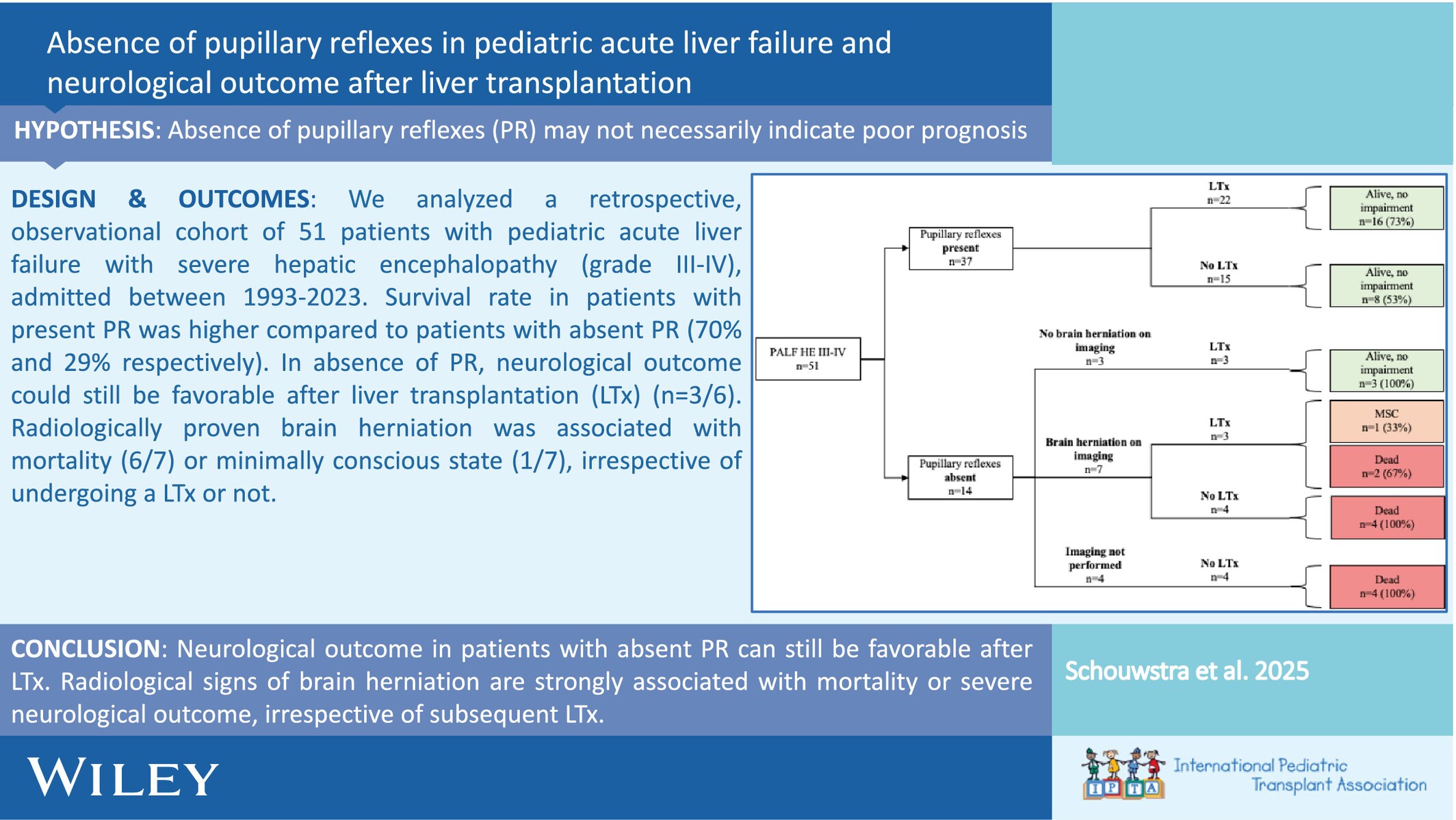
We analyzed a retrospective, observational cohort of 51 patients with pediatric acute liver failure with severe hepatic encephalopathy (grade III-IV), admitted between 1993 and 2023. The survival rate in patients with present PR was higher compared to patients with absent PR (70% and 29%, respectively). In the absence of PR, the neurological outcome could still be favorable after liver transplantation (LTx) (n = 3/6). Radiologically proven brain herniation was associated with mortality (6/7) or minimally conscious state (1/7), irrespective of undergoing a LTx or not.
