All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Pneumocystis jiroveci Pneumonia Infections in Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
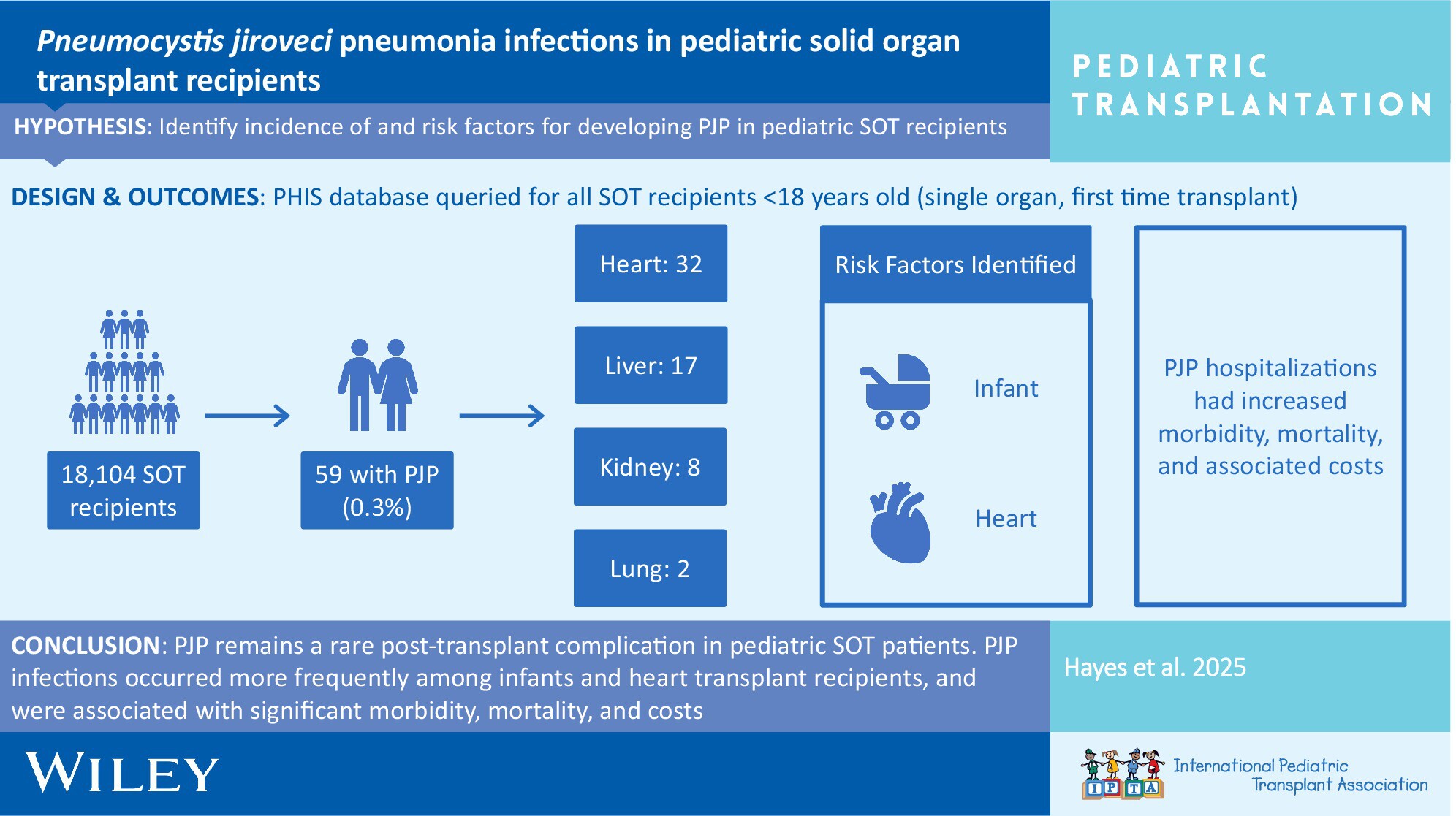
In the current era, PJP remains a rare post-transplant complication in pediatric SOT patients. PJP infections are associated with significant morbidity, mortality, and costs. Risk factors for PJP are young age at transplant and heart transplantation. An assessment of individual risk factors should be regularly performed to optimize prevention strategies.
