All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
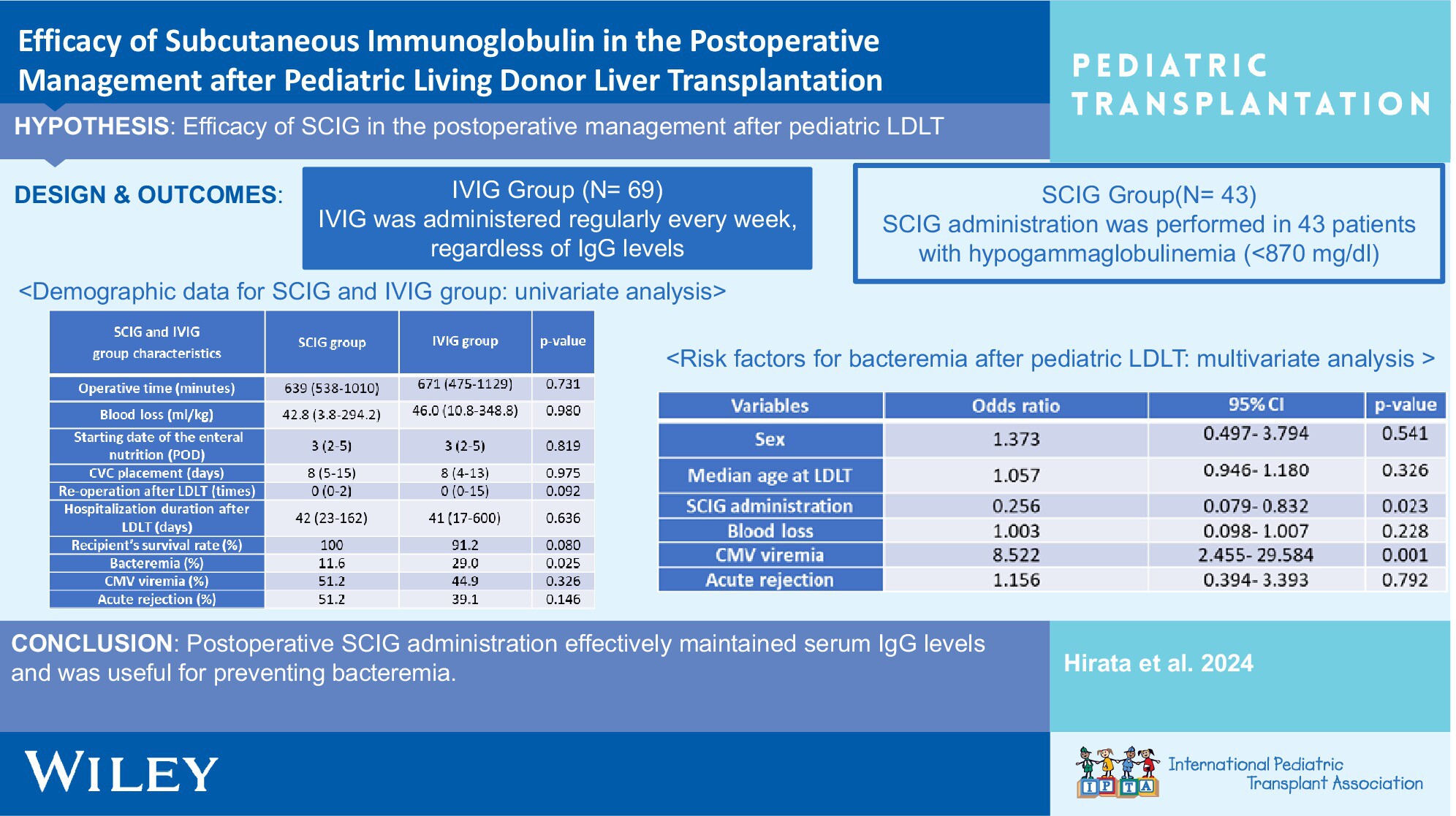
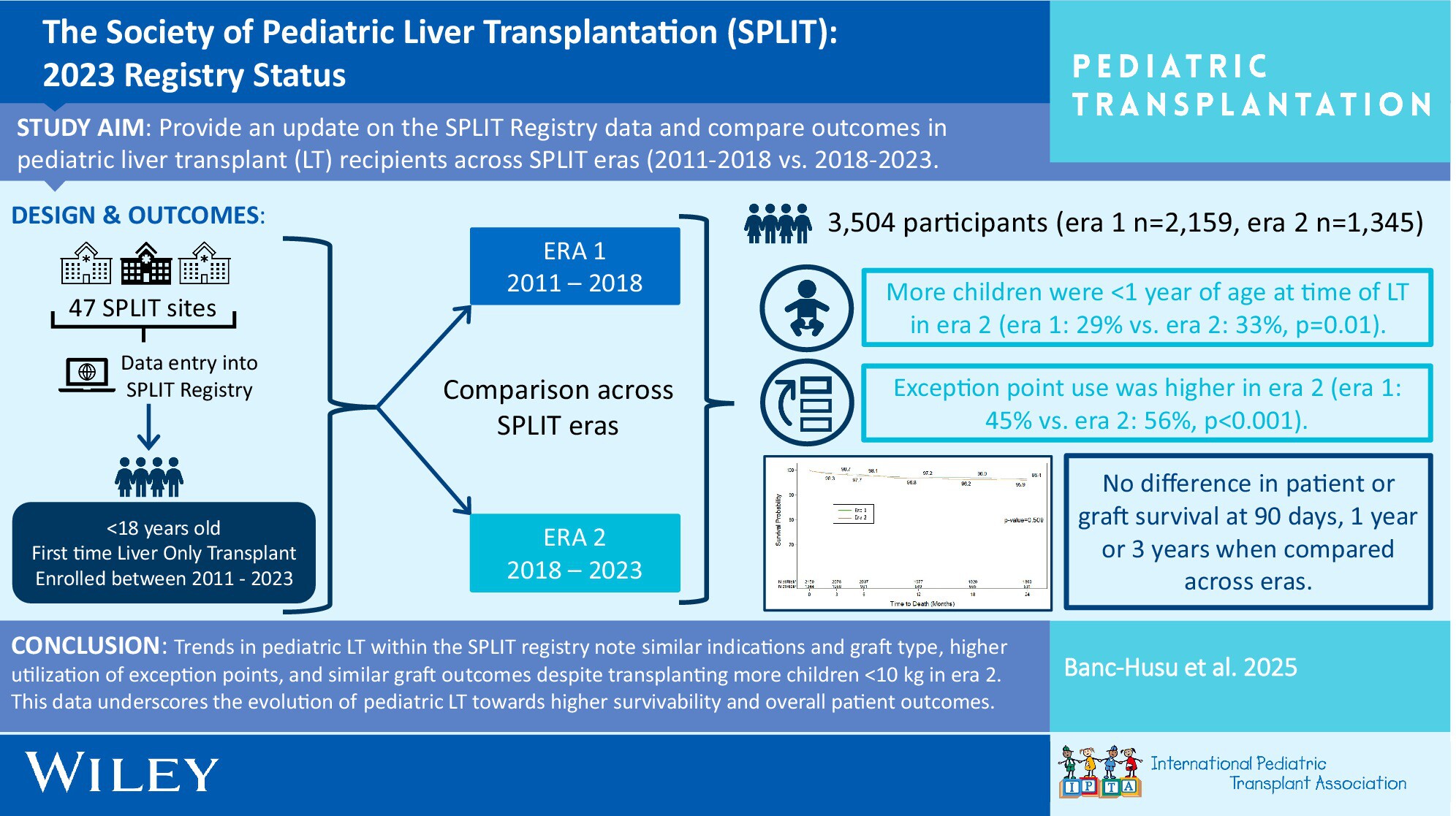
Incidence and Risk Factors of Fungal Infections Within 3 Months Following Pediatric Liver Transplantationno
Graphical Abstract
Invasive fungal infections occurred in nearly one-third of pediatric LT recipients who did not receive antifungal prophylaxis during the early posttransplant. Reexploratory laparotomy and postoperative bacterial infections were key risk factors. Early identification and close monitoring of high-risk patients are essential for improving clinical outcomes.