-
Simultaneous Bilateral Pediatric Nephrectomies: Indications, Approach and Outcomes Over a 15-Year Periodoa
Graphical Abstract
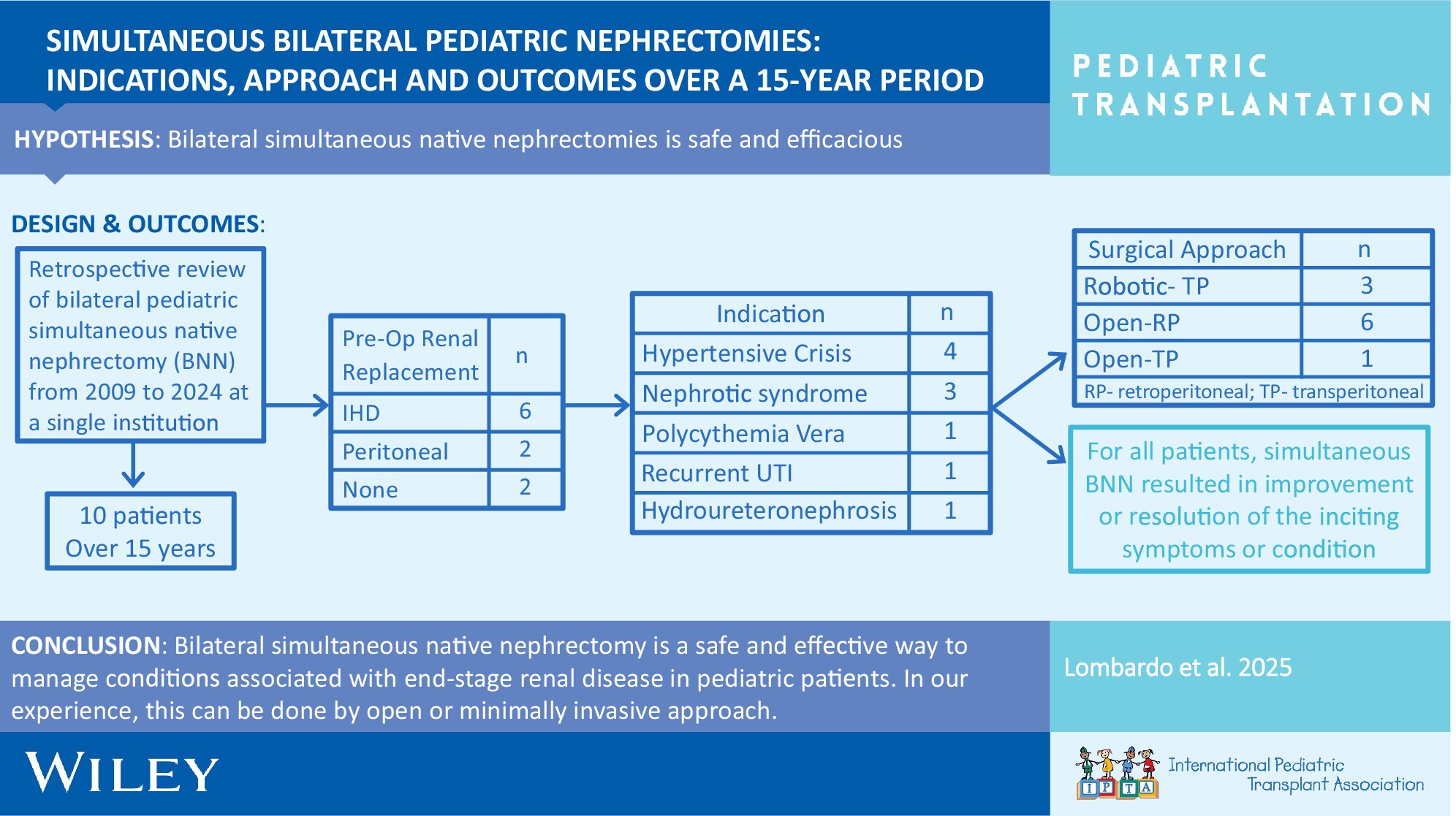
Our single-institution 15-year experience with simultaneous bilateral native nephrectomy (BNN) in pediatric patients demonstrates utility and safety. We discuss considerations of BNN relative to timing of transplantation, an area of conversation. We demonstrate that a minimally invasive approach is feasible, and the surgical approach should consider the route of current or planned dialysis.
