All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
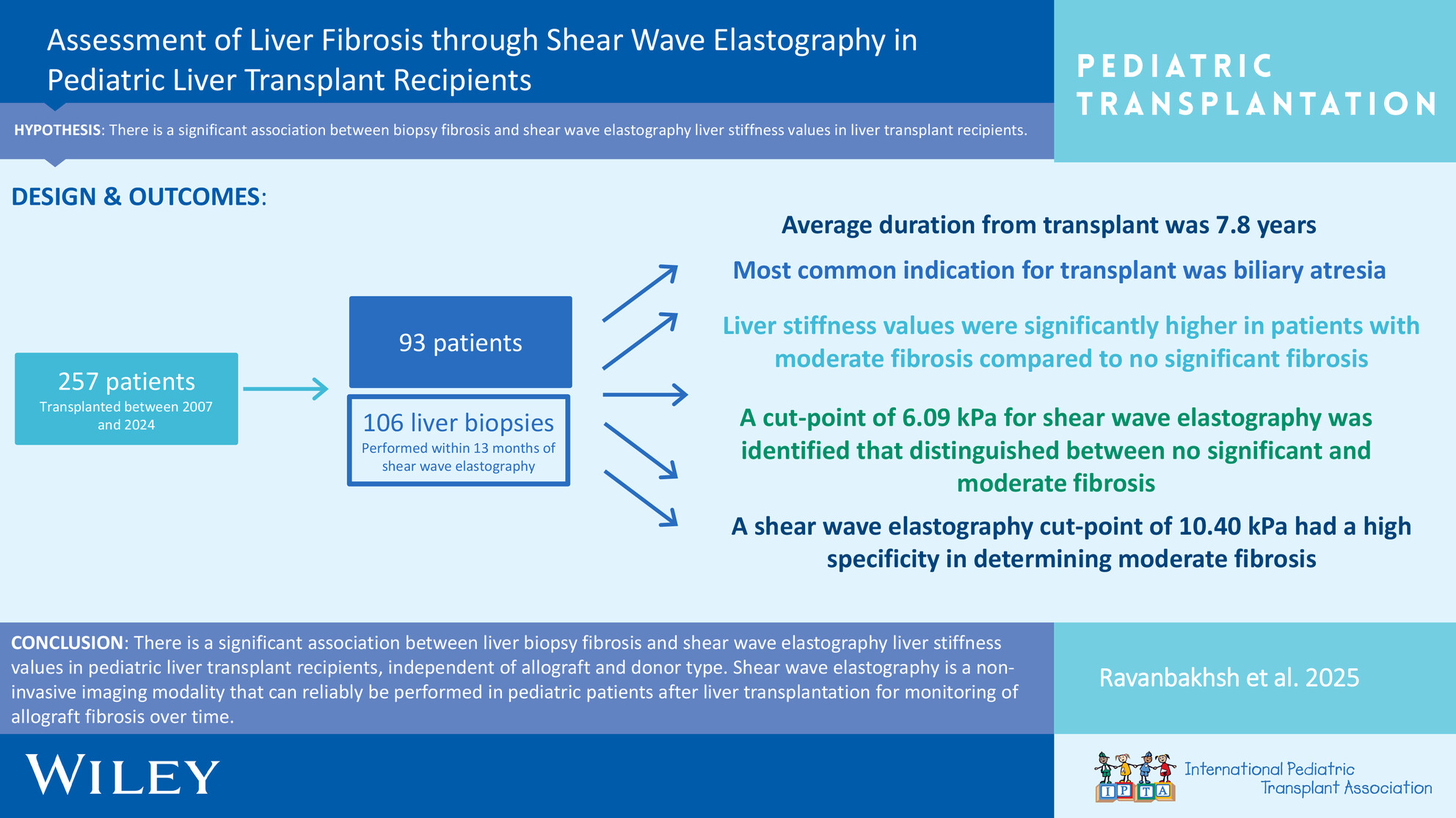
Do Cold Ischemia and Transfusion Affect Pediatric Transplant Outcomes?no
Graphical Abstract
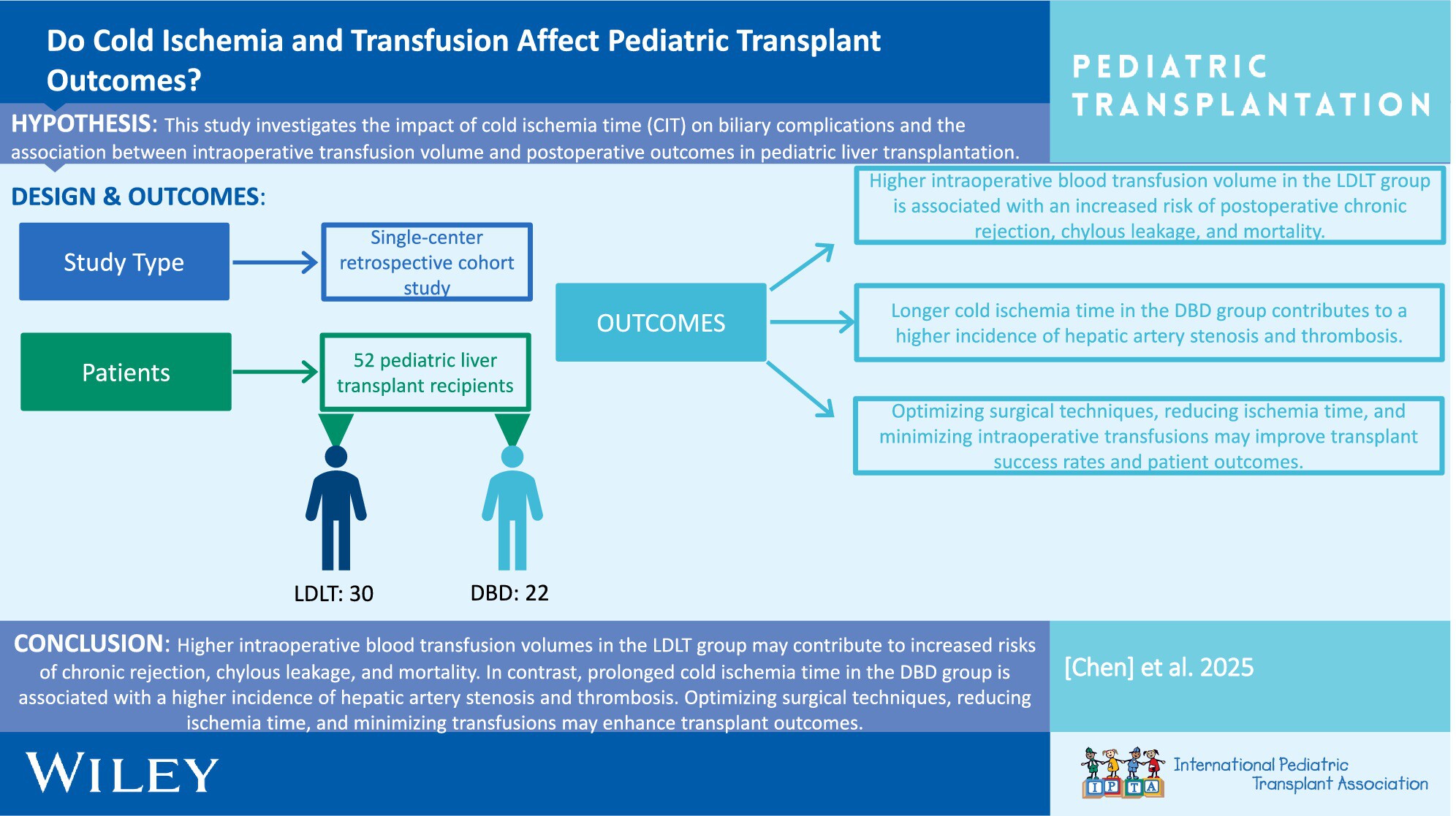
This study compares pediatric liver transplant outcomes between living donor liver transplantation (LDLT) and donation after brain death (DBD), highlighting the impact of cold ischemia time, blood transfusions, and recipient characteristics on postoperative complications and survival rates.
