All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
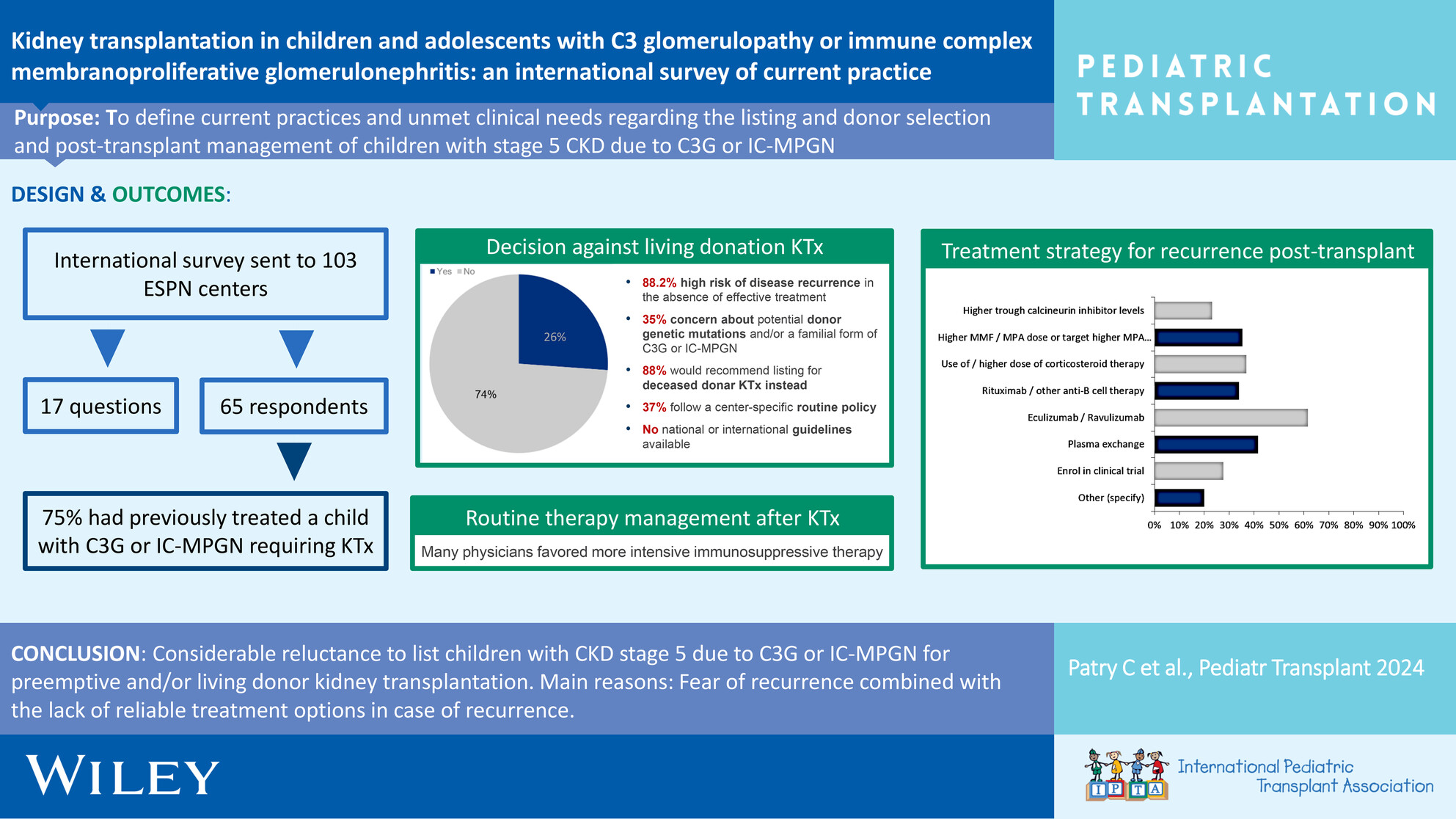
Oral Health Status of Children With a History of Liver Transplantationoa
Graphical Abstract
This study examines the oral health of children who have undergone liver transplantation, highlighting dental development delays despite similar caries rates compared to their healthy peers. Findings emphasize the need for integrated dental-medical care, focusing on dental age assessment and early intervention to optimize oral health outcomes in this vulnerable population.