-
Procedure Costs Associated With Management of Biliary Strictures in Pediatric Liver Transplant Recipients in the Society of Pediatric Liver Transplantation (SPLIT) Registryno
Graphical Abstract
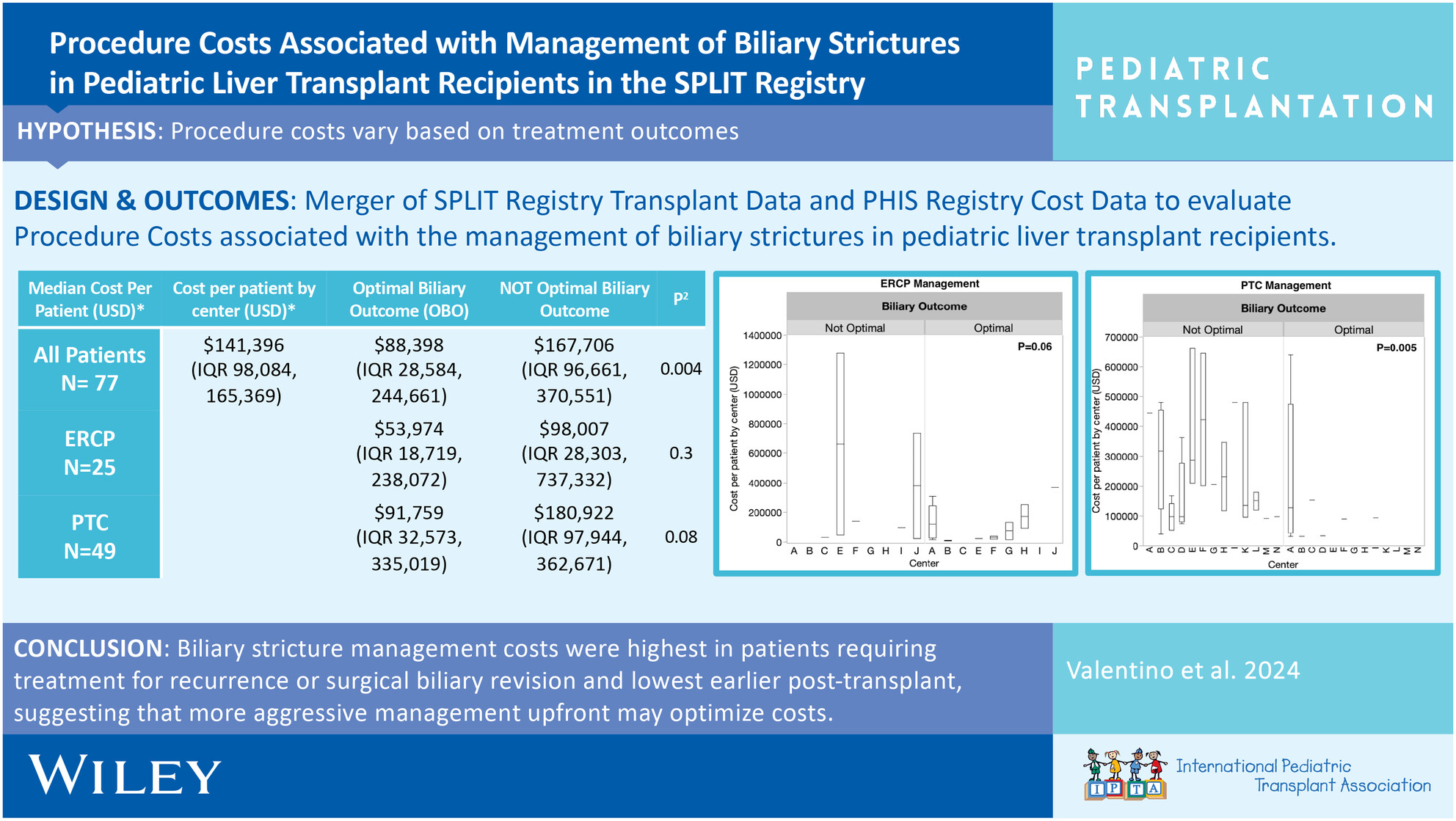
Biliary strictures management costs were highest in patients requiring treatment for recurrence or surgical biliary revision and lowest earlier post-transplant, suggesting that more aggressive management upfront may optimize costs. Future work will explore practice variation and cost-effective strategies to achieve OBO.
