


All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
Absolute CD3+ T-Cell Counts After Anti-Thymocyte Globulin: Impact on Graft and Infectious Outcomes in Pediatric Kidney Recipientsno
Graphical Abstract
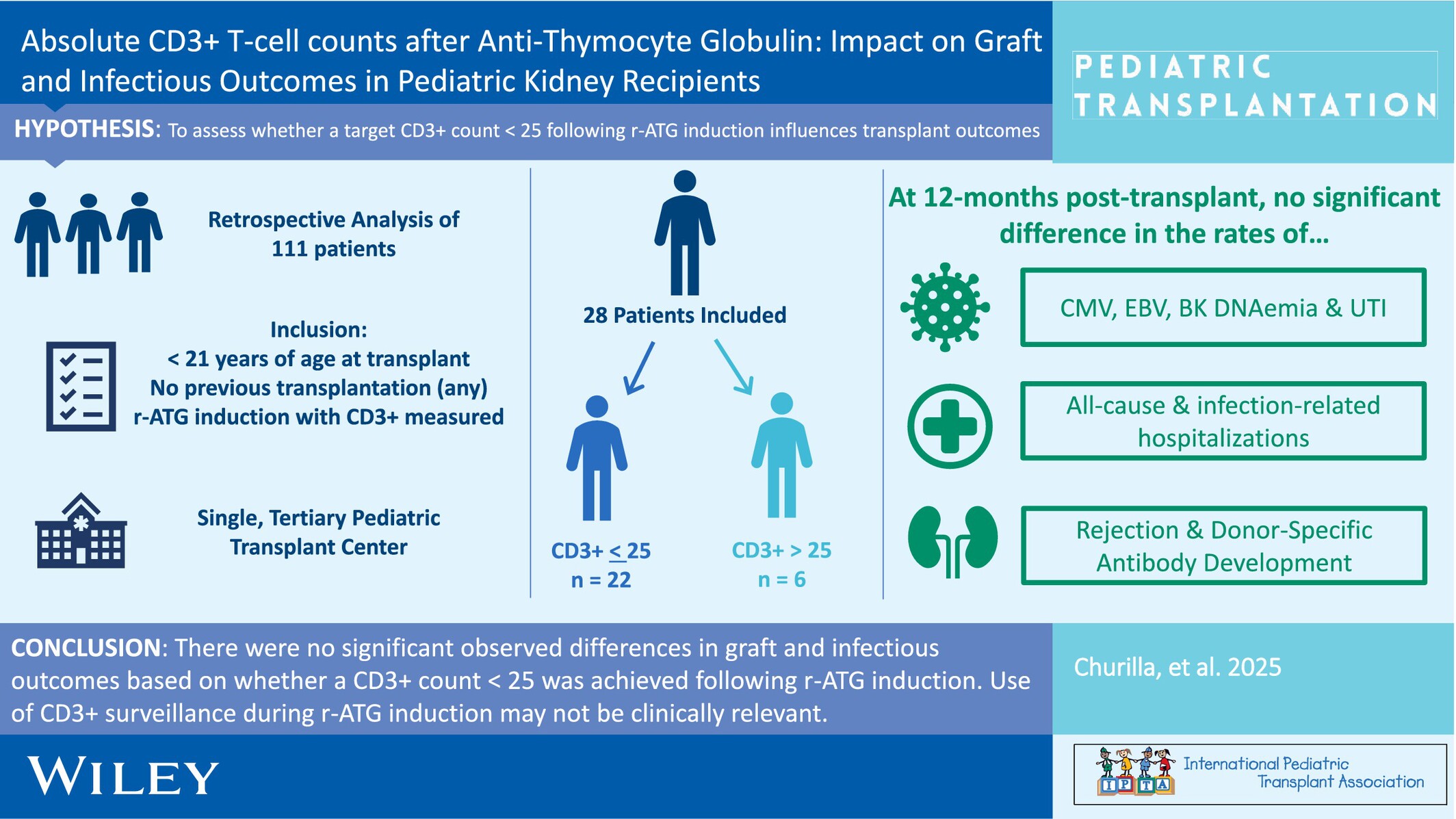
When pediatric kidney transplant recipients were compared based on the achievement (or not) of a CD3+ T-cell count < 25 cells/mm3 following rabbit anti-thymocyte globulin induction, there were no differences in infectious or graft outcomes by 12-months post-transplant.