-
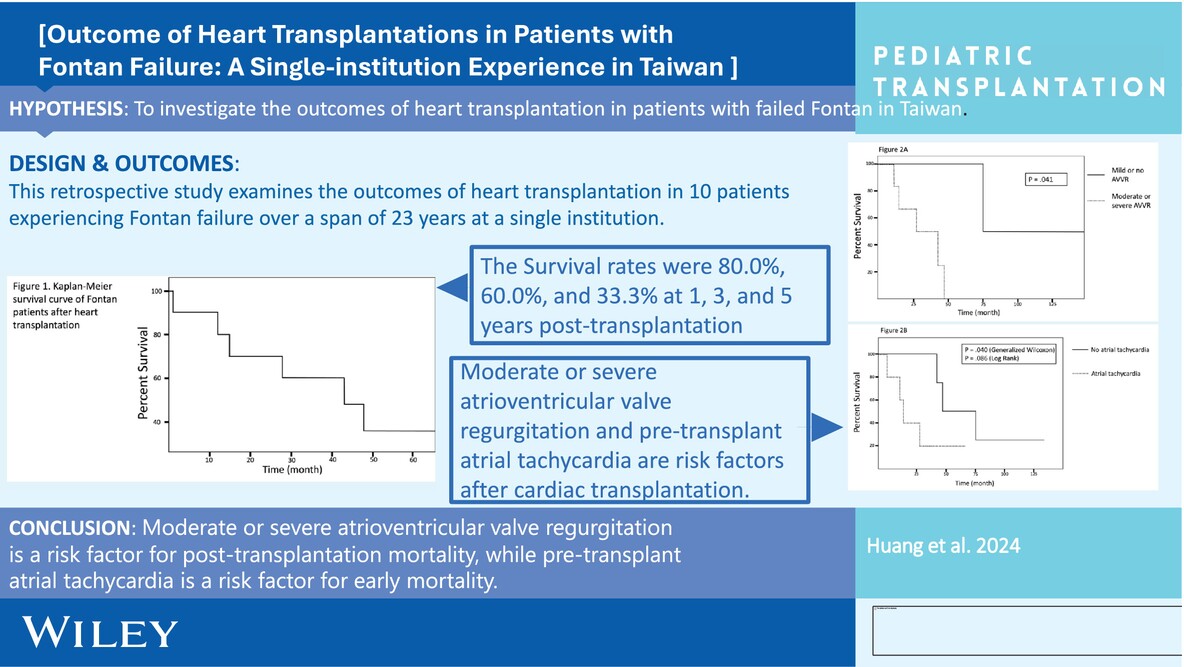
Postoperative Dialysis in Fontan Patients Undergoing Heart Transplant: How Predictive is the Pretransplant Serum Creatinine?no
Graphical Abstract
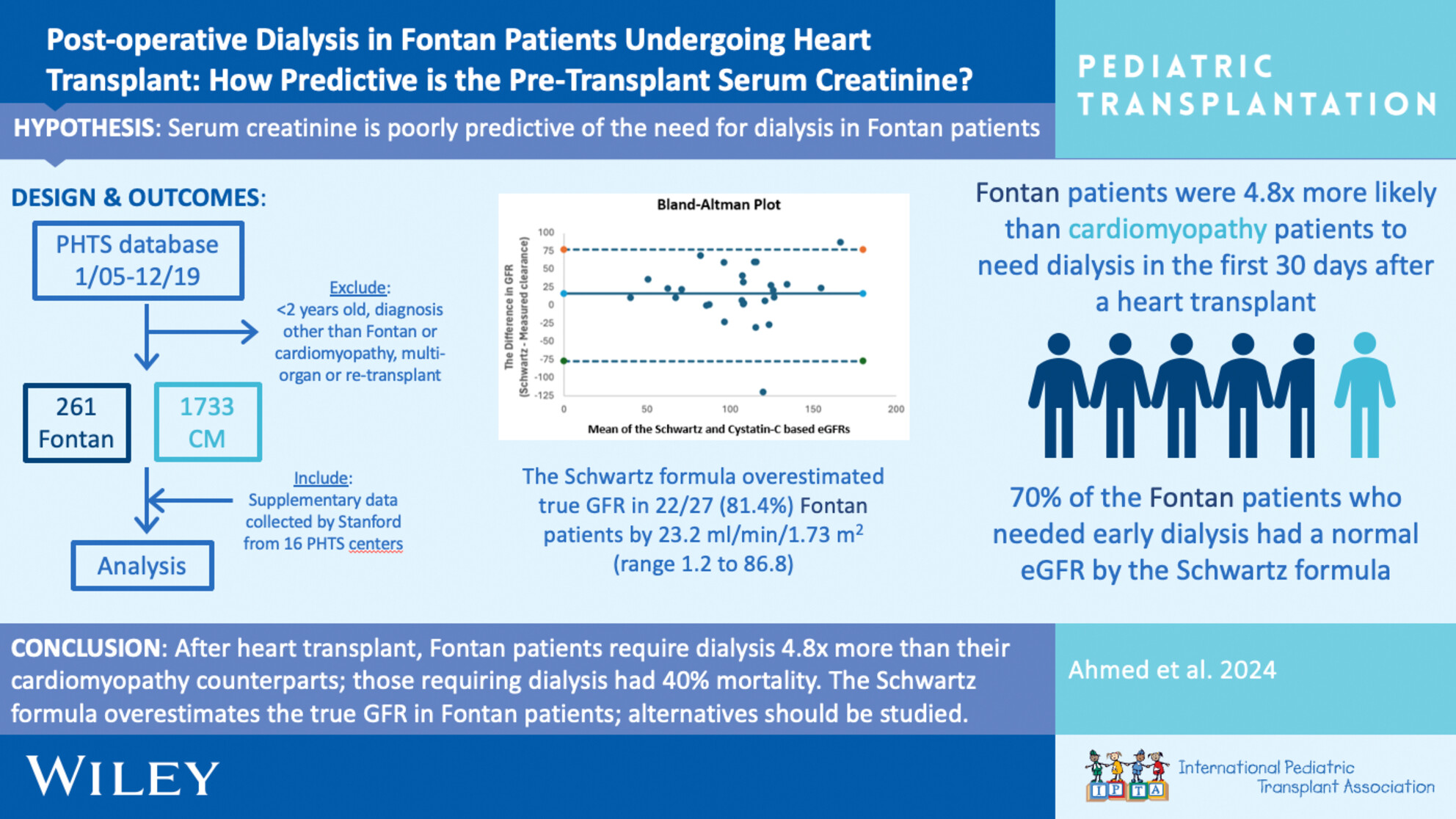
The Pediatric Heart Transplant Society database was used to identify all children ≥ 2 years old with failing Fontan or cardiomyopathy who underwent isolated heart transplant 2005–2019. The primary endpoint was postoperative dialysis within the first 30 days. Fontan patients have a ~fivefold higher risk of dialysis compared to cardiomyopathy patients.
-
Machine Learning for Predicting Waitlist Mortality in Pediatric Heart Transplantationoa
Graphical Abstract

Machine learning identified key predictors of pediatric heart transplant waitlist mortality, including candidate-specific factors (e.g., diagnosis, ventilator use) and institutional practices (e.g., organ refusal rates). Centers with high refusal rates had worse outcomes, highlighting the need to standardize organ acceptance criteria and address modifiable risk factors to improve survival.
-
Ten-Year Pediatric Heart Transplantation: Insights and Outcomes From a Leading Center in Iranno
Graphical Abstract

This study analyzed 225 pediatric heart transplants performed over a decade in Iran. The 1-year, 3-year, and 5-year survival rates were 85.7%, 79.7%, and 73.9%, respectively. Key mortality risk factors included donor age (HR: 1.04, p=0.03), male donor gender (HR: 2.04, p=0.05), and rituximab treatment (HR: 2.44, p=0.05). These findings provide insights for improving pediatric heart transplant outcomes.
-
Frailty in Pediatric Liver Disease May Be Associated With an Increased Incidence of Readmissions After Pediatric Liver Transplantationno
Graphical Abstract

Pretransplant frailty in children is associated with worse post-LT outcomes. Multicenter study included patients who had frailty assessment and then underwent liver transplant. Clinical outcomes were collected up to 1 year post LT. 28 pediatric LT recipients were included, and 15 participants met criteria for frailty. Higher pre-transplant frailty scores were also significantly associated with an increased number of readmissions after transplantation (p = 0.034). Pediatric frailty is associated with increased frequency of hospitalization in the first year after pediatric liver transplantation. These data support the concept that frail children should be identified and targeted for prehabilitation prior to liver transplant.