-
Short and Long-Term Outcomes of Liver Transplantation in Pediatric Patients With Inborn Errors of Metabolism: A Single-Center Studyno
Graphical Abstract
In our single-center study, we retrospectively analyzed 50 patients who underwent liver transplantation with the diagnosis of IEM. The parental consanguinity rate was 74%. The mean age at liver transplantation was 75.3 ± 8.2 months (range: 5–218), with a follow-up period of 82.1 ± 10.2 months (range:1 day–229 months). Survival rates at 1, 5, 10, and 15 years were 83.7%, 81%, 81%, and 70.9%, respectively. Liver transplantation is an effective solution for children with IEM causing chronic organ failure and difficult to manage with medical treatment, showing good long-term prognosis.
-
Sex-Based Disparities in Heart Transplantation in Teenagersno
Graphical Abstract

Female teenagers have lower survival following heart transplantation than their male counterparts. Male donor—female recipient transplants have the lowest survival among sex-matching groups. The use of organs from oversized or younger donors may be considered to help improve post-transplant survival in teenagers.
-
Evolution of the Florida Pediatric Bone Marrow Transplant and Cell Therapy Consortium (FPBCC): A Statewide Initiative Toward Improving Transplant Outcomesoa
Graphical Abstract
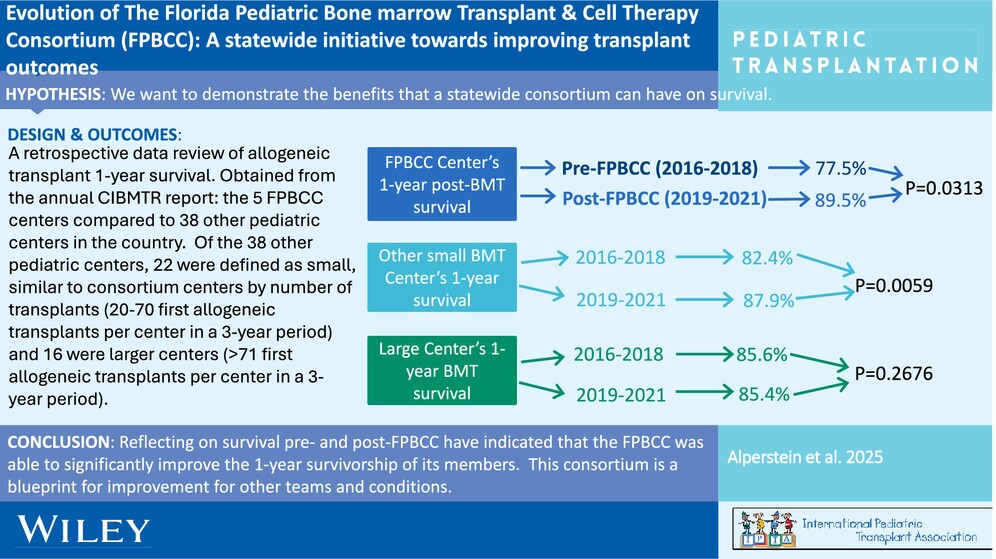
Survival after allogeneic hematopoietic stem cell transplants (aHSCTs) in the state of Florida since the creation of a state pediatric HSCT consortium has improved. This is significant because it demonstrates that small-sized pediatric HSCT centers can work together in a consortium to improve outcomes similar to larger centers.