-
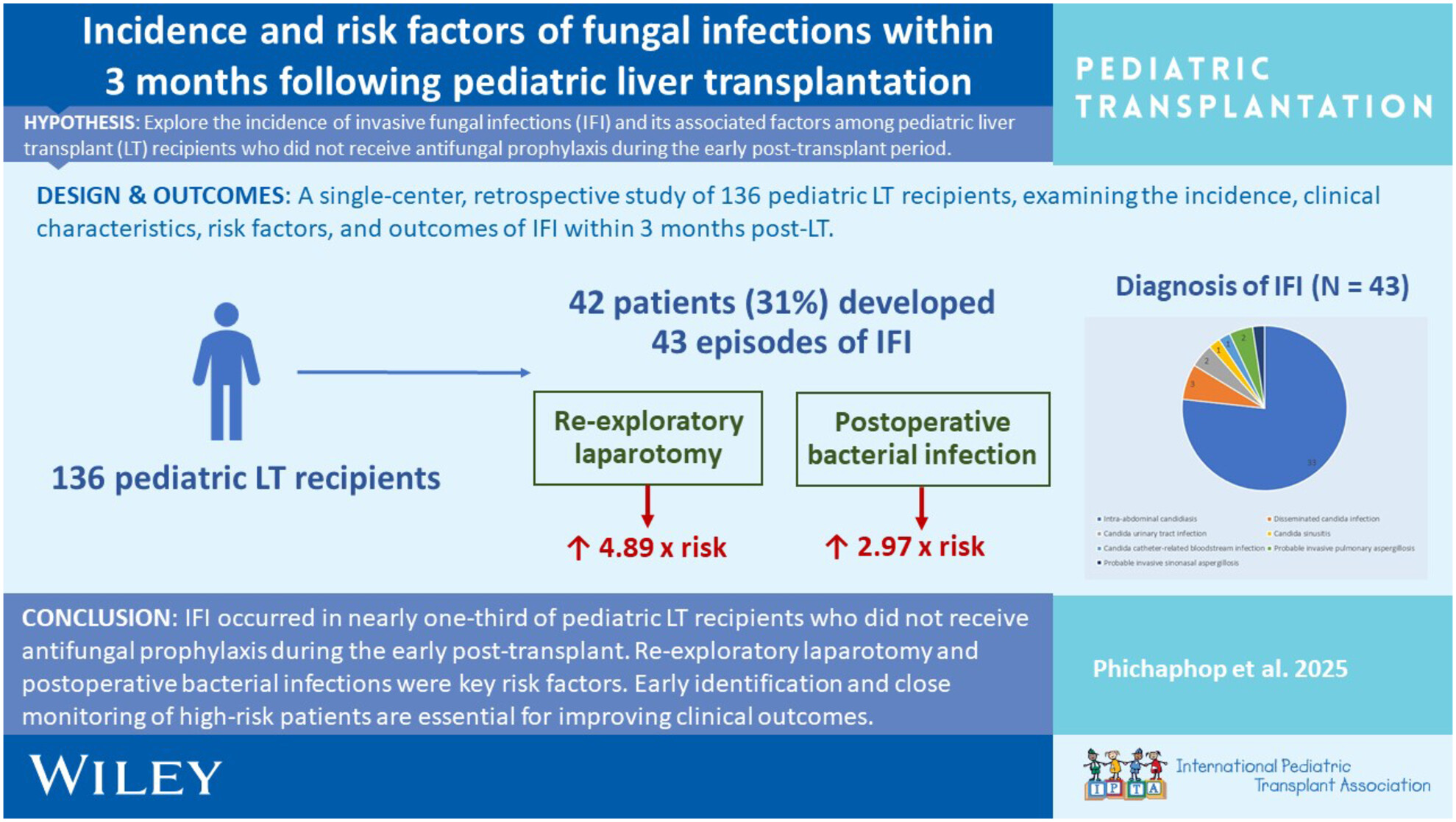
Semilunar Valve Function After Rejection in Heart Transplant Recipients: Implications for Partial Heart Transplantationoa
Graphical Abstract
To better understand the immunosuppression requirements for patients receiving partial heart transplants (PHTs), we investigated the effect of rejection episodes on the aortic and pulmonary valves of patients who received orthotopic heart transplants (OHTs). Compared to patients with no rejection, those who experienced rejection episodes had no clinically significant changes to their pulmonary or aortic valves. Knowing that rejection primarily targets the myocardium and spares the valve, intensive immunosuppression regimens required for graft protection in OHT may not be necessary for semilunar valve protection in PHT.