-
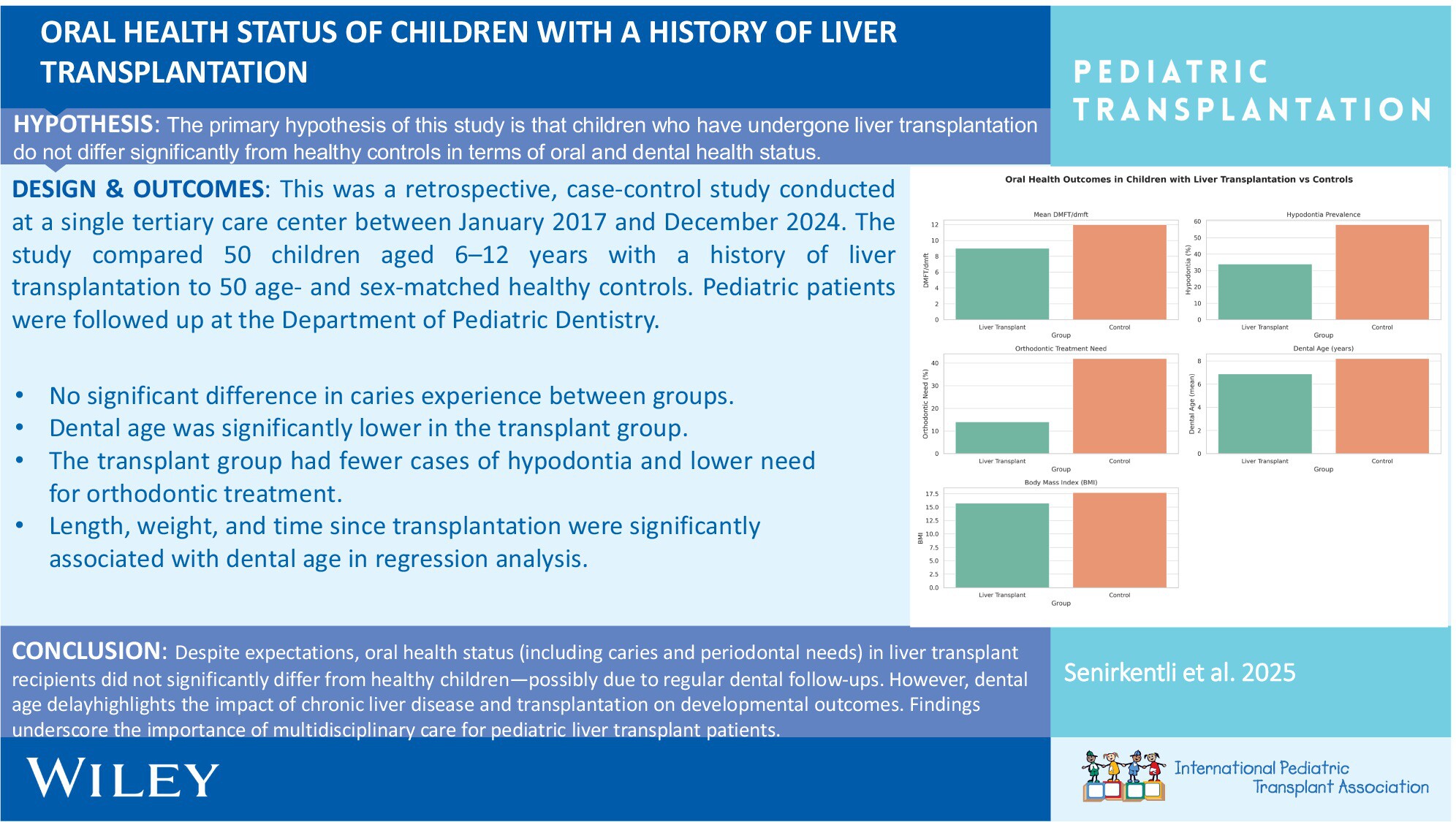
Liver Transplantation in Primary Hyperoxaluria: A Single-Center 10-Year Experienceno
Graphical Abstract
Liver transplantation (LT) significantly improves survival and quality of life for children with primary hyperoxaluria (PH), with favorable long-term outcomes observed in most patients. Despite reductions in urine oxalate levels, challenges such as graft shortages and renal graft loss persist, underscoring the need for ongoing monitoring and care.
-
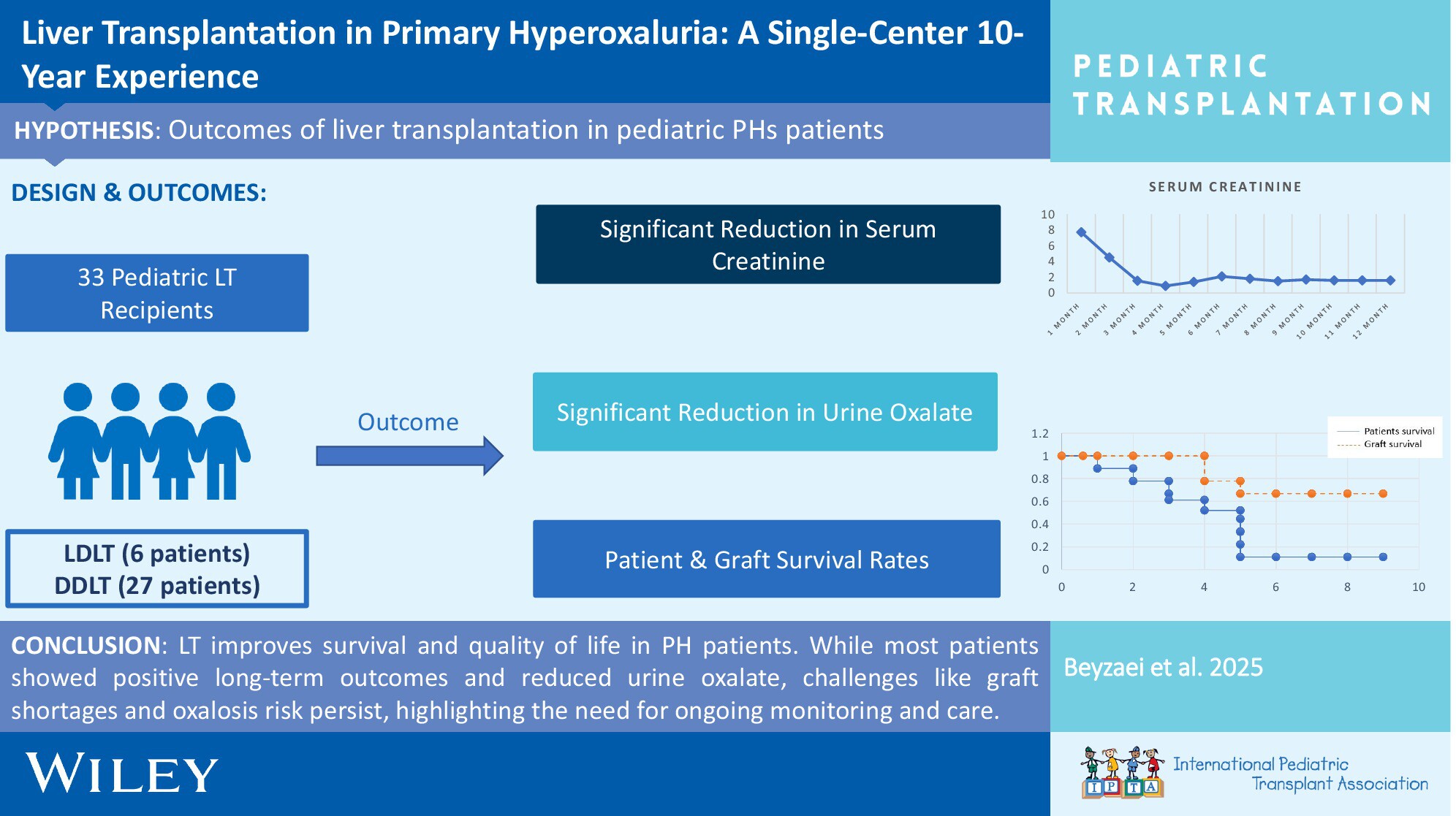
Educational Gaps and Suggestions for Change for Pediatric Transplant Fellowship Training Based on Fellow Survey Responsesno
Graphical Abstract