-
Pneumocystis jiroveci Pneumonia Infections in Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
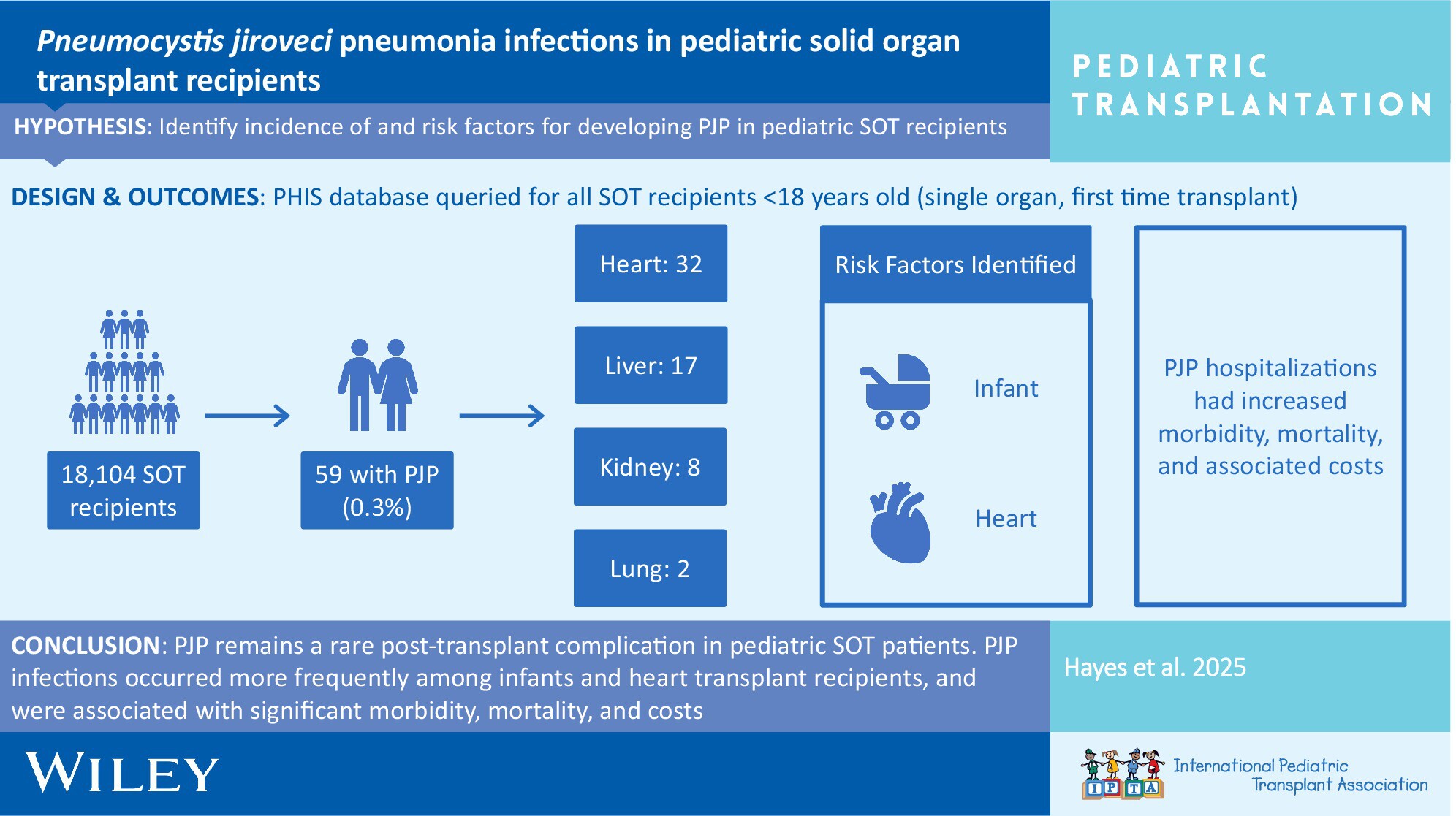
In the current era, PJP remains a rare post-transplant complication in pediatric SOT patients. PJP infections are associated with significant morbidity, mortality, and costs. Risk factors for PJP are young age at transplant and heart transplantation. An assessment of individual risk factors should be regularly performed to optimize prevention strategies.
-
Association of Neutropenia With Valganciclovir Prophylaxis Dosing Practices Within Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
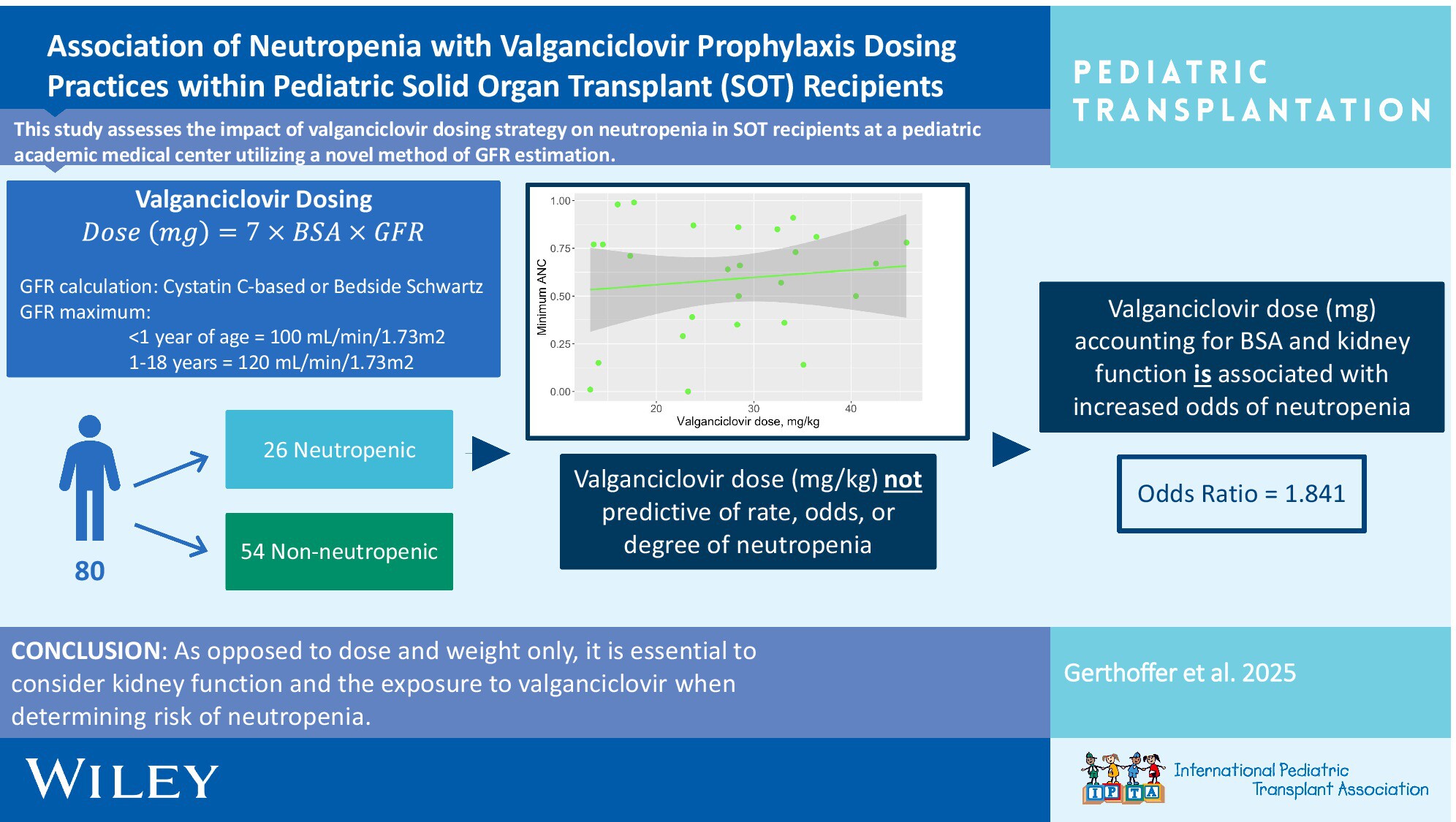
It is crucial to consider kidney function and the exposure to valganciclovir vs. dose alone when determining the risk of neutropenia in pediatric solid organ transplant recipients. Utilizing BSA-based dosing, Cystatin C-based GFR estimation, and appropriate upper limits of GFR for age was associated with a lower rate of neutropenia.