-
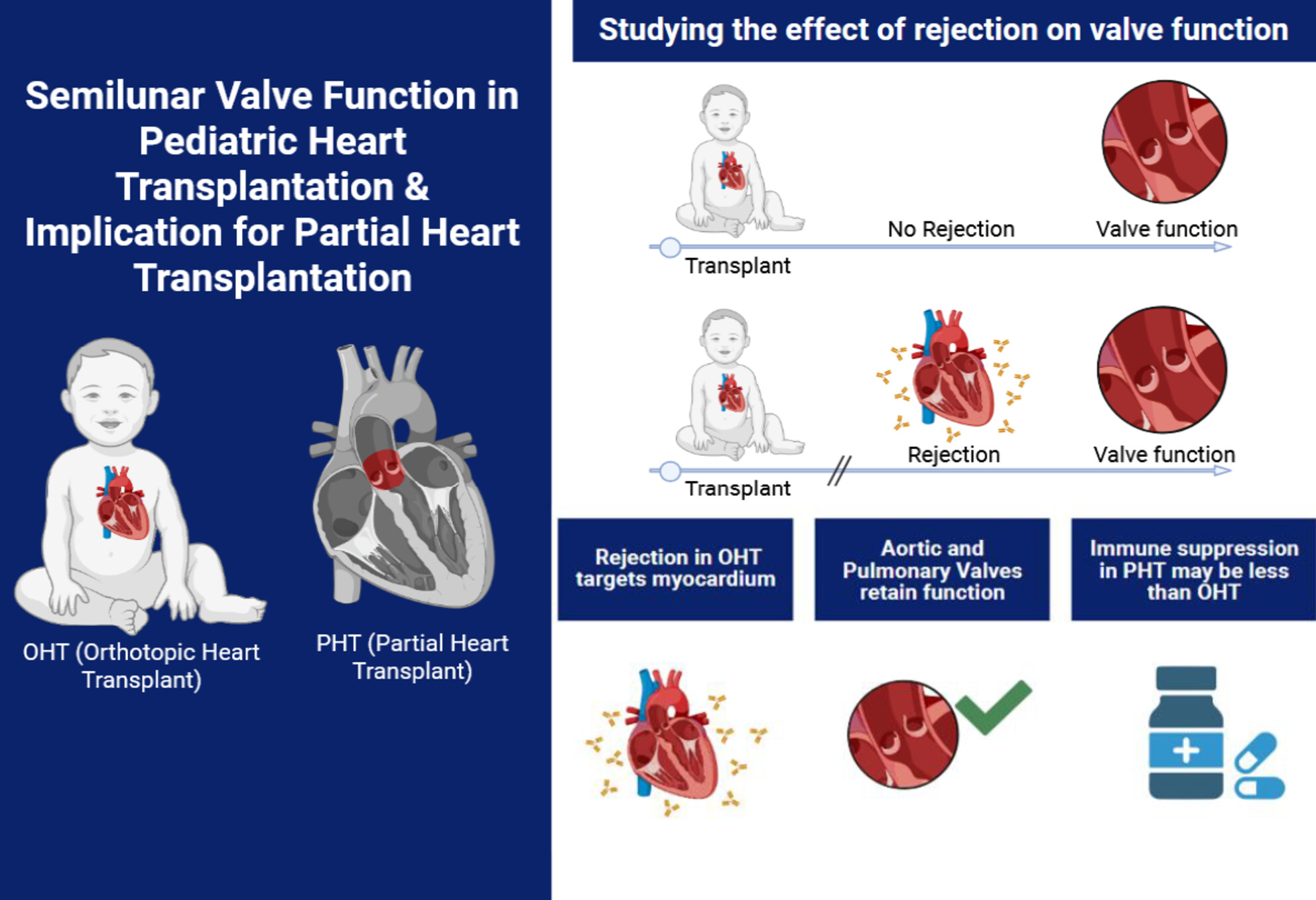
The Society of Pediatric Liver Transplantation (SPLIT): 2023 Registry Statusno
Graphical Abstract
Trends within the Society of Pediatric Liver Transplant (SPLIT) registry note similar indications and graft type, higher utilization of exception points, and lower hepatic artery thrombosis rates despite transplanting more children < 10 kg. This data underscores the evolution of pediatric LT toward higher survivability and overall improved patient outcomes.