-
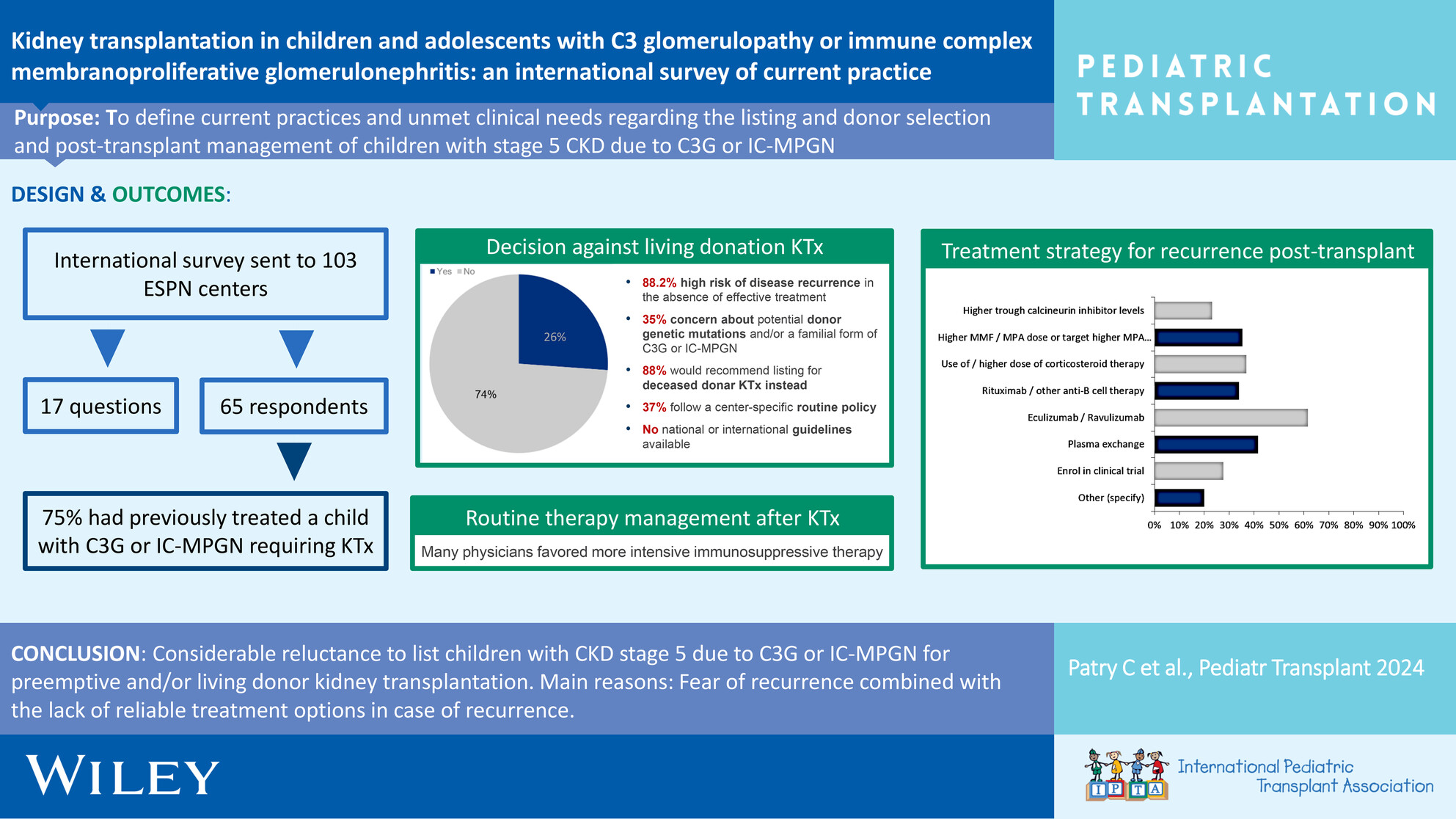
Low Absolute Lymphocyte Count Associated With Anti-Thymocyte Globulin Induction May Be a Predictor of Early Cytomegalovirus Infection in Pediatric Heart Transplantationoa
Graphical Abstract
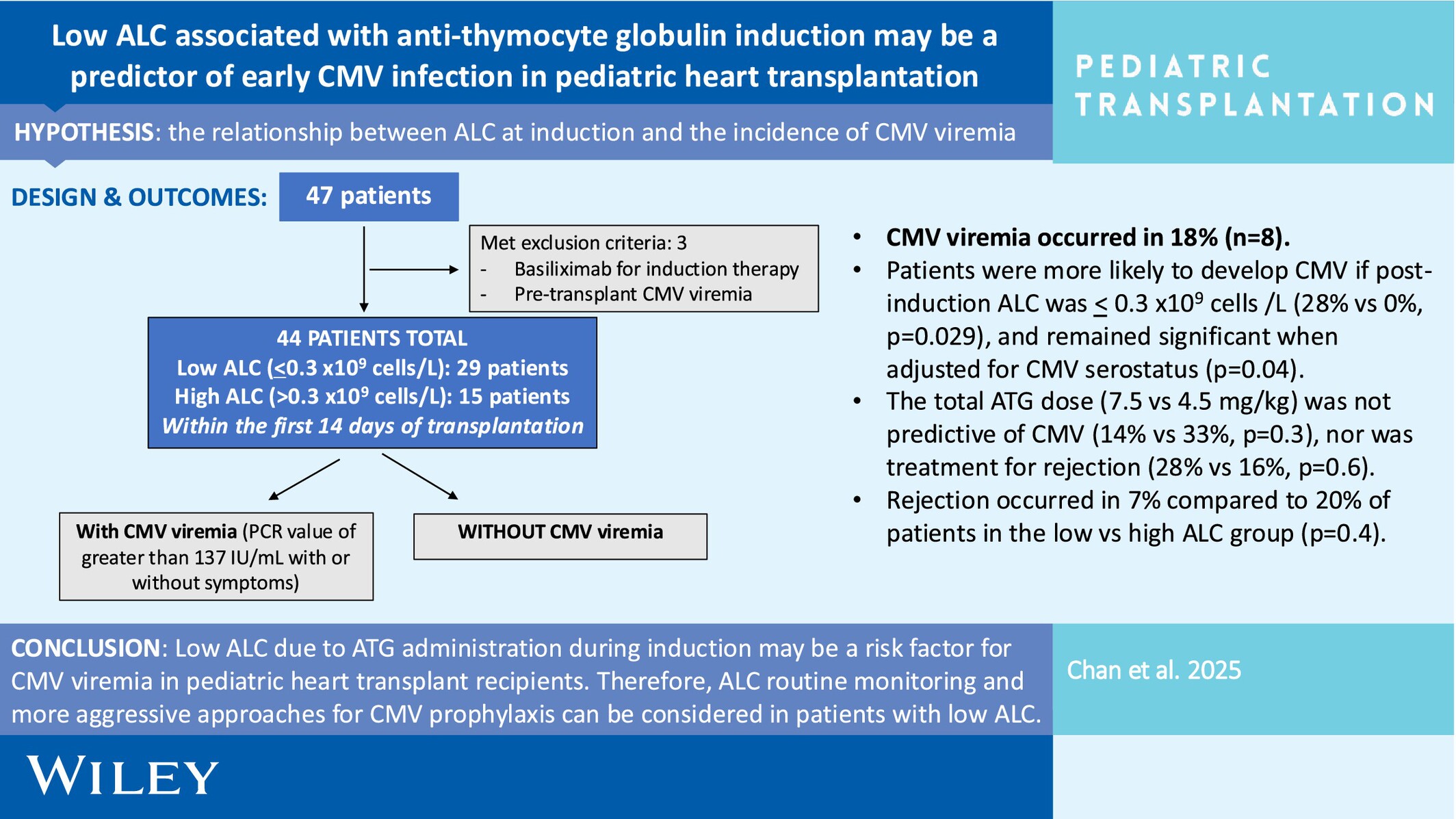
In pediatric heart transplant recipients, there is a higher incidence of cytomegalovirus if ALC ≤ 0.3 × 109 cells/L during induction, regardless of serostatus. Low ALC levels during induction may identify a high-risk group that could benefit from an altered CMV prophylactic regimen.