-
Low Incidence of Rejection and De Novo Donor-Specific Antibody Formation Following COVID-19 Vaccination or Infection Among Pediatric Kidney Transplant Recipientsno
Graphical Abstract
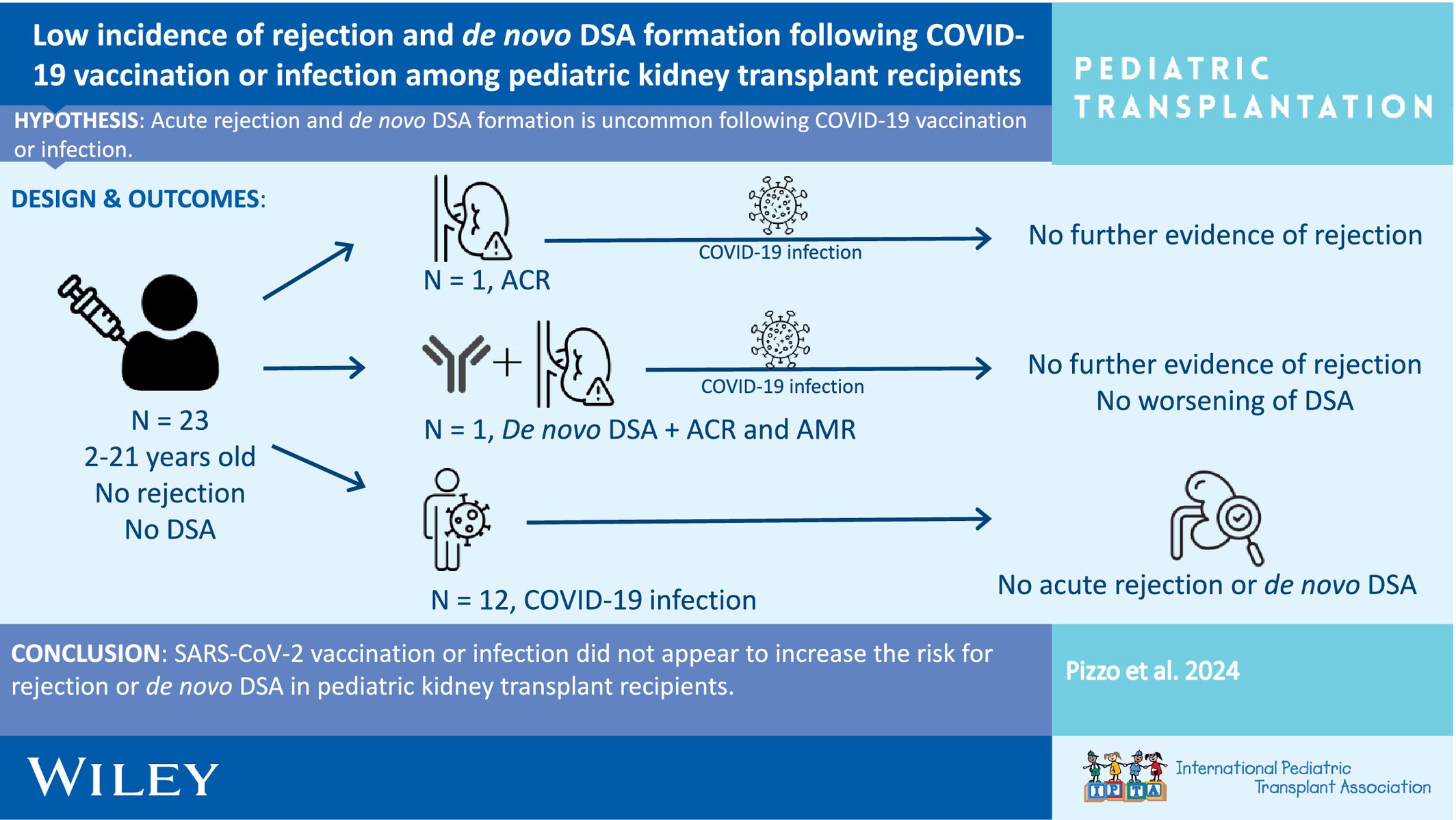
This study investigated the incidence of allograft rejection and de novo donor-specific antibody formation following COVID-19 vaccination or infection among pediatric kidney transplant recipients.