-
Diffusion Tensor Imaging (DTI) as a Non-Invasive Tool for Assessing Pediatric Kidney Transplants: A Feasibility Studyoa
Graphical Abstract
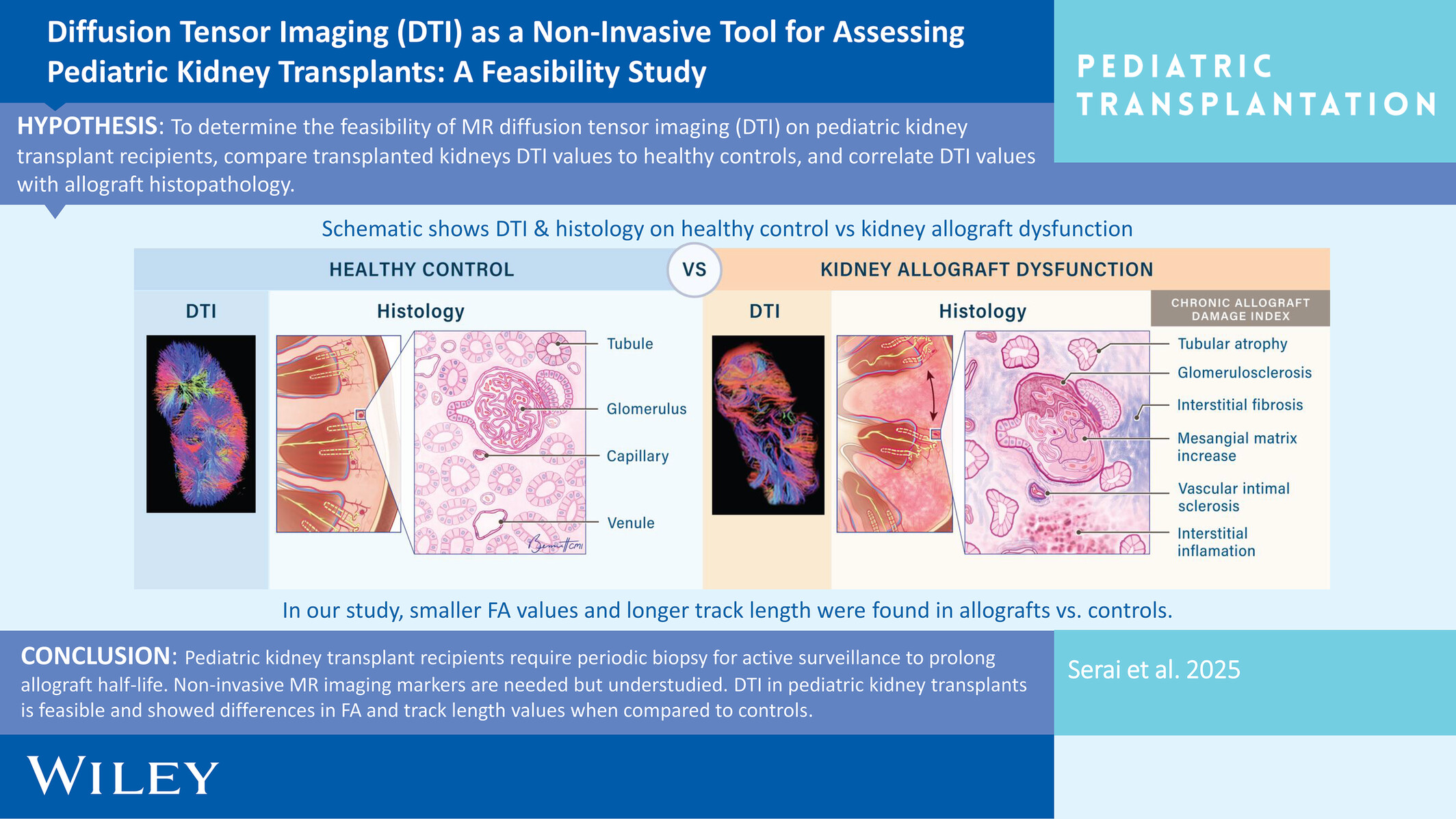
Our study demonstrates the feasibility of using diffusion tensor imaging (DTI) to evaluate pediatric kidney transplants. Significant differences in fractional anisotropy (FA) and track length were observed between transplanted and healthy kidneys, reflecting altered microstructural organization. While DTI metrics did not distinguish allografts by rejection status or chronic damage index, the findings support DTI's potential as a non-invasive biomarker for assessing kidney allograft health. Further research with larger cohorts is needed to validate these results and explore the clinical utility of DTI in pediatric kidney transplant management.