Significant gaps exist in pediatric transplant fellowship training, including immunosuppression management and long-term care. Our study identifies these areas through a global survey of 237 fellows and proposes actionable strategies, such as case-based learning and interdisciplinary collaboration, to enhance training and improve patient outcomes.
-
Cidofovir Treatment for Prevention of BK Virus-Associated Hemorrhagic Cystitis in Pediatric Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantationno
Graphical Abstract
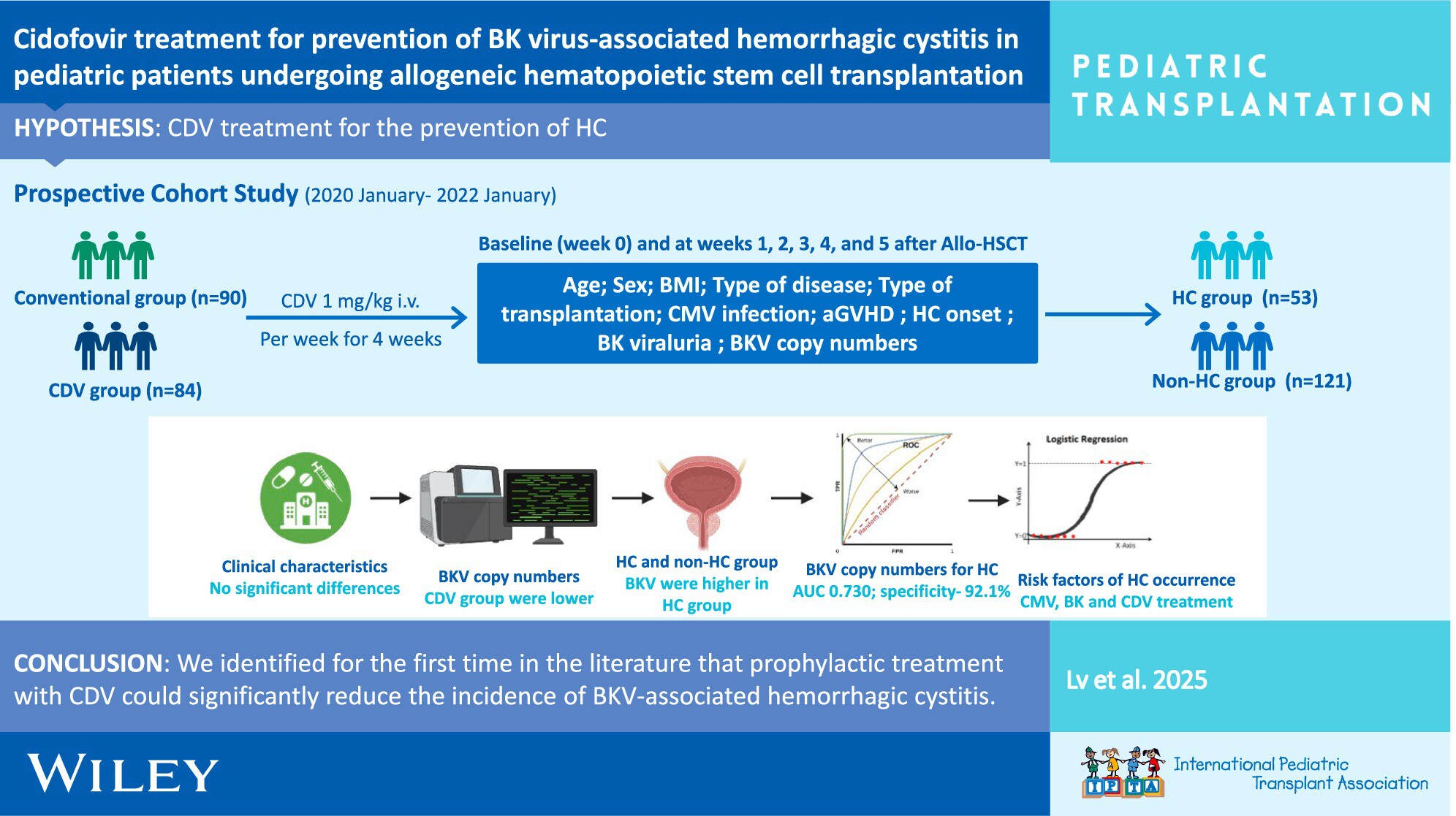
Cidofovir (CDV) prophylaxis significantly reduces the incidence of BK virus-associated hemorrhagic cystitis in pediatric patients undergoing allogeneic hematopoietic stem cell