-
Liver Transplantation in Primary Hyperoxaluria: A Single-Center 10-Year Experienceno
Graphical Abstract
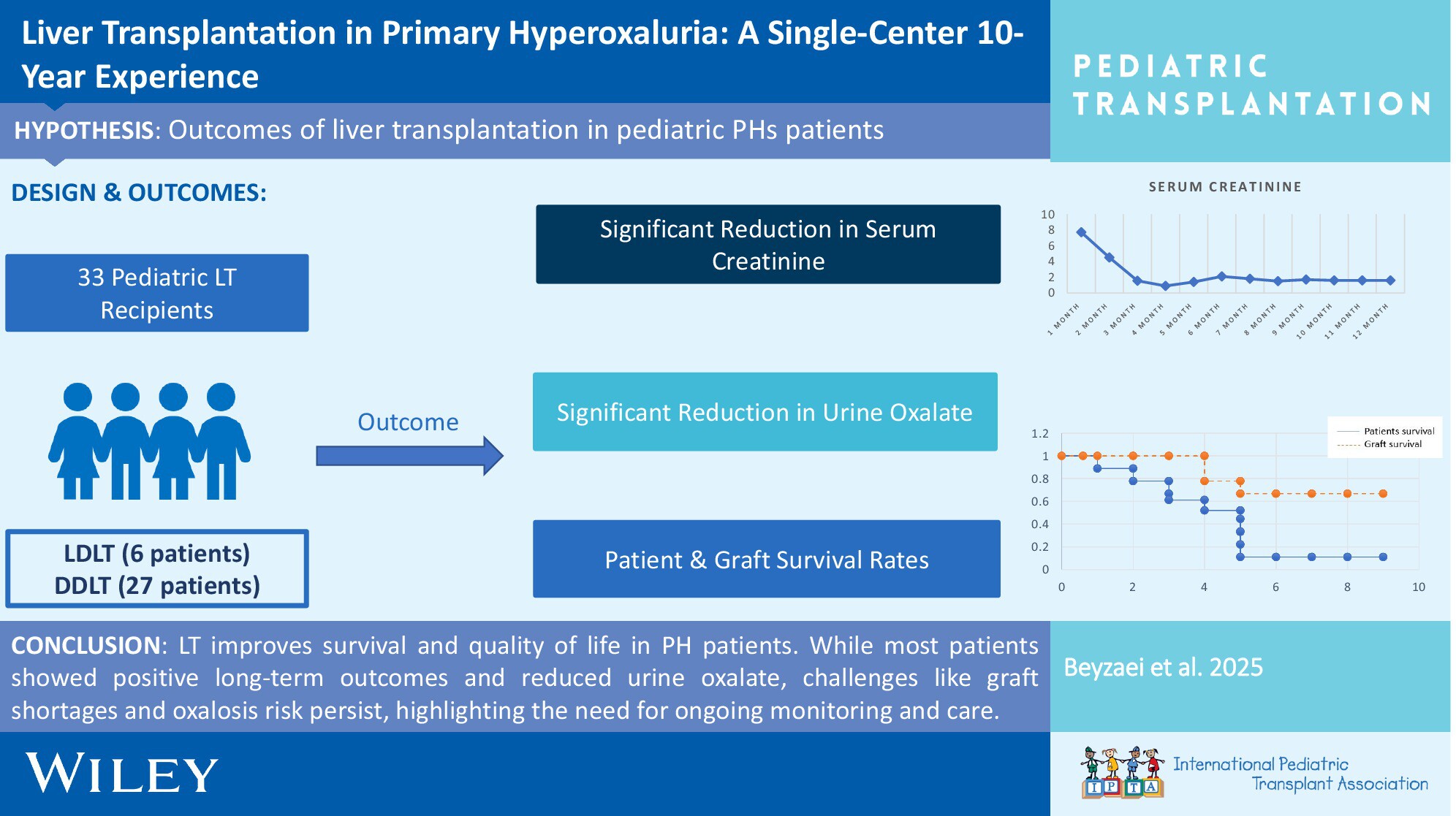
Liver transplantation (LT) significantly improves survival and quality of life for children with primary hyperoxaluria (PH), with favorable long-term outcomes observed in most patients. Despite reductions in urine oxalate levels, challenges such as graft shortages and renal graft loss persist, underscoring the need for ongoing monitoring and care.