-
Long-Term Survival in Children Following Heart Transplantationno
Graphical Abstract
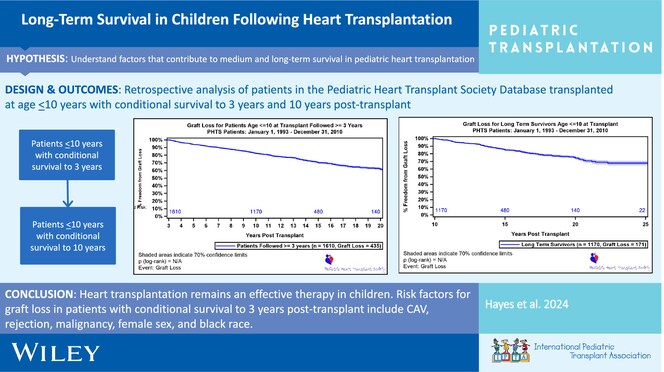
Heart transplantation remains an effective therapy in children with a growing number of long-term survivors. Risk factors for mortality in patients ≤ 10 years of age at transplant with conditional survival to 3 years post-transplant include CAV, rejection, malignancy, female sex, and Black race.
-
Pediatric Age-Prioritized Waitlisting Policy Potentially Disadvantages Adolescents on Dialysis Not Listed for Transplant Until Adulthoodno
Graphical Abstract
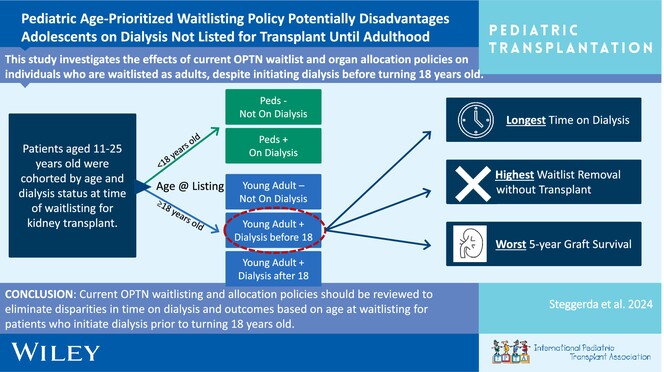
Young adults who initiate dialysis before 18 years old are disadvantaged by current OPTN waitlist and organ allocation policies for kidney transplantation. Compared to adolescents and other young adults, these patients spend the longest time on dialysis, have the highest incidence of waitlist removal without transplant, and have the worst graft survival after kidney transplantation.