-
Induction With Antithymocyte Globulin Is Associated With Decreased Mortality and PTLD in Pediatric Liver Transplantation: A UNOS Data Analysisno
Graphical Abstract
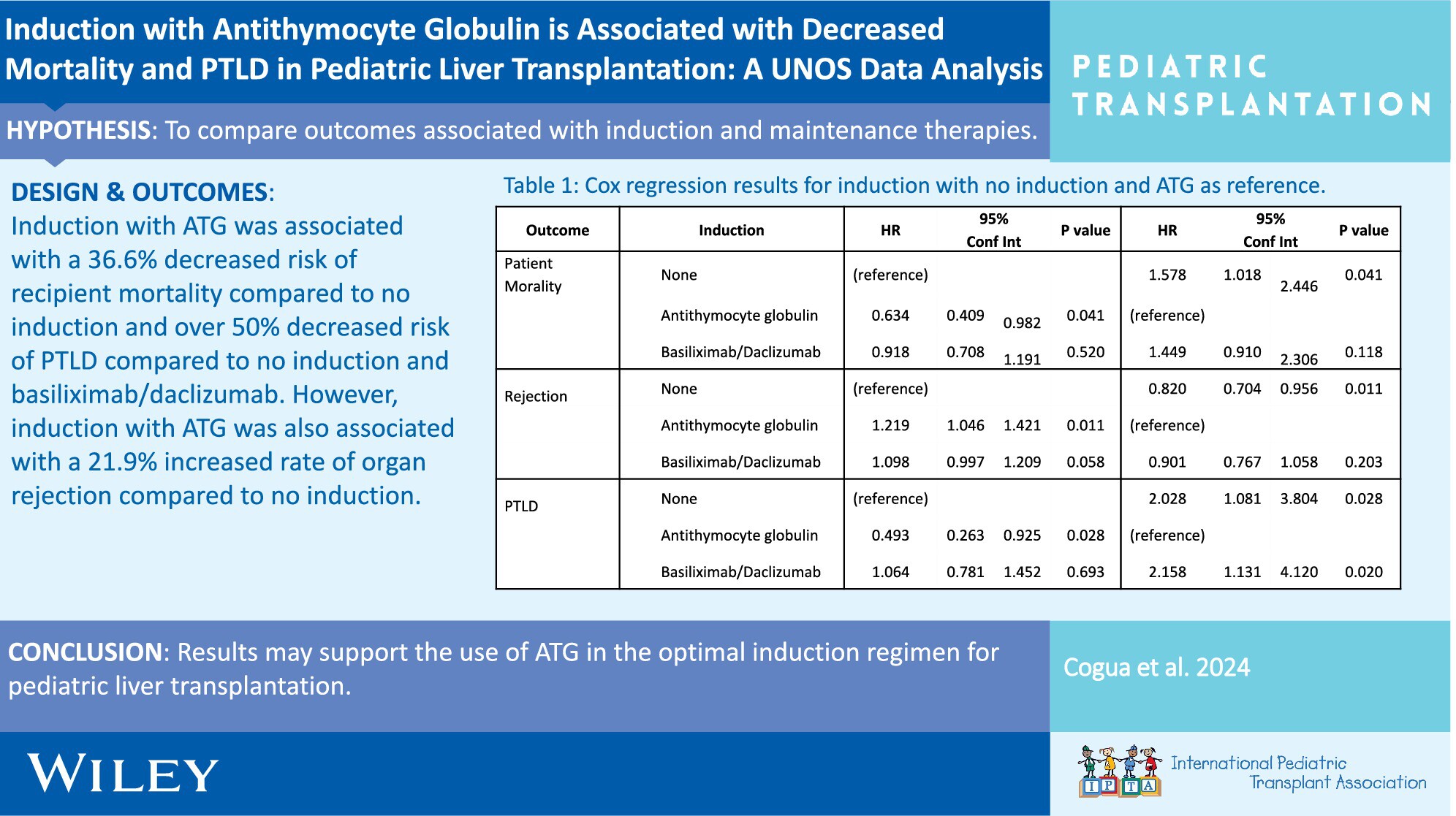
ATG induction is associated with decreased mortality and PTLD, but increased risk of organ rejection. Despite no differences in induction for the rate of graft failure and CMV, the decreased rate of mortality and PTLD with ATG induction may support its use in the optimal induction regimen for pediatric liver transplantation.