-
Educational Gaps and Suggestions for Change for Pediatric Transplant Fellowship Training Based on Fellow Survey Responsesno
Graphical Abstract
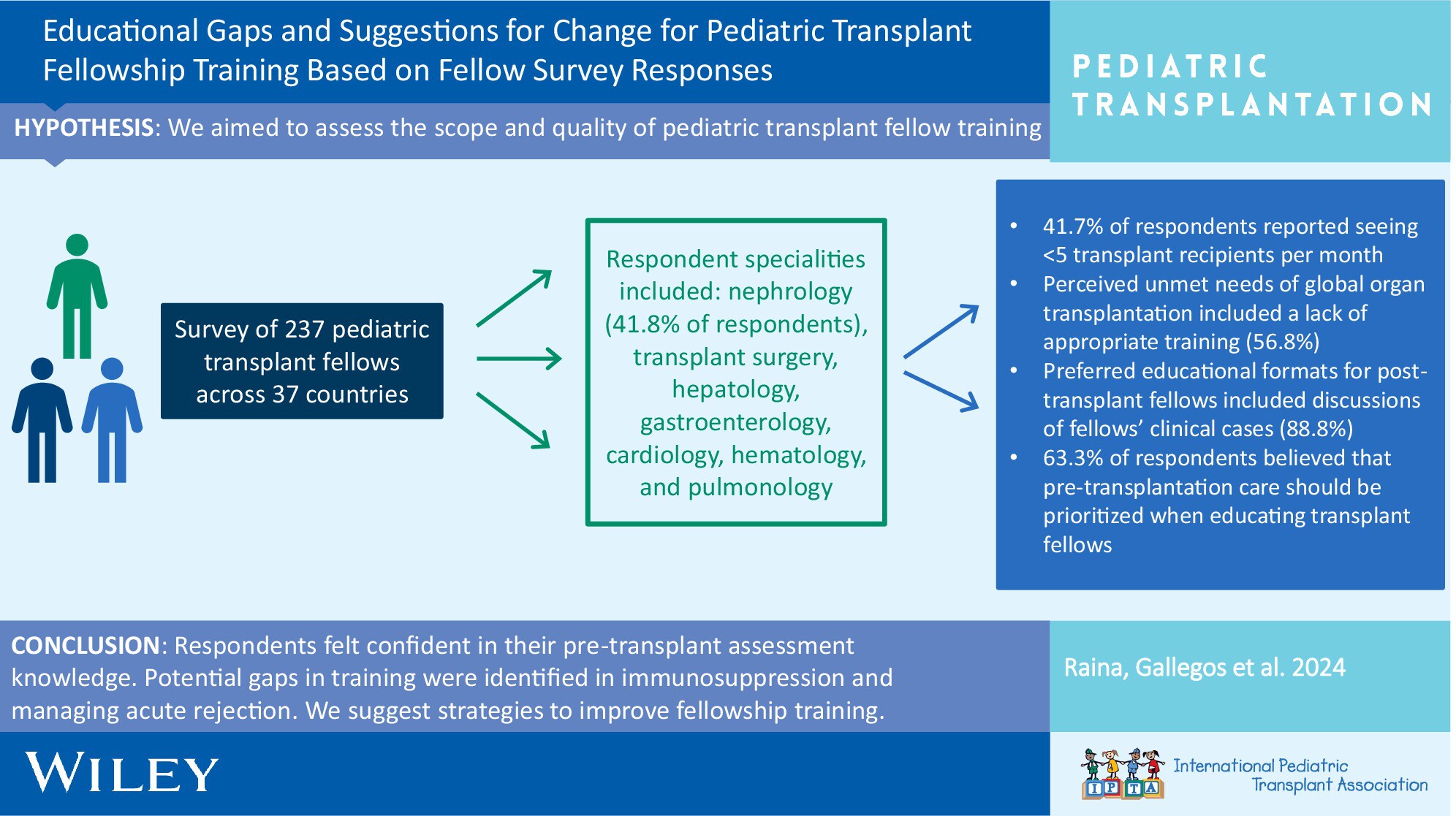
Significant gaps exist in pediatric transplant fellowship training, including immunosuppression management and long-term care. Our study identifies these areas through a global survey of 237 fellows and proposes actionable strategies, such as case-based learning and interdisciplinary collaboration, to enhance training and improve patient outcomes.
-
Combining Acute Kidney Injury Grading and Recovery Mode for Screening in Pediatric Liver Transplantation: A Retrospective Observational Studyno
Graphical Abstract
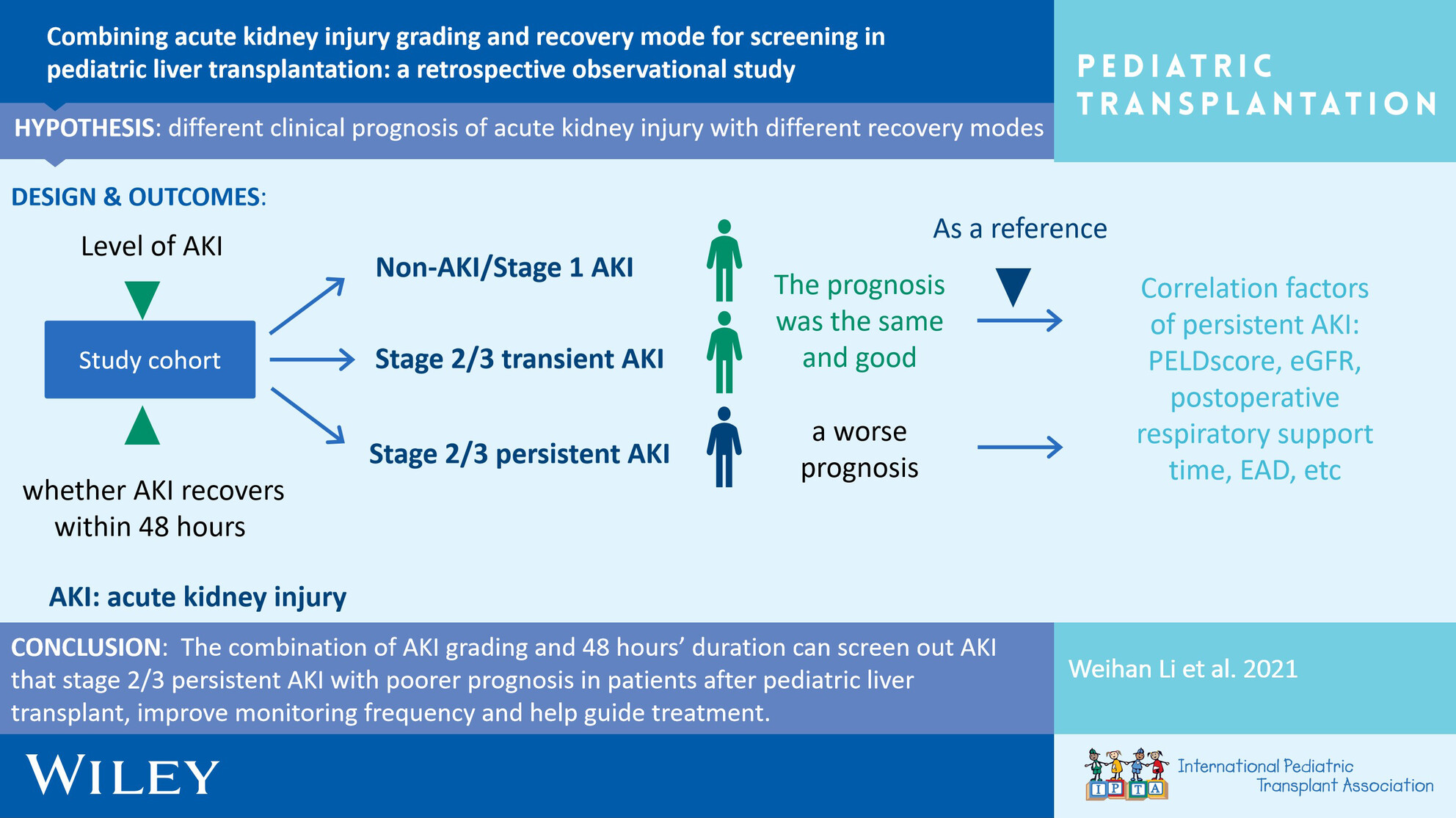
This is a retrospective study to investigate the incidence and clinical prognosis of acute kidney injury and different modes of recovery after pediatric liver transplantation.