-
Recurrence of Primary Sclerosing Cholangitis After Pediatric Liver Transplantation: A Single-Center, Retrospective Study in Japanno
Graphical Abstract
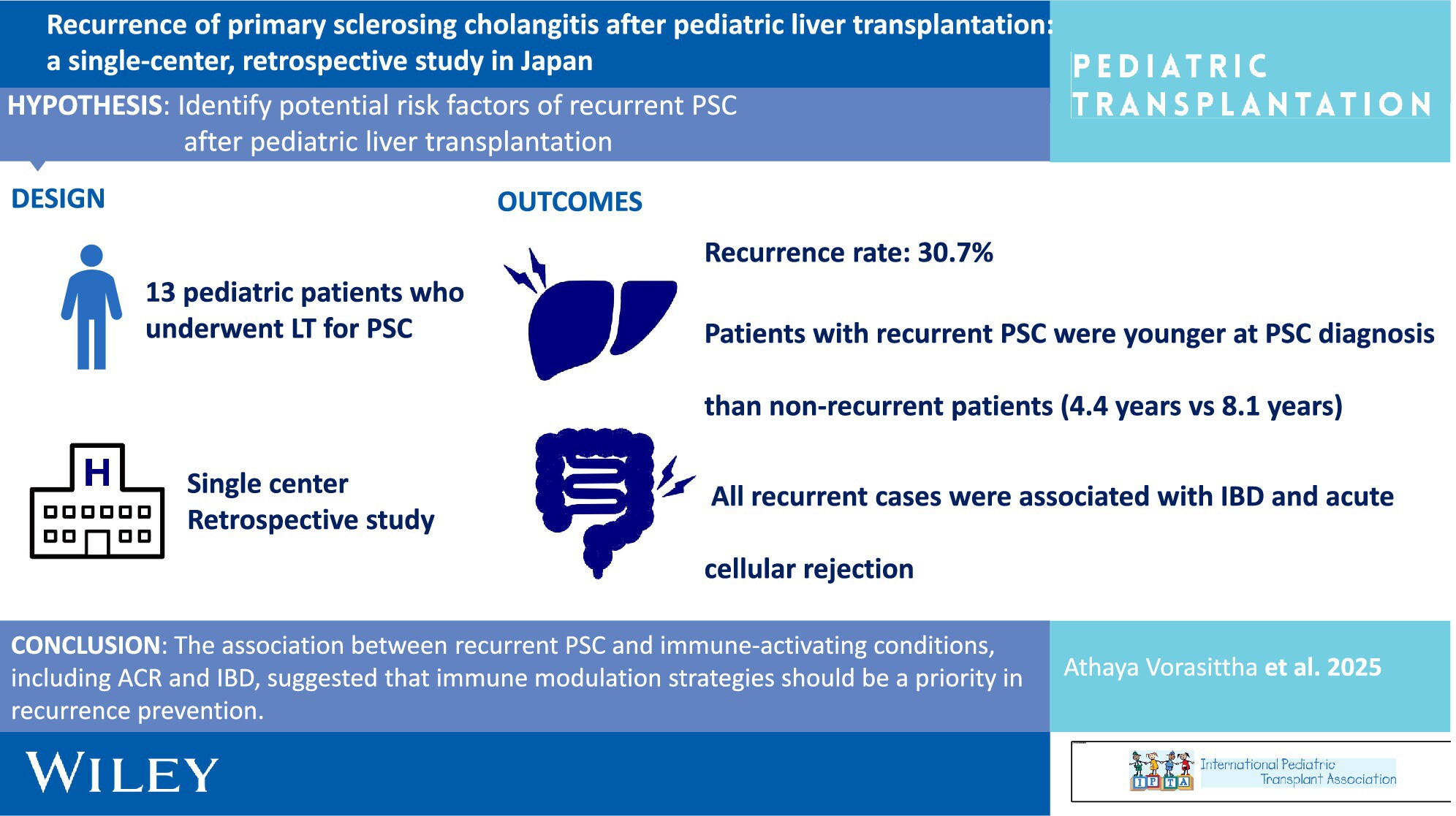
The recurrence rate was high in pediatric patients with PSC, emphasizing the need for tailored management strategies in children. The association between recurrent PSC and immune-activating conditions, including ACR and IBD, suggested that immune modulation strategies should be a priority in recurrence prevention.
-
Pre-Transplant Immunophenotyping in Pediatric Heart Transplant: A Role for the Immunologist?oa
Graphical Abstract
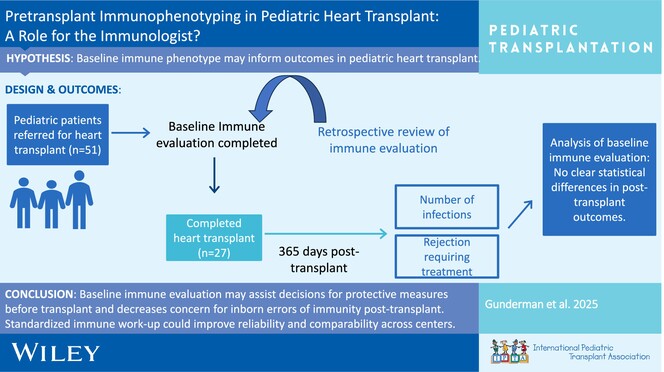
Baseline immune evaluation can assist in decisions for additional protective measures before transplant (avoidance of live vaccines, antimicrobial prophylaxis) and decrease the uncertainties in the evaluation of inborn errors of immunity after transplant. Ongoing work and developing standardized protocols for baseline immunologic work-up could improve reliability and comparability across different centers.