transplantation. Early BKV copy number reduction and lower graft-versus-host disease prevalence in the CDV group suggest its potential as an effective preventive treatment.
-
From Referral to Consent: Unveiling Racial Disparities at Critical Stages of Pediatric Organ Donationno
Graphical Abstract
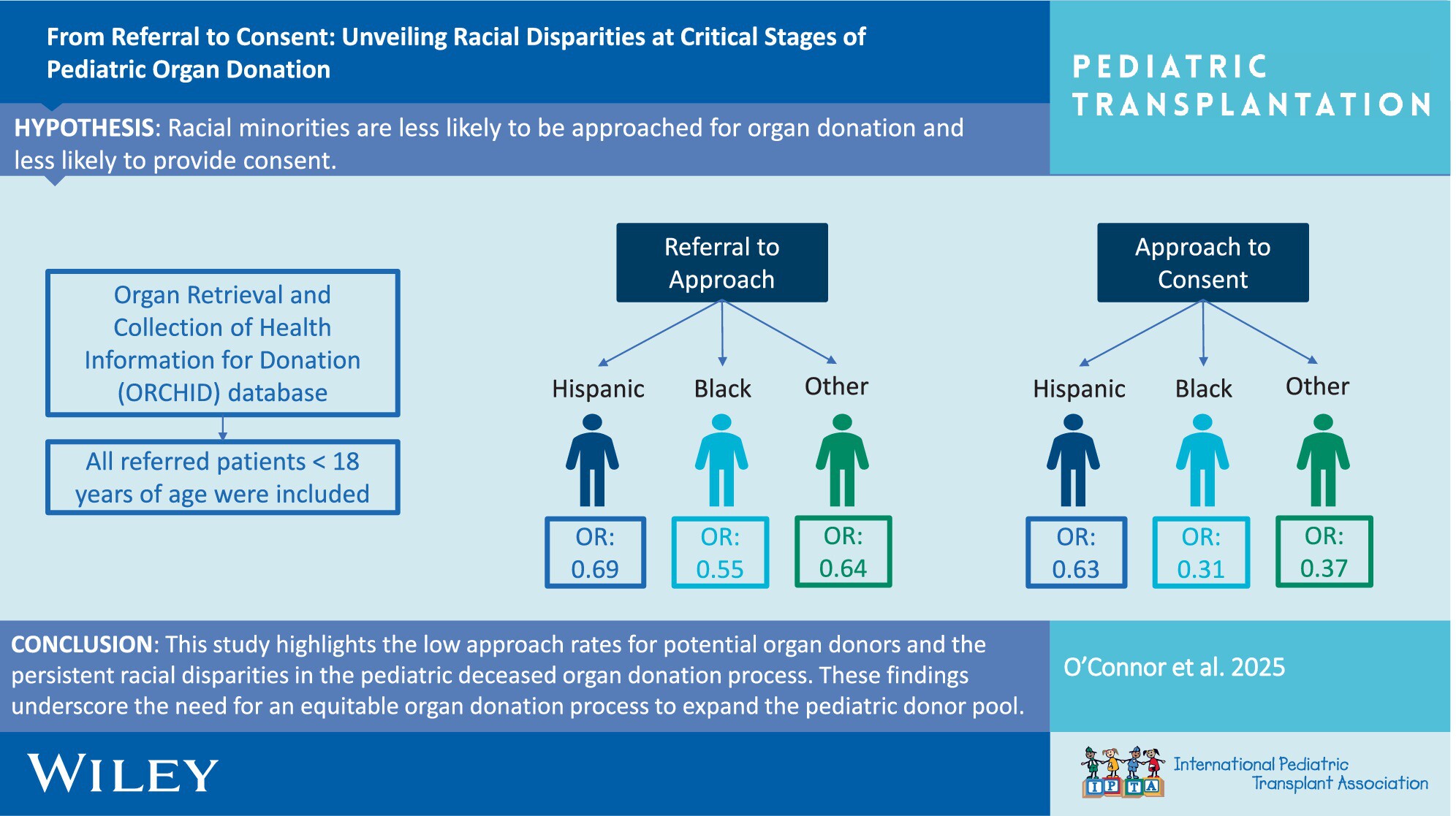
This study highlights the low approach rates for potential organ donors and the persistent racial disparities in the pediatric deceased organ donation process. Racial minority groups are less likely to be approached for donation and consent compared to Whites. These findings underscore the need for an equitable organ donation process to expand the pediatric donor pool.