-
Association of Neutropenia With Valganciclovir Prophylaxis Dosing Practices Within Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
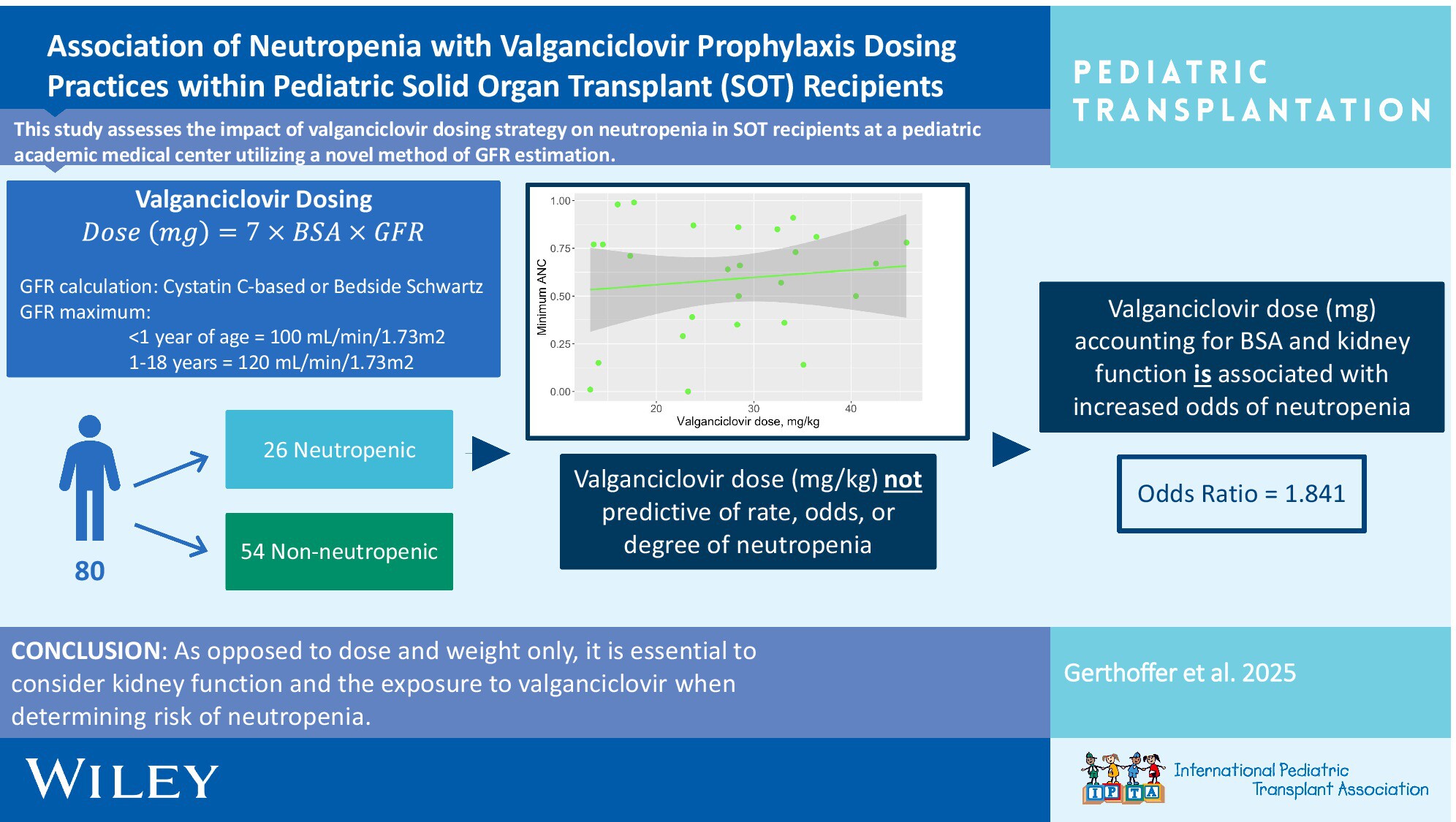
It is crucial to consider kidney function and the exposure to valganciclovir vs. dose alone when determining the risk of neutropenia in pediatric solid organ transplant recipients. Utilizing BSA-based dosing, Cystatin C-based GFR estimation, and appropriate upper limits of GFR for age was associated with a lower rate of neutropenia.
-
From Referral to Consent: Unveiling Racial Disparities at Critical Stages of Pediatric Organ Donationno
Graphical Abstract
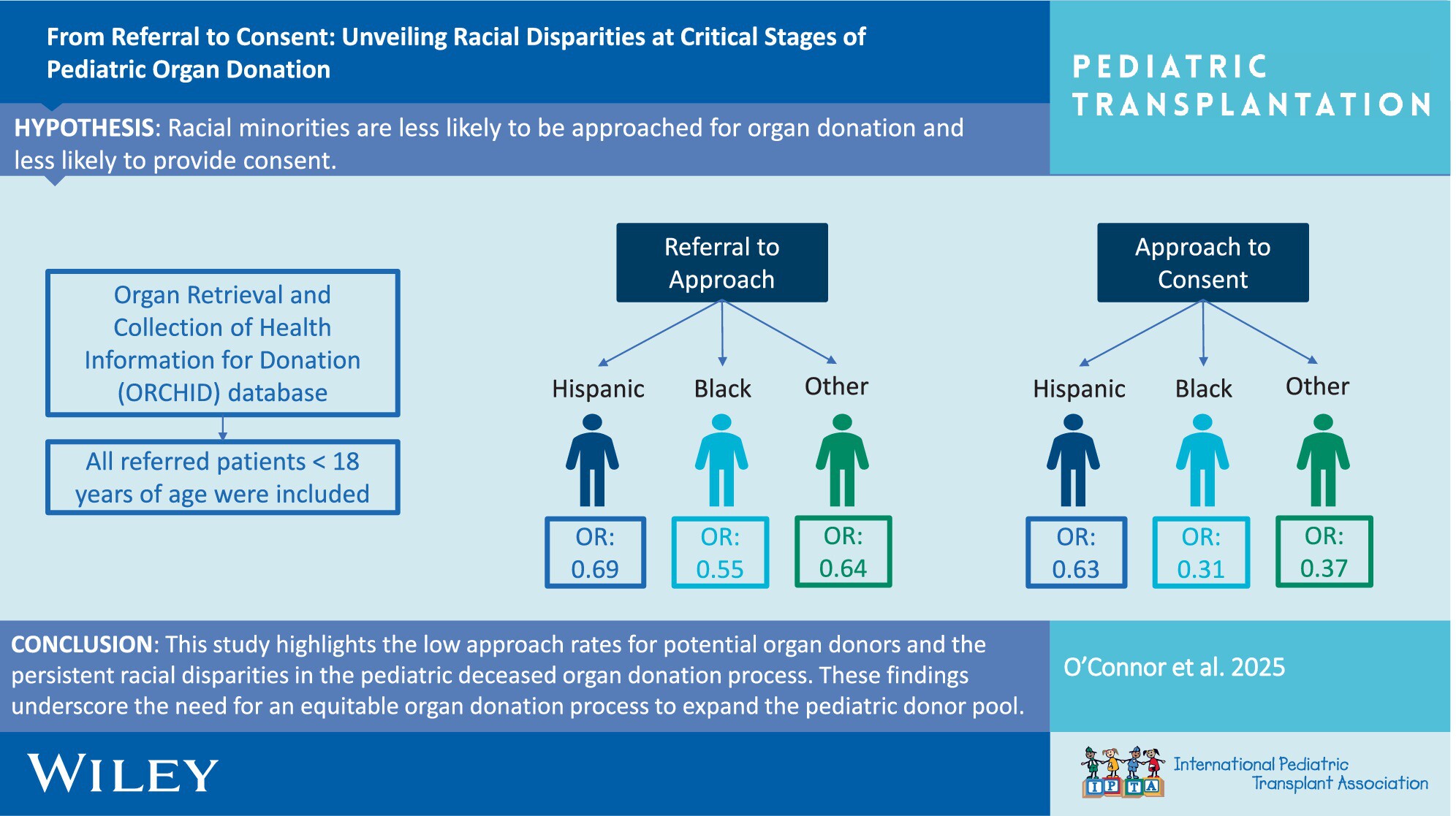
This study highlights the low approach rates for potential organ donors and the persistent racial disparities in the pediatric deceased organ donation process. Racial minority groups are less likely to be approached for donation and consent compared to Whites. These findings underscore the need for an equitable organ donation process to expand the pediatric donor pool.