-
Sex-Based Disparities in Heart Transplantation in Teenagersno
Graphical Abstract

Female teenagers have lower survival following heart transplantation than their male counterparts. Male donor—female recipient transplants have the lowest survival among sex-matching groups. The use of organs from oversized or younger donors may be considered to help improve post-transplant survival in teenagers.
-
Pre-Transplant Immunophenotyping in Pediatric Heart Transplant: A Role for the Immunologist?oa
Graphical Abstract
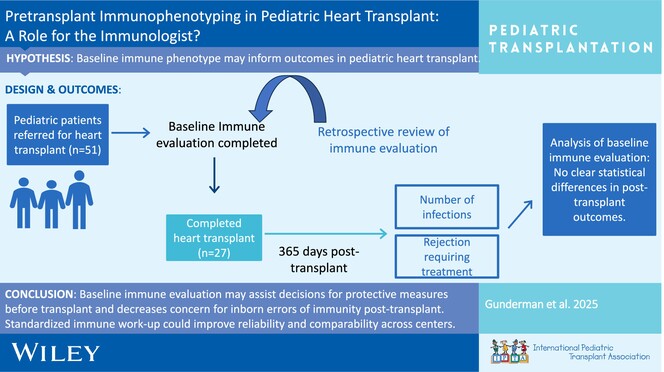
Baseline immune evaluation can assist in decisions for additional protective measures before transplant (avoidance of live vaccines, antimicrobial prophylaxis) and decrease the uncertainties in the evaluation of inborn errors of immunity after transplant. Ongoing work and developing standardized protocols for baseline immunologic work-up could improve reliability and comparability across different centers.
-
Impact of Pharmacogenomic Testing in Pediatric Heart and Kidney Transplantno
Graphical Abstract
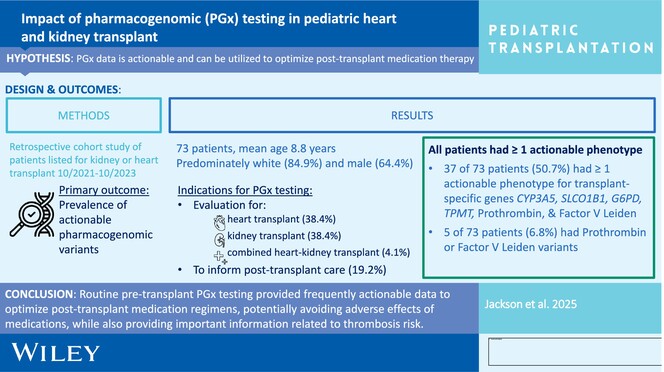
Routine pretransplant PGx testing provides frequently actionable data to optimize posttransplant medication regimens, potentially avoiding adverse effects of medications including tacrolimus, azathioprine, HMG-CoA reductase inhibitors, and dapsone, while also providing important information related to thrombosis risk for VTE prophylaxis.
-
Long-Term Survival in Children Following Heart Transplantationno
Graphical Abstract
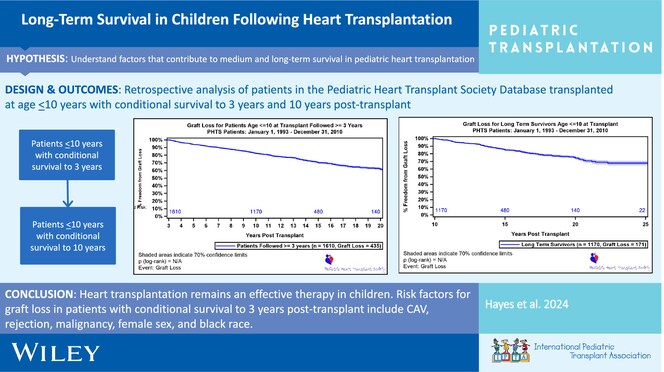
Heart transplantation remains an effective therapy in children with a growing number of long-term survivors. Risk factors for mortality in patients ≤ 10 years of age at transplant with conditional survival to 3 years post-transplant include CAV, rejection, malignancy, female sex, and Black race.