-
Early Post-Operative Versus Late Arrhythmias After Heart Transplant at a Pediatric Center: Incidence, Management, and Outcomesno
Graphical Abstract
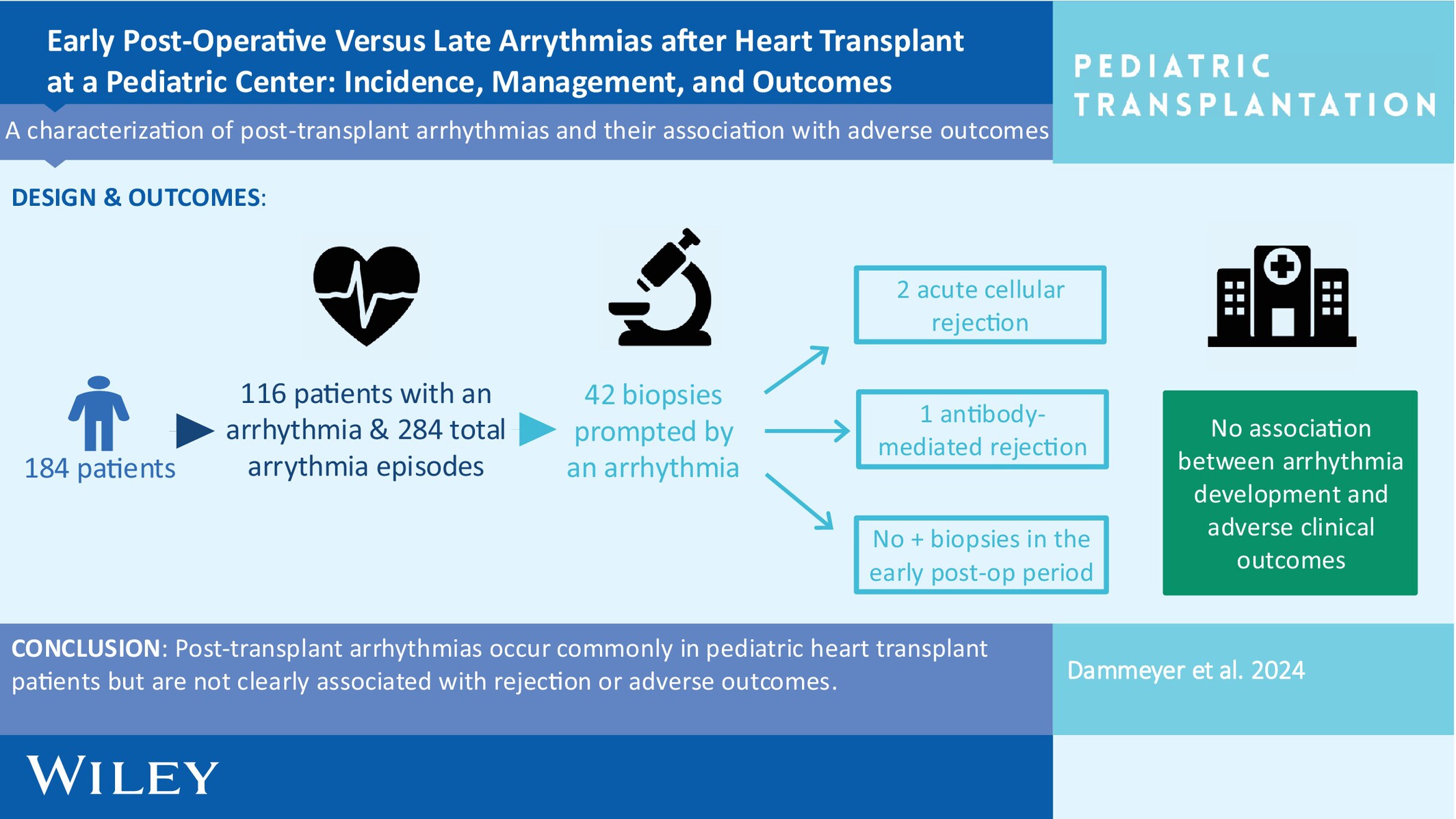
We sought to characterize the arrhythmias that occur after pediatric heart transplant and determine if the development of arrhythmia is associated with adverse outcomes. We found that arrhythmias are common after heart transplant but are not clearly associated with rejection or other adverse outcomes, including death, cardiac allograft vasculopathy, and retransplant.