-
Recurrence of Primary Sclerosing Cholangitis After Pediatric Liver Transplantation: A Single-Center, Retrospective Study in Japanno
Graphical Abstract
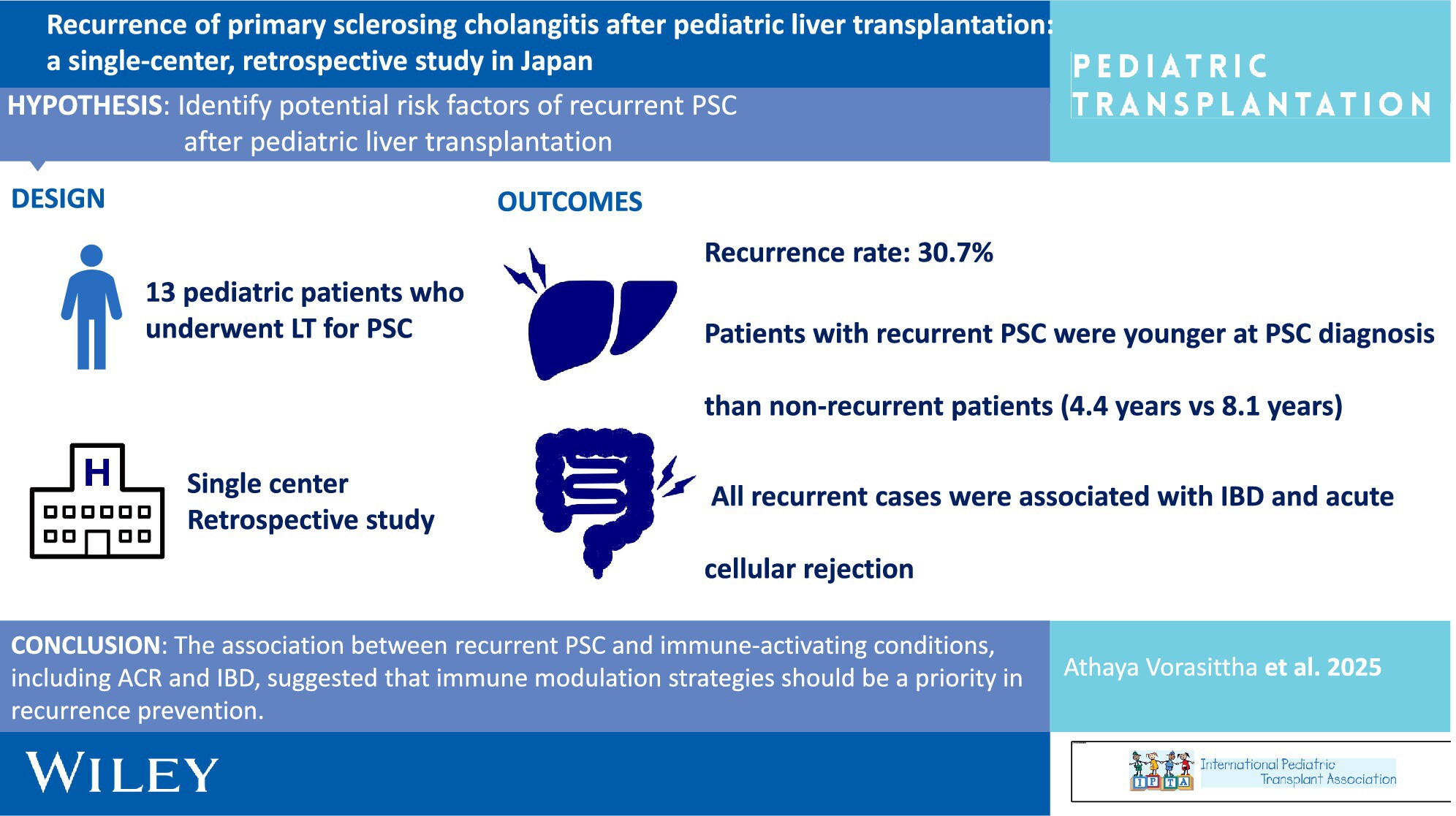
The recurrence rate was high in pediatric patients with PSC, emphasizing the need for tailored management strategies in children. The association between recurrent PSC and immune-activating conditions, including ACR and IBD, suggested that immune modulation strategies should be a priority in recurrence prevention.