-
De Novo and Progressive Pulmonary Vein Stenosis Following Pediatric Heart Transplantation: A Multicenter Retrospective Studyno
Graphical Abstract
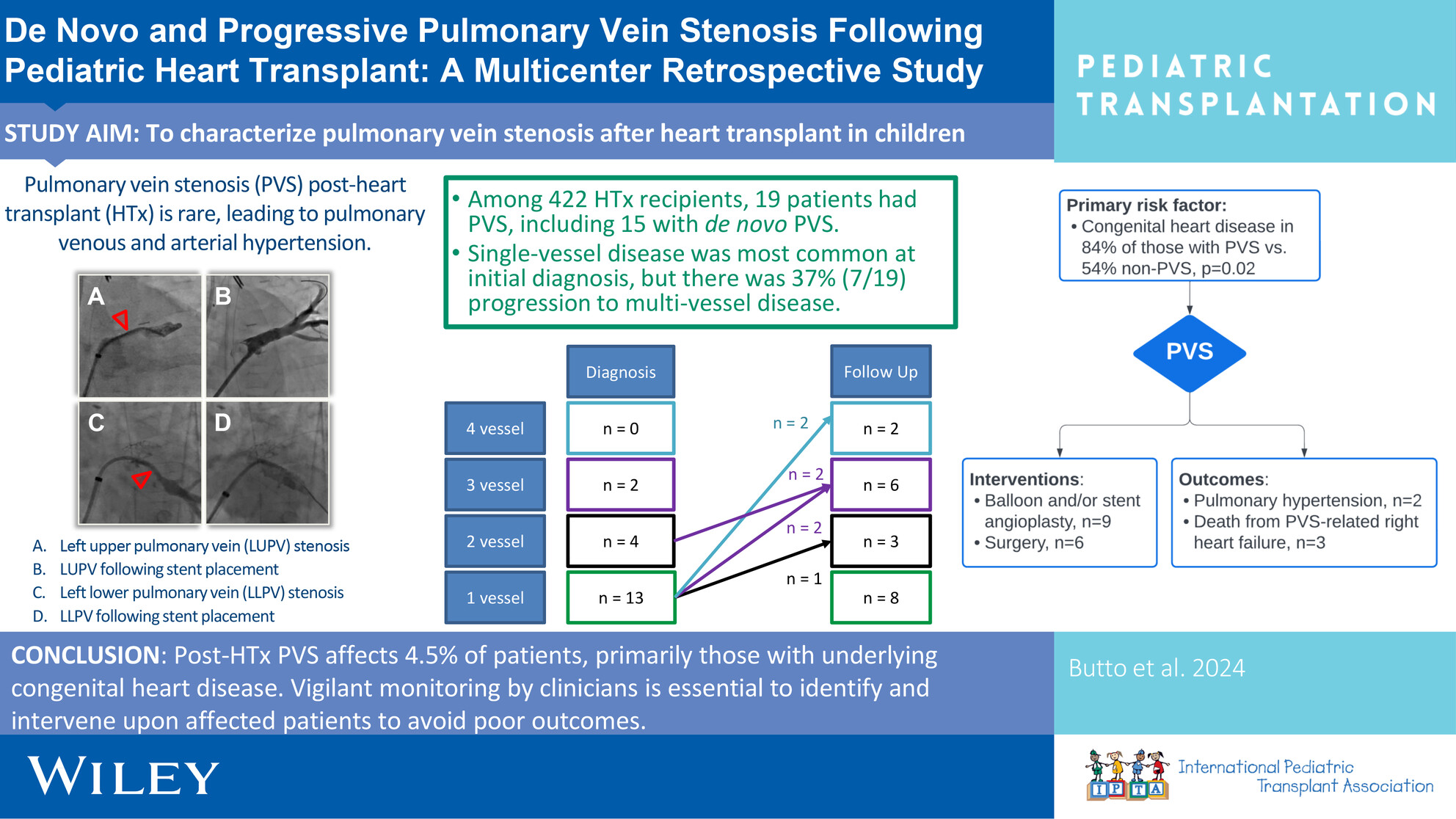
Investigating pulmonary vein stenosis following heart transplantation in children, this is the largest study of its kind that examines the prevalence, risk factors, and interventions for post-transplant PVS at two large transplant centers.
-
Norovirus Management and Outcomes in a Multicenter Pediatric Kidney Transplant Populationoa
Graphical Abstract
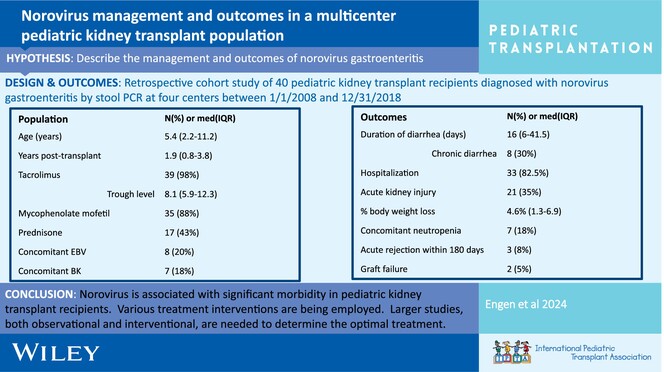
Post-transplant norovirus diarrhea persists for a median of 16 days (IQR 6–41.5 days) with 30% of patients developing chronic diarrhea. Morbidity is high, including AKI in 53% of patients, reduction in immunosuppression 20%, and acute rejection in 8% within 6 months of diagnosis.
-