-
Tracheostomy as a Management Option After Listing for Pediatric Cardiac Transplantationoa
Graphical Abstract
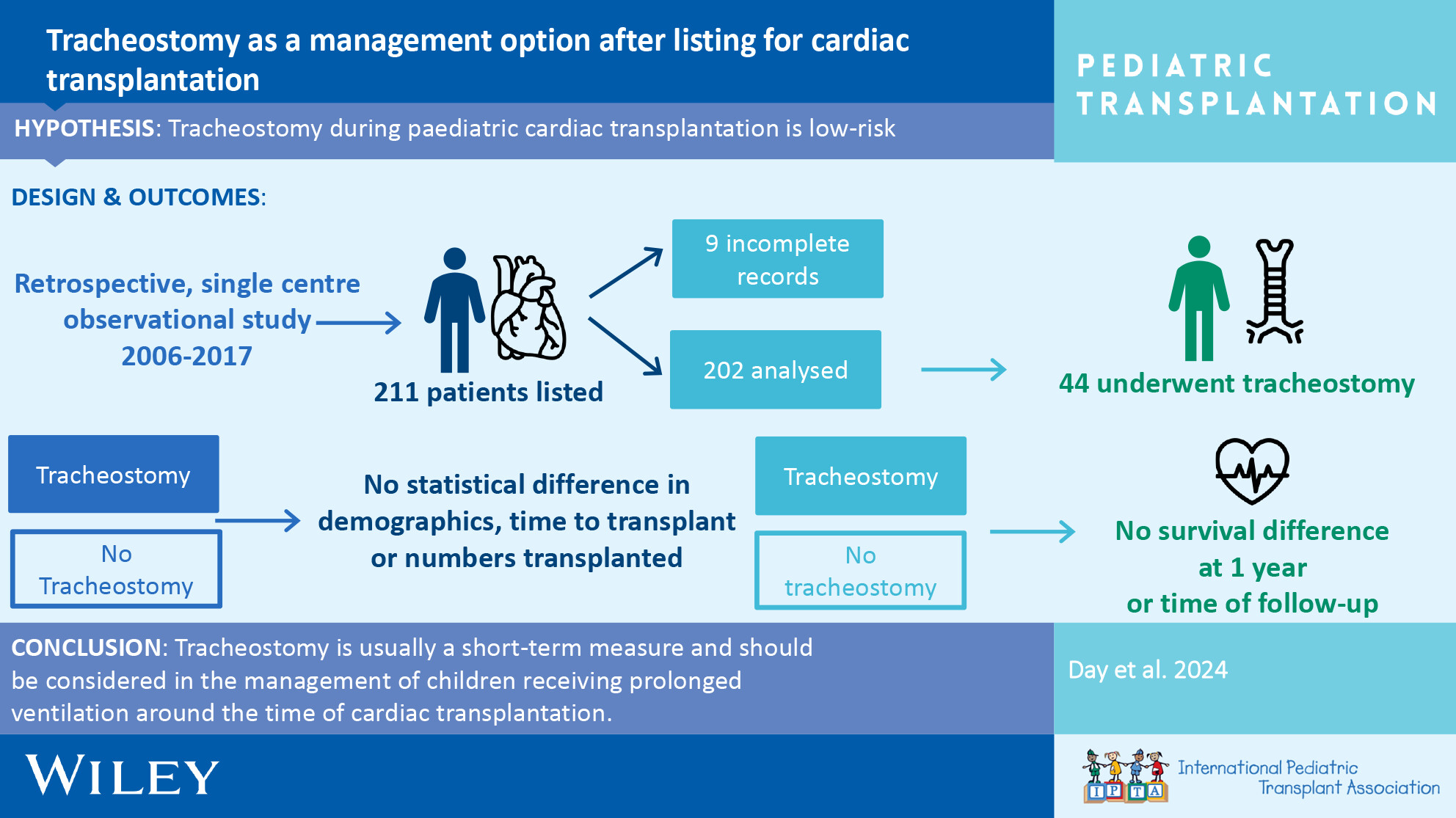
Tracheostomy after listing for pediatric cardiac transplantation is a safe adjunct to assist progress. We show minimal side effects and no difference in survival between those with tracheostomy and those without over the full follow-up period.