-
Absence of Pupillary Reflexes in Pediatric Acute Liver Failure and Neurological Outcome After Liver Transplantationoa
Graphical Abstract
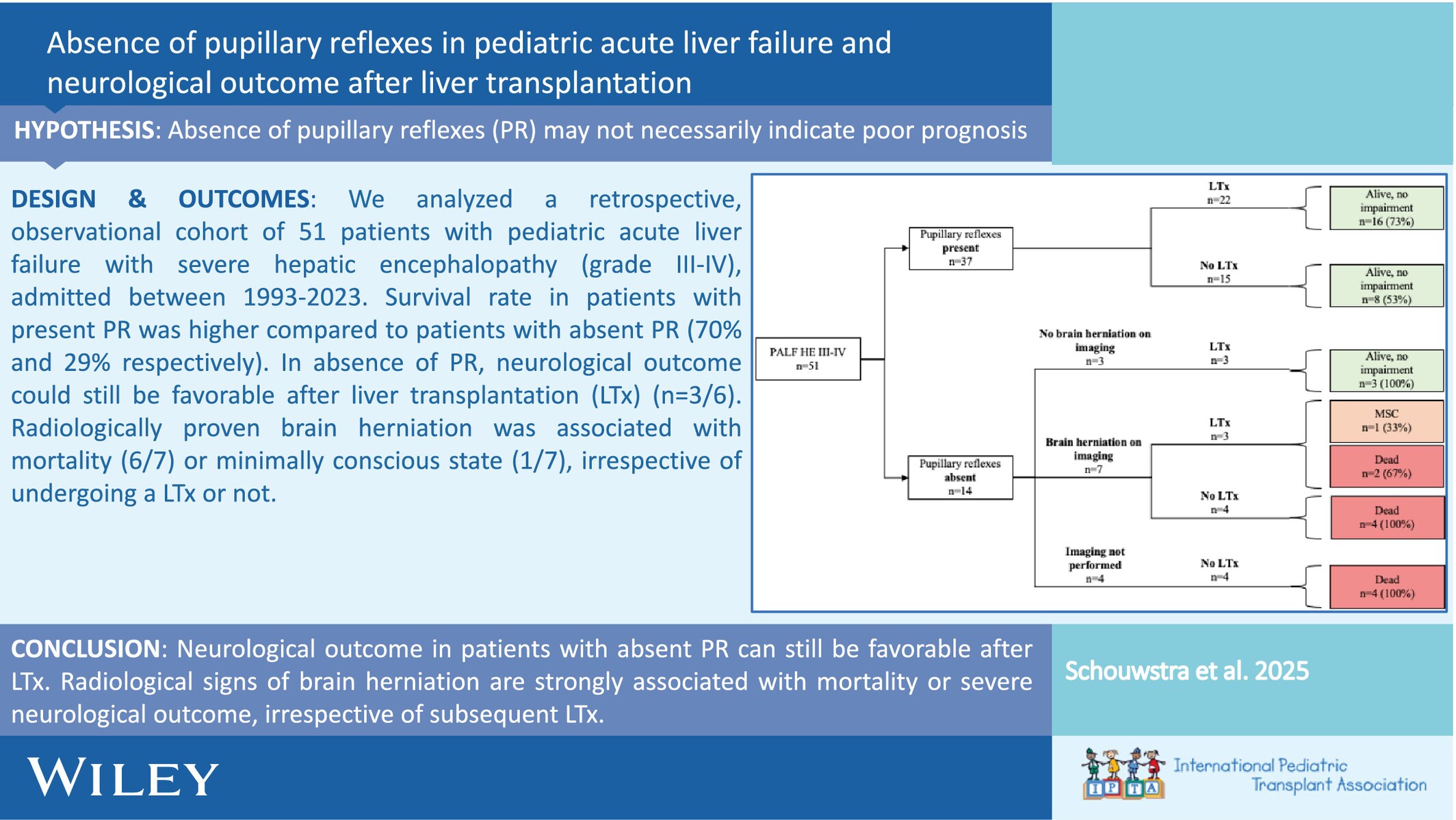
We analyzed a retrospective, observational cohort of 51 patients with pediatric acute liver failure with severe hepatic encephalopathy (grade III-IV), admitted between 1993 and 2023. The survival rate in patients with present PR was higher compared to patients with absent PR (70% and 29%, respectively). In the absence of PR, the neurological outcome could still be favorable after liver transplantation (LTx) (n = 3/6). Radiologically proven brain herniation was associated with mortality (6/7) or minimally conscious state (1/7), irrespective of undergoing a LTx or not.
-
Short and Long-Term Outcomes of Liver Transplantation in Pediatric Patients With Inborn Errors of Metabolism: A Single-Center Studyno
Graphical Abstract
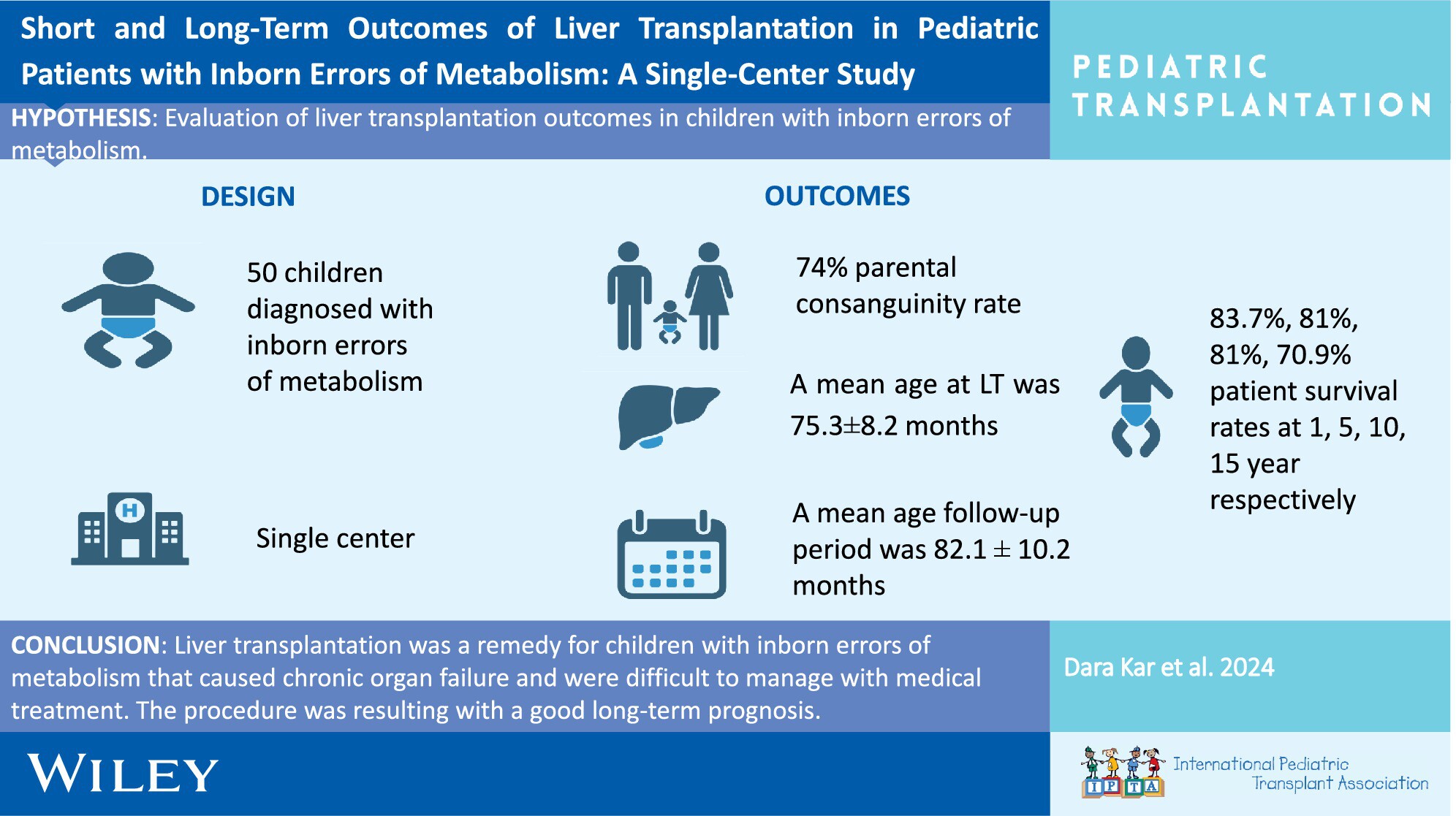
In our single-center study, we retrospectively analyzed 50 patients who underwent liver transplantation with the diagnosis of IEM. The parental consanguinity rate was 74%. The mean age at liver transplantation was 75.3 ± 8.2 months (range: 5–218), with a follow-up period of 82.1 ± 10.2 months (range:1 day–229 months). Survival rates at 1, 5, 10, and 15 years were 83.7%, 81%, 81%, and 70.9%, respectively. Liver transplantation is an effective solution for children with IEM causing chronic organ failure and difficult to manage with medical treatment, showing good long-term prognosis.