-
Frailty in Pediatric Liver Disease May Be Associated With an Increased Incidence of Readmissions After Pediatric Liver Transplantationno
Graphical Abstract

Pretransplant frailty in children is associated with worse post-LT outcomes. Multicenter study included patients who had frailty assessment and then underwent liver transplant. Clinical outcomes were collected up to 1 year post LT. 28 pediatric LT recipients were included, and 15 participants met criteria for frailty. Higher pre-transplant frailty scores were also significantly associated with an increased number of readmissions after transplantation (p = 0.034). Pediatric frailty is associated with increased frequency of hospitalization in the first year after pediatric liver transplantation. These data support the concept that frail children should be identified and targeted for prehabilitation prior to liver transplant.
-
An Unheard Voice: The Perspectives of Siblings of Solid Organ Transplant Recipientsno
Graphical Abstract
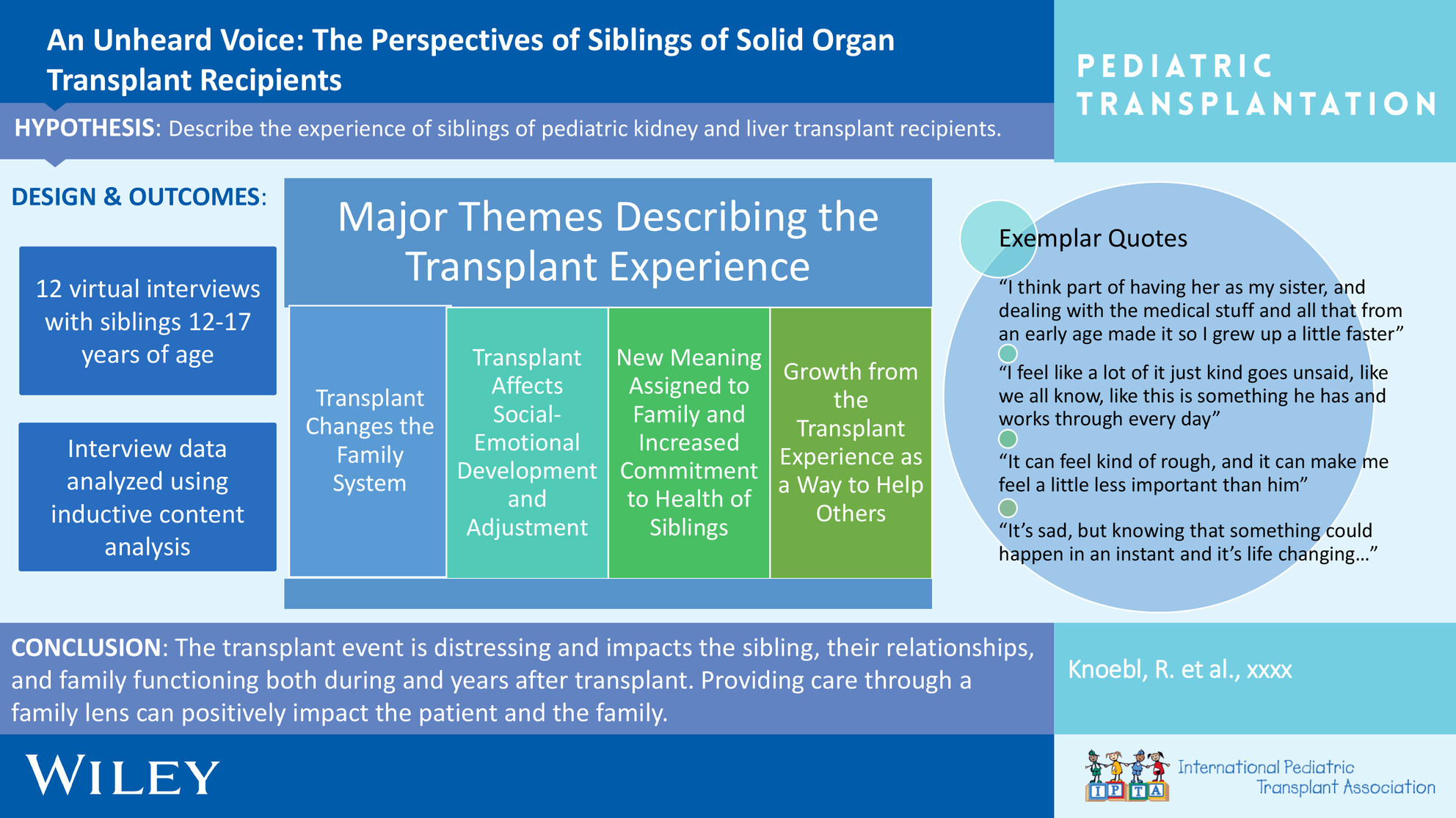
Sibling (ages 12–17 years) of kidney and liver transplant recipients affirm that the transplant event is distressing and impacts their relationships and family functioning both in the moment and for years after the transplant. Transplant team members can support siblings through healthcare interactions and a family-inclusive model of care.