-
Tracheostomy as a Management Option After Listing for Pediatric Cardiac Transplantationoa
Graphical Abstract
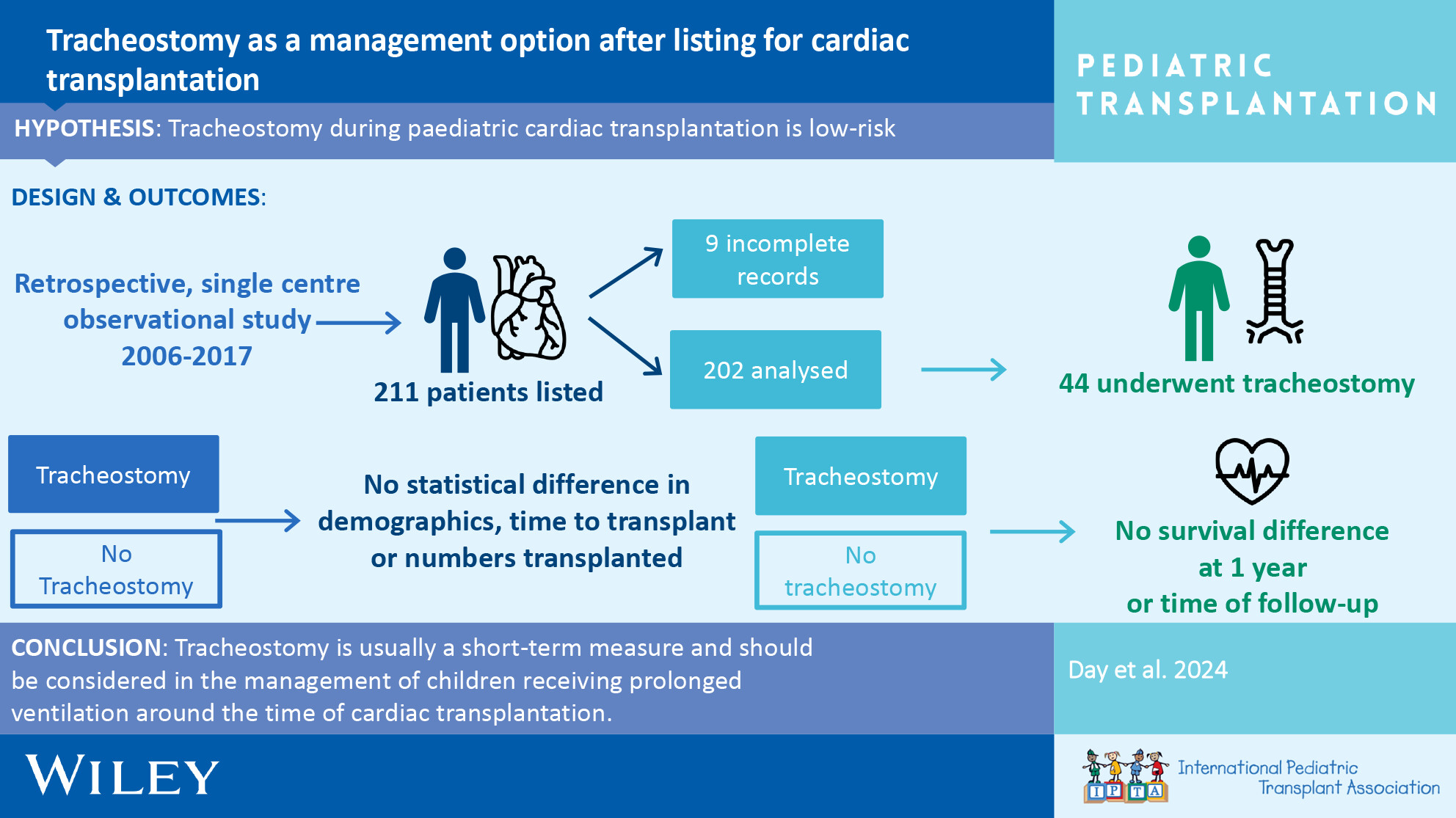
Tracheostomy after listing for pediatric cardiac transplantation is a safe adjunct to assist progress. We show minimal side effects and no difference in survival between those with tracheostomy and those without over the full follow-up period.
-
Living Donor Liver Transplantation for Young Biliary Atresia Recipients Is Associated With Improved Outcomes in the Modern Erano
Graphical Abstract
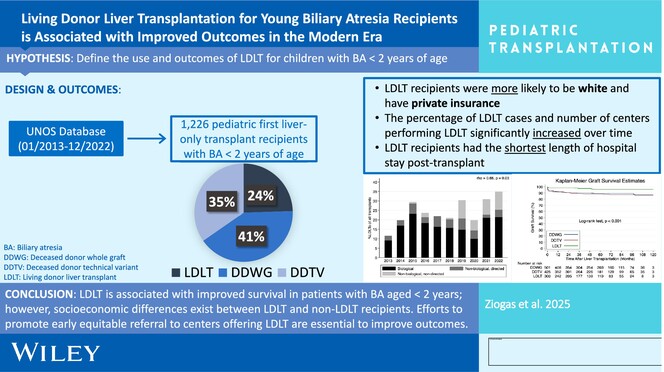
Living donor liver transplantation (LDLT) is associated with improved survival in patients with biliary atresia aged < 2 years; however, socioeconomic differences exist between LDLT and non-LDLT recipients. Efforts to promote early equitable referral to centers offering LDLT are essential for improving outcomes in young children with biliary atresia.