-
Combining Acute Kidney Injury Grading and Recovery Mode for Screening in Pediatric Liver Transplantation: A Retrospective Observational Studyno
Graphical Abstract
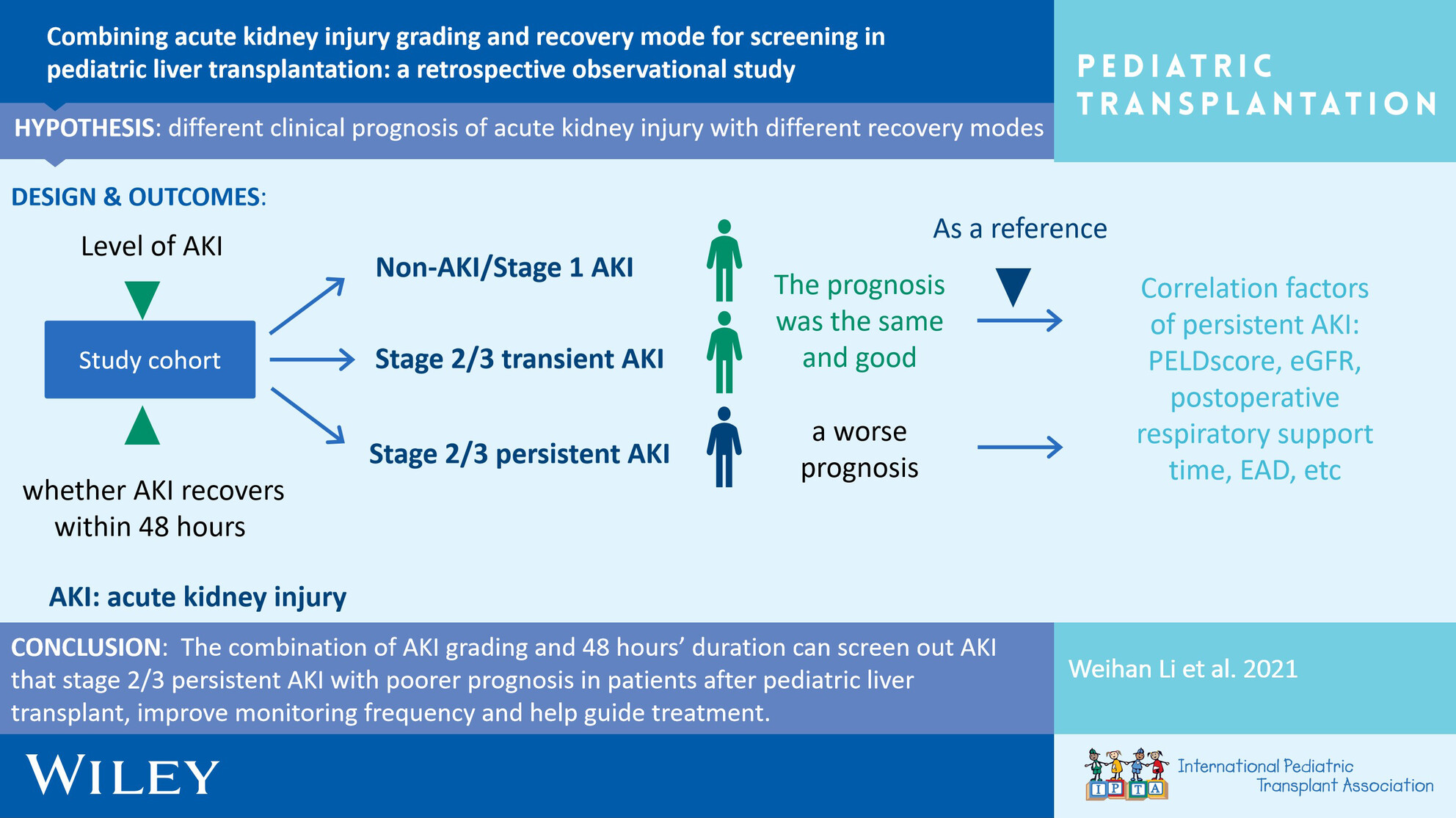
This is a retrospective study to investigate the incidence and clinical prognosis of acute kidney injury and different modes of recovery after pediatric liver transplantation.
-
Low Incidence of Rejection and De Novo Donor-Specific Antibody Formation Following COVID-19 Vaccination or Infection Among Pediatric Kidney Transplant Recipientsno
Graphical Abstract