-
Procedure Costs Associated With Management of Biliary Strictures in Pediatric Liver Transplant Recipients in the Society of Pediatric Liver Transplantation (SPLIT) Registryno
Graphical Abstract
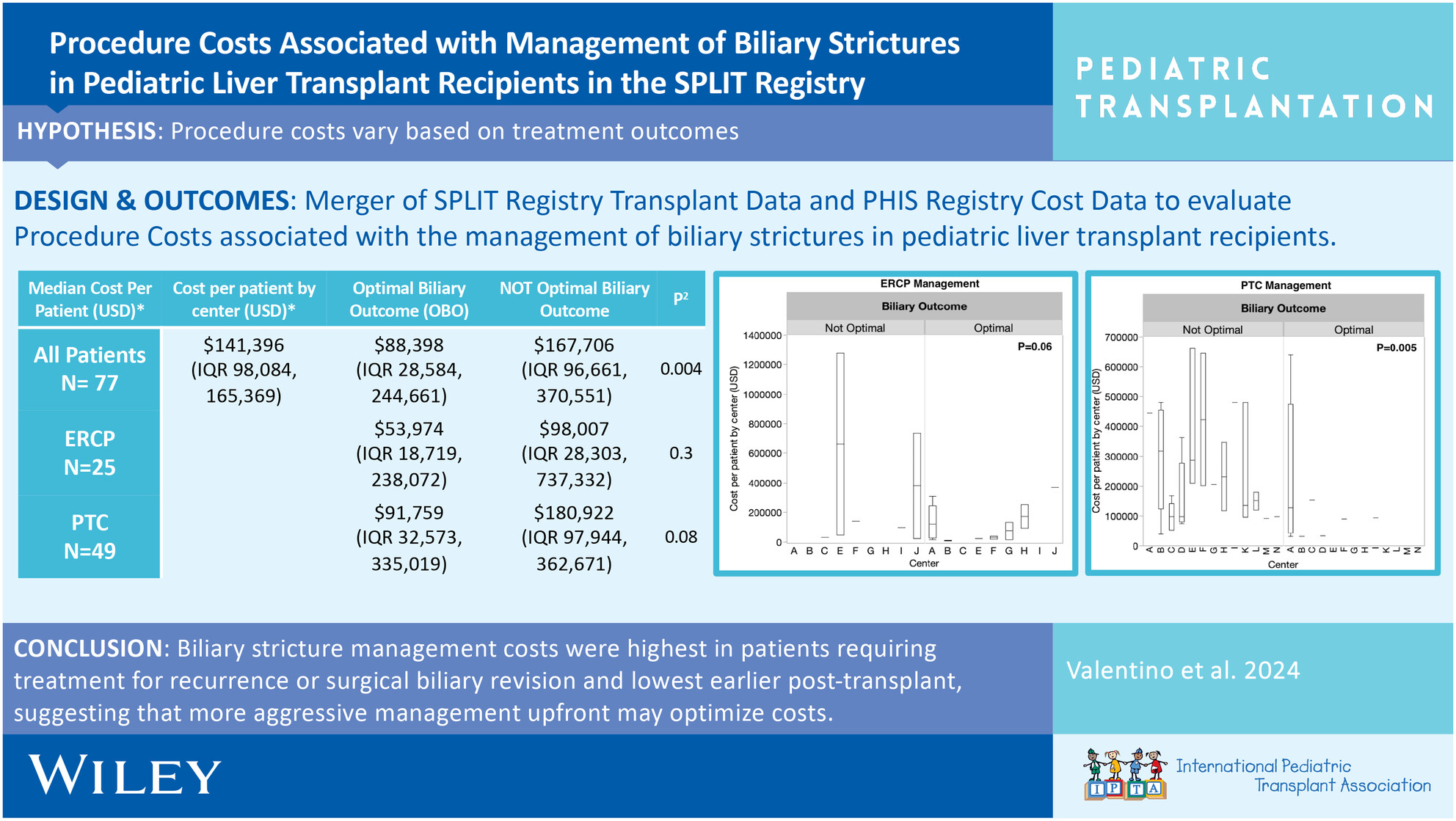
Biliary strictures management costs were highest in patients requiring treatment for recurrence or surgical biliary revision and lowest earlier post-transplant, suggesting that more aggressive management upfront may optimize costs. Future work will explore practice variation and cost-effective strategies to achieve OBO.