Alemtuzumab induction is associated with decreased hospitalization rates in pediatric kidney transplant: A UNOS data review for safety and outcomes with common induction regimensno
Graphical Abstract
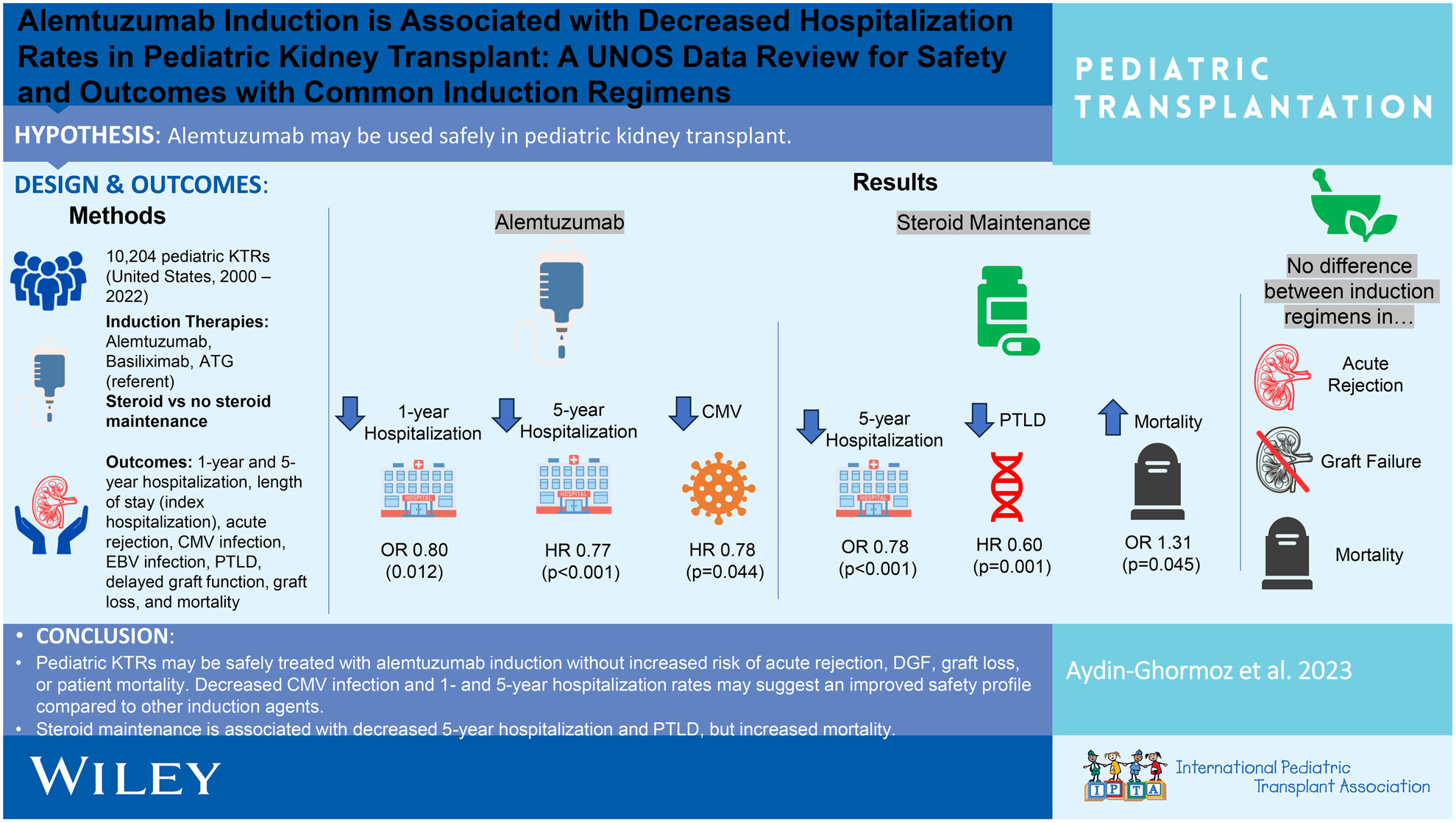
Pediatric KTRs may be safely treated with alemtuzumab induction without increased acute rejection, delayed graft function, graft loss, or patient mortality, but with decreased CMV infection and 1 and 5 years hospitalization rates. Steroid maintenance is associated with decreased 5 years hospitalization and PTLD, but increased mortality.
-
Safety and infectious outcomes in pediatric kidney transplant recipients after COVID-19 vaccination: A pediatric nephrology research consortium studyno
Graphical Abstract
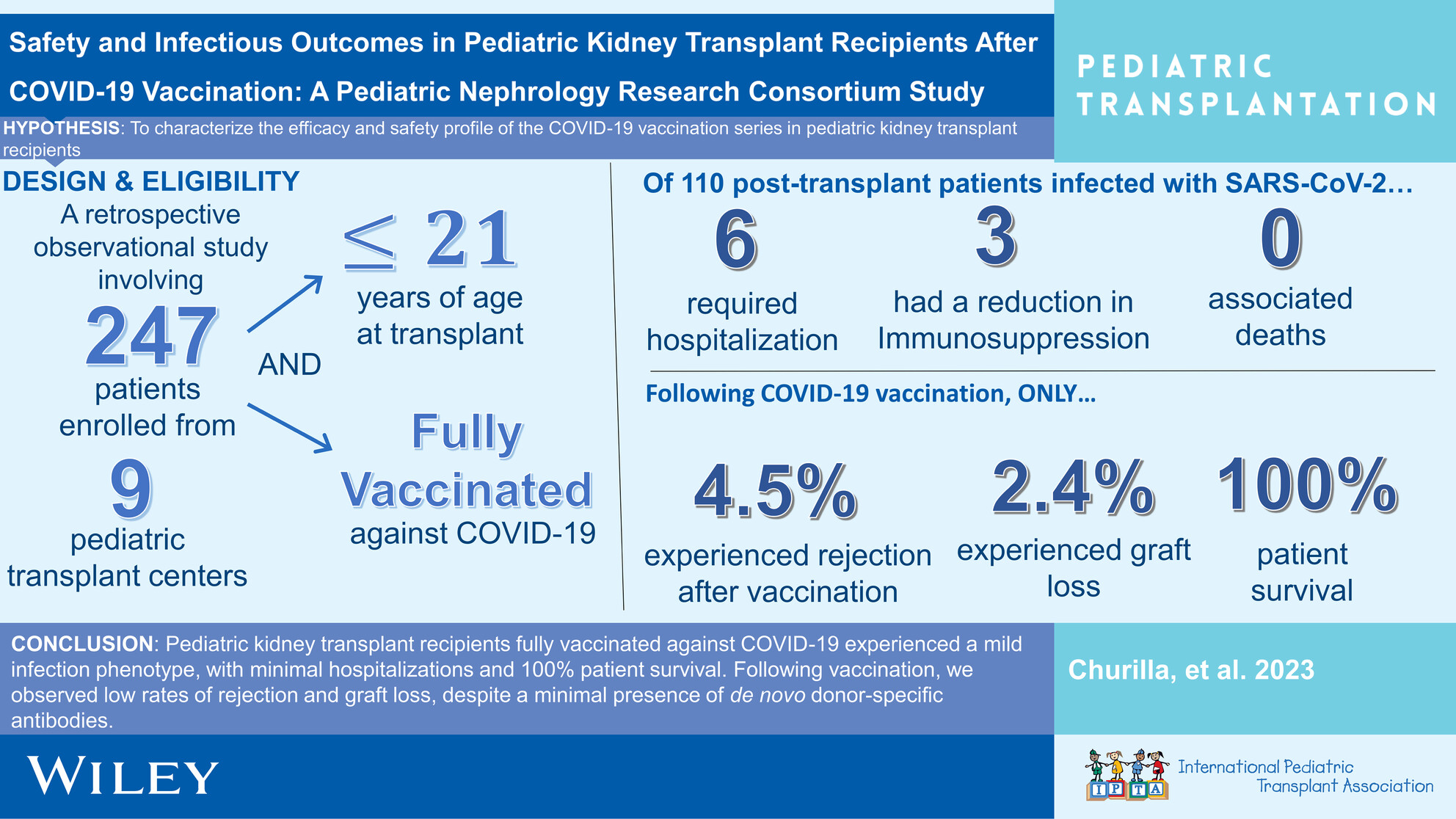
This observational, retrospective investigation demonstrates temporal associations pointing to a reassuring vaccine safety profile and mild SARS-Cov-2 infectious phenotype in pediatric renal transplant recipients fully vaccinated against COVID-19.