-
It's Getting Better All the Time: Decreased Cumulative Incidence of Waitlist Mortality in Pediatric Candidates Following 2018 Heart Allocation Policy Changeno
Graphical Abstract
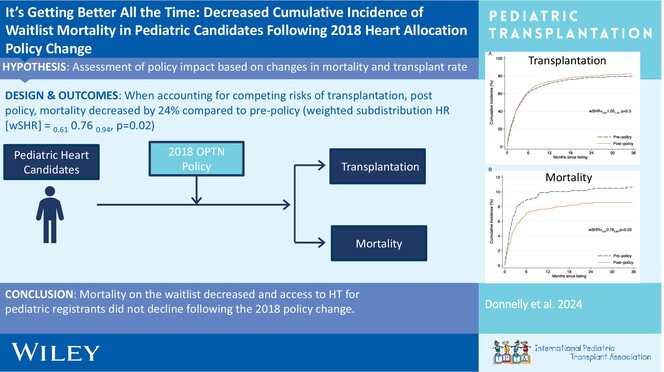
In October 2018, the OPTN changed adult heart transplant (HT) allocation policy, increasing the number of adult candidates that had higher priority than pediatric candidates, potentially disadvantaging pediatric waitlist registrants. Mortality on the waitlist decreased and access to HT for pediatric registrants did not decline following the policy change.
-
Change in Allocation Pattern of Pediatric Deceased Donor Kidneys Following the Implementation of a New Allocation Policy With Pediatric Priority in Koreano
Graphical Abstract
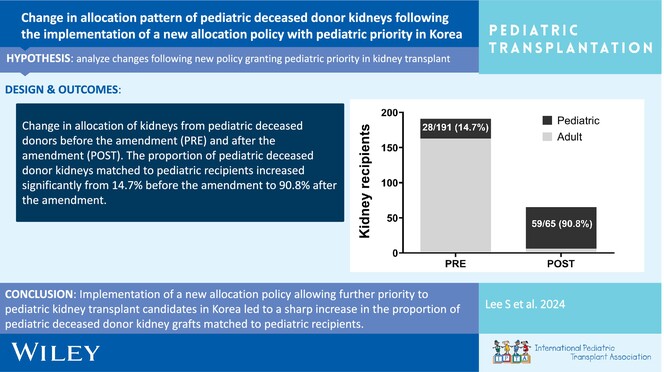
Change in allocation of kidneys from pediatric deceased donors before the amendment (PRE) and after the amendment (POST). The proportion of pediatric deceased donor kidneys matched to pediatric recipients increased significantly from 14.7% before the amendment to 90.8% after the amendment.
-