-
Short and Long-Term Outcomes of Liver Transplantation in Pediatric Patients With Inborn Errors of Metabolism: A Single-Center Studyno
Graphical Abstract
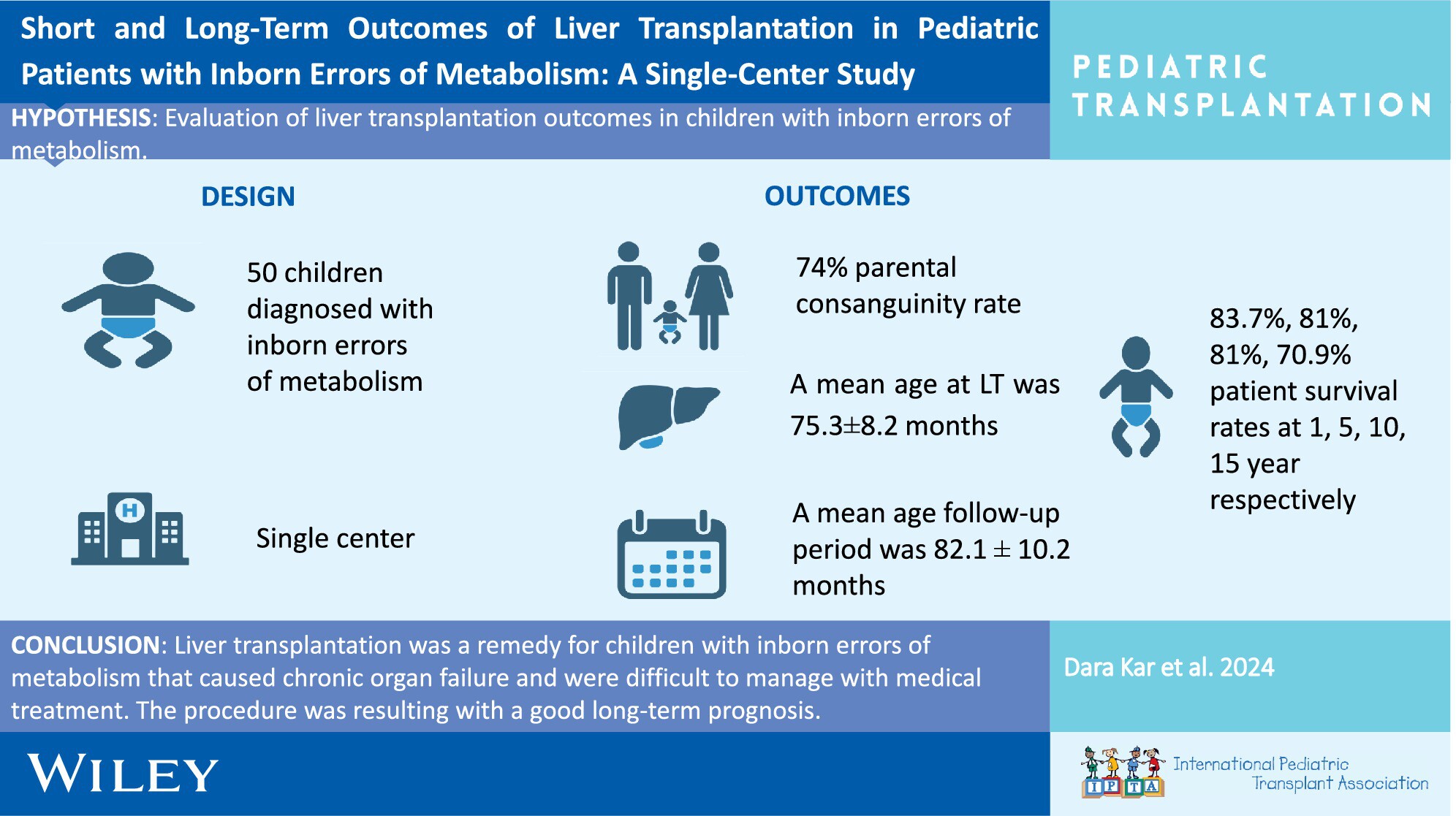
In our single-center study, we retrospectively analyzed 50 patients who underwent liver transplantation with the diagnosis of IEM. The parental consanguinity rate was 74%. The mean age at liver transplantation was 75.3 ± 8.2 months (range: 5–218), with a follow-up period of 82.1 ± 10.2 months (range:1 day–229 months). Survival rates at 1, 5, 10, and 15 years were 83.7%, 81%, 81%, and 70.9%, respectively. Liver transplantation is an effective solution for children with IEM causing chronic organ failure and difficult to manage with medical treatment, showing good long-term prognosis.