-
Epstein–Barr virus-associated post-transplant lymphoproliferative disorders in pediatric transplantation: A prospective multicenter study in the United Statesoa
Graphical Abstract
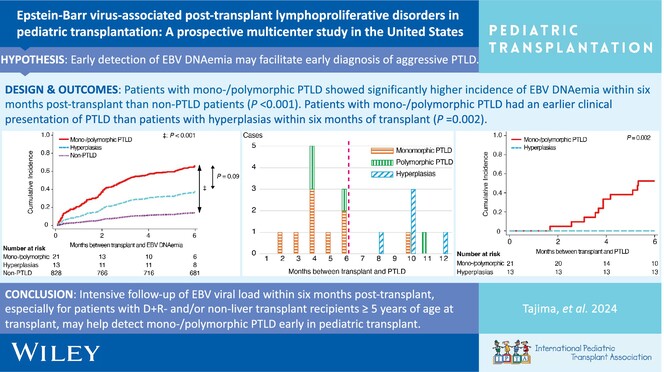
D+R− serostatus is significantly associated with the development of monomorphic/polymorphic PTLD. Intensive follow-up of EBV viral load within 6-month post-transplant, especially for patients with D+R− and/or non-liver transplant recipients ≥5 years of age at transplant, may help detect monomorphic/polymorphic PTLD early in pediatric transplant.
-
Long-term outcomes of two-dose alemtuzumab induction in pediatric kidney transplantationoa
Graphical Abstract
Pediatric kidney transplant recipients given two doses of alemtuzumab induction immunosuppression, with steroid-free maintenance immunosuppression, had a ten-year living-donor graft survival of 86.5% and a deceased donor graft survival of 57.7%. The incidence of viral infections was similar to that reported in other cohorts, and growth improved after transplant.
-
A novel approach to reducing hepatotoxicity related to fungal prophylaxis in pediatric lung transplant recipientsno
Graphical Abstract
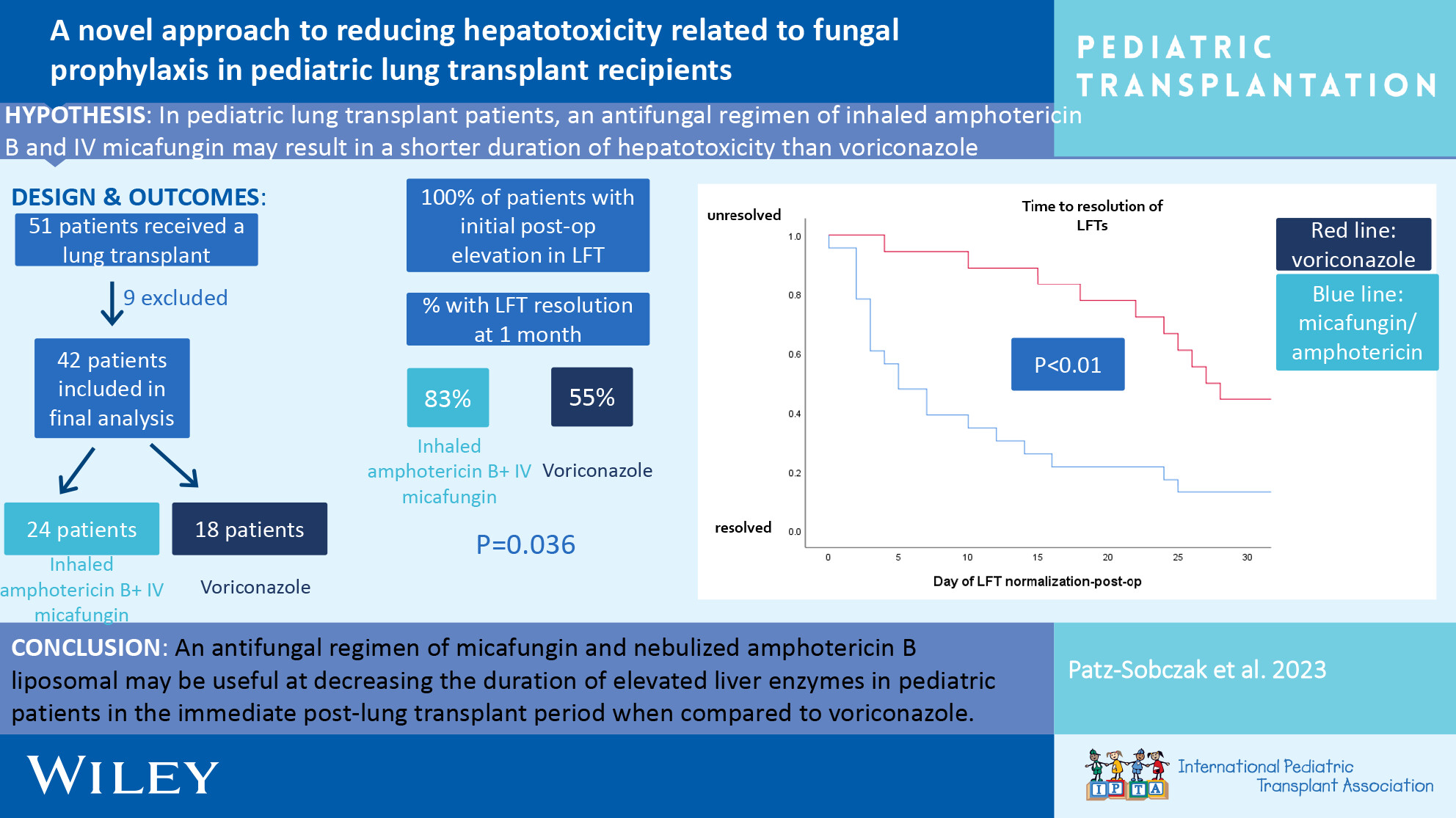
An antifungal regimen of micafungin and nebulized amphotericin B liposomal may be useful at decreasing the duration of elevated liver enzymes in pediatric patients in the immediate post-lung transplant period when compared to voriconazole monotherapy.