-
ABO Incompatible Grafts Are Associated With Excellent Outcomes in Pediatric Liver Transplant Recipients: An Important Resource to Reduce Waitlist Mortalityno
Graphical Abstract
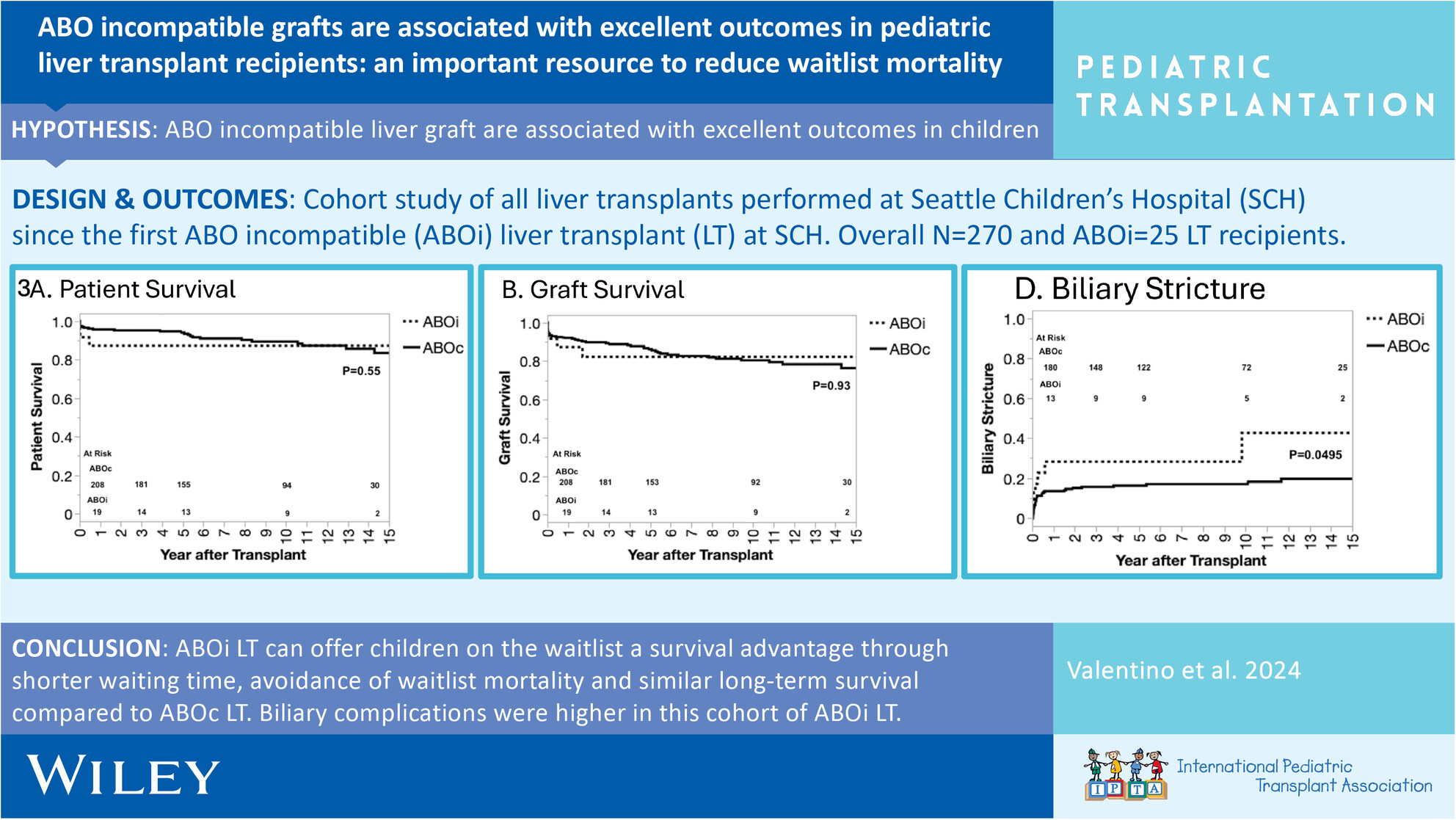
This is a large single-center investigation of pediatric ABO incompatible (ABOi) liver transplants (LT) in the United States demonstrating equivalent survival outcomes following transplantation, when compared to ABO compatible LT, and without an increase in acute rejection or vascular complications. Advocacy efforts are needed in the United States to change allocation policy to expand access to ABOi LT for children on the LT waitlist.
-
Bladder Outcomes in Bilateral Renal Agenesisno
Graphical Abstract
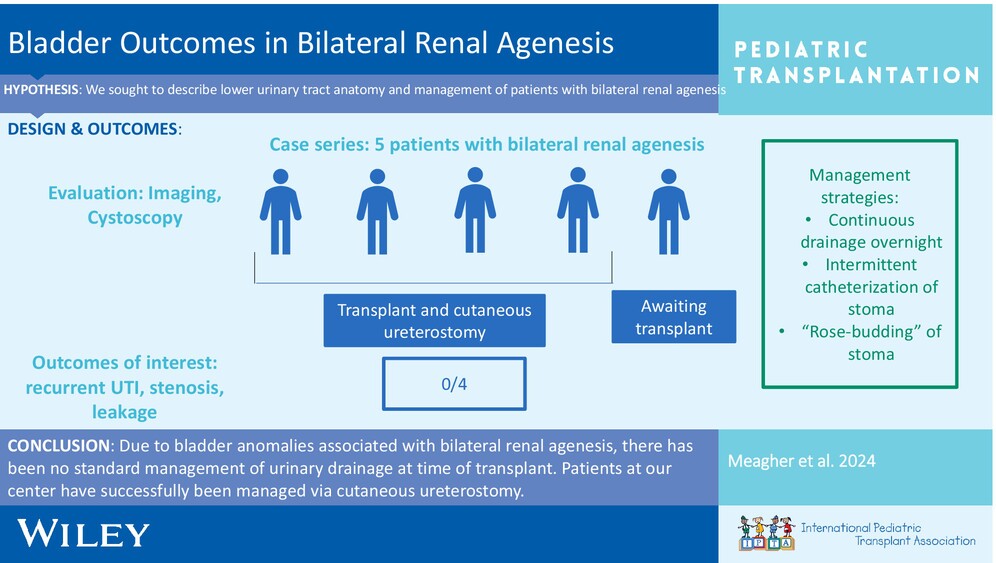
We present the lower urinary tract management of our patients with bilateral renal agenesis. As these patients do not have bladders, they are managed via cutaneous ureterostomy concurrently with kidney transplantation.