-
Impact of Pharmacogenomic Testing in Pediatric Heart and Kidney Transplantno
Graphical Abstract
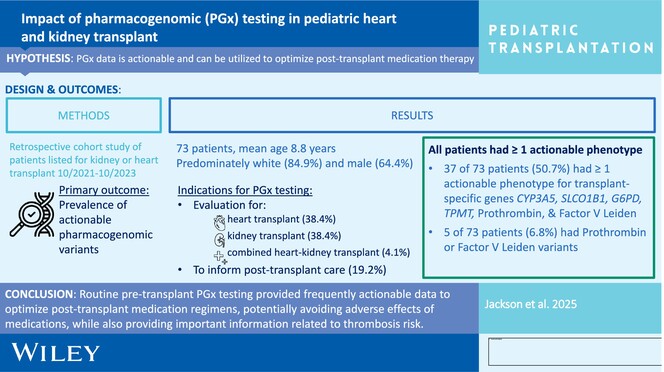
Routine pretransplant PGx testing provides frequently actionable data to optimize posttransplant medication regimens, potentially avoiding adverse effects of medications including tacrolimus, azathioprine, HMG-CoA reductase inhibitors, and dapsone, while also providing important information related to thrombosis risk for VTE prophylaxis.
-
Tracheostomy as a Management Option After Listing for Pediatric Cardiac Transplantationoa
Graphical Abstract
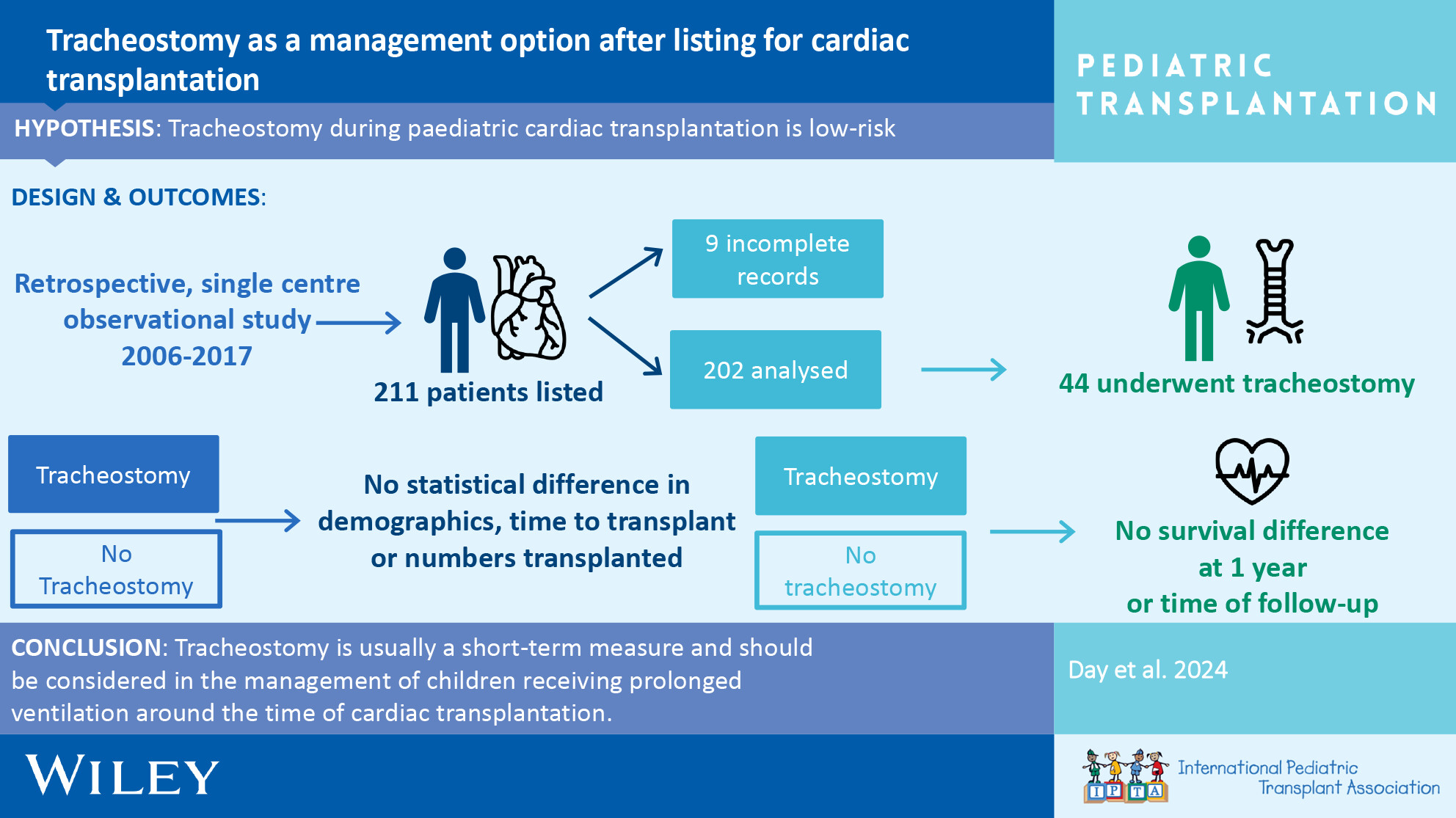
Tracheostomy after listing for pediatric cardiac transplantation is a safe adjunct to assist progress. We show minimal side effects and no difference in survival between those with tracheostomy and those without over the full follow-up period.