-
Effect of pre-emptive rituximab on EBV DNA levels and prevention of post-transplant lymphoproliferative disorder in pediatric kidney transplant recipients: A case series from the pediatric nephrology research consortiumno
Graphical Abstract
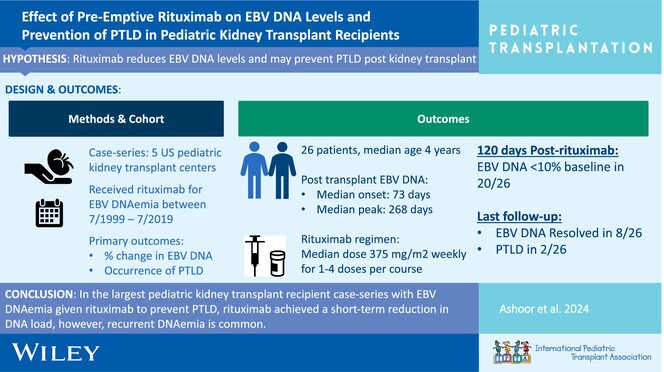
In the largest pediatric kidney transplant recipient case series with EBV DNAemia given rituximab to prevent PTLD, rituximab achieved a short-term reduction in DNA load; however, recurrent DNAemia is common.
-
Kidney transplant in pediatric gut transplant recipients – Technical challenges and outcomesno
Graphical Abstract
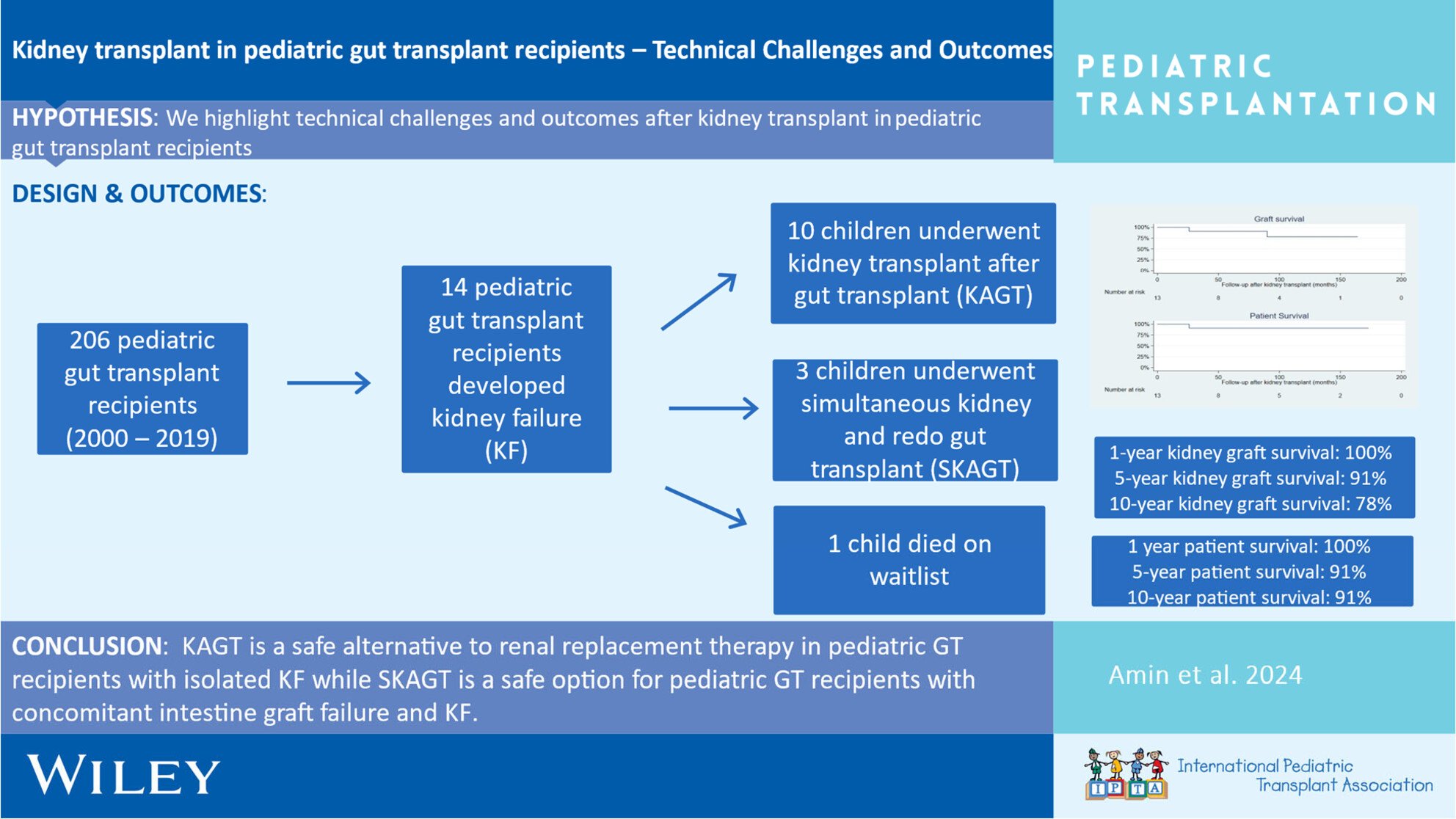
Excellent short- and long-term kidney transplant graft, gut transplant graft, and patient survival can be achieved through meticulous surgical technique and multidisciplinary peri-operative management of pediatric kidney after gut transplant recipients.