Deficits in Pre- and Post-transplant Functional, Motor, and Cognitive Deficits Associated With Graft Failure and Mortality in Pediatric Heart Transplant Recipientsno
Graphical Abstract
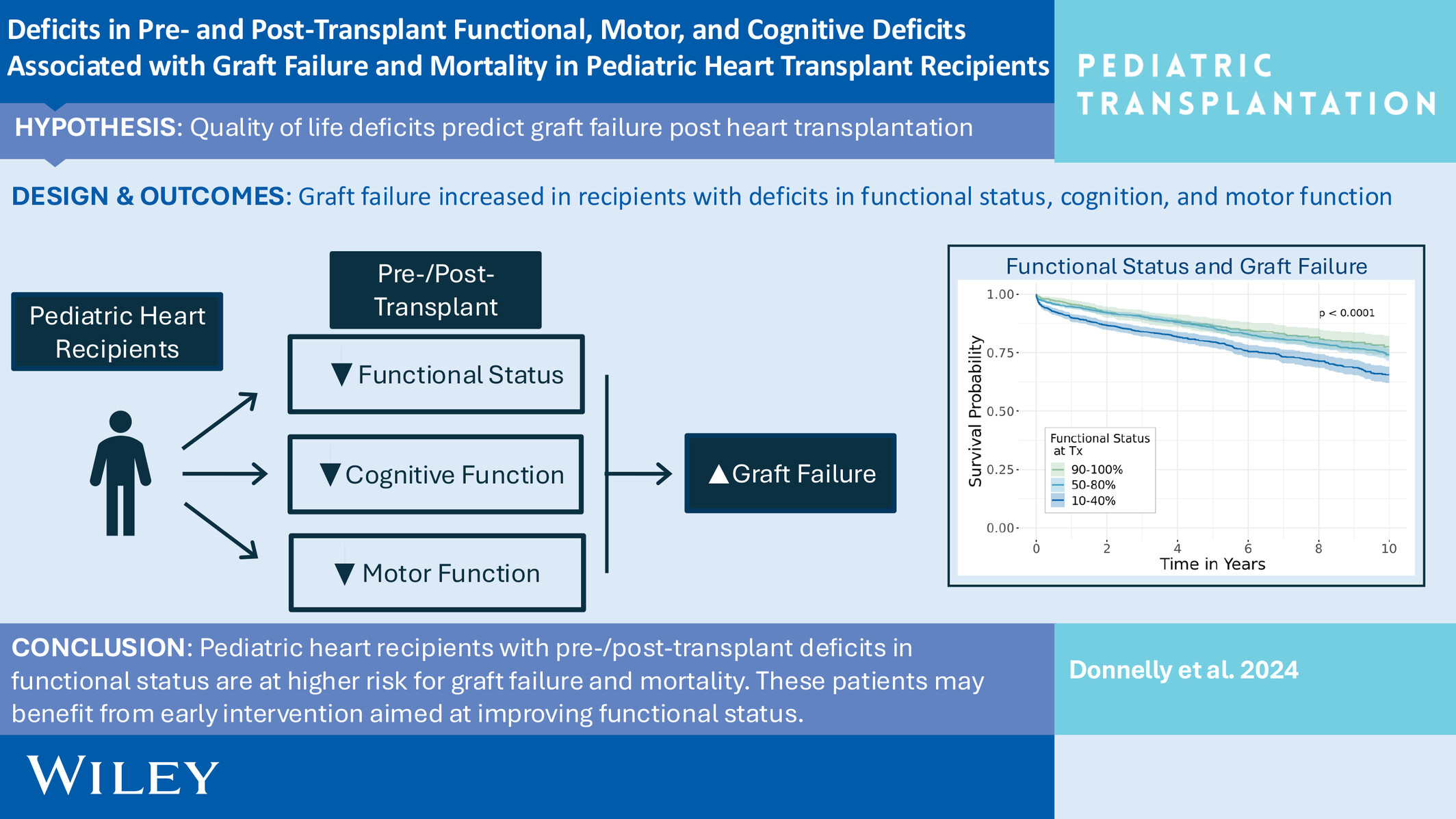
Pediatric HT recipients with decreased pre- and post-transplant functional status are at higher risk for graft failure and mortality. These patients may benefit from early intervention aimed at improving functional status.
-
Decreasing Endomyocardial Biopsy Frequency in Pediatric Heart Transplantation Using A Rejection Risk Prediction Score—A Single Center Studyoa
Graphical Abstract
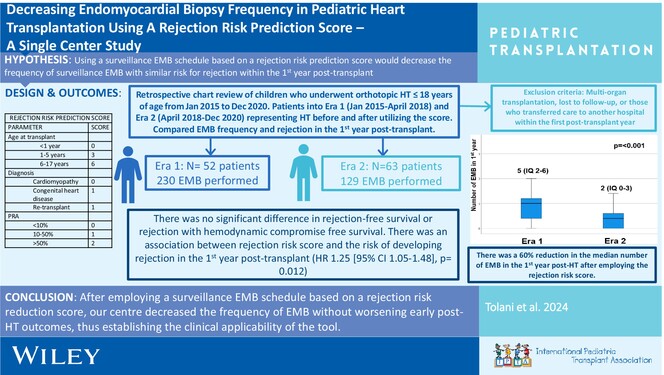
We retrospectively reviewed 115 pediatric HT recipients to evaluate the clinical applicability of the rejection risk score described by Butts et al. by comparing early rejection episodes of pediatric HT recipients and the number of EMB performed at our center before and after use of the score. With utilization of the score, our center decreased the frequency of EMB by 60% in the first-year post-transplant without worsening early post-transplant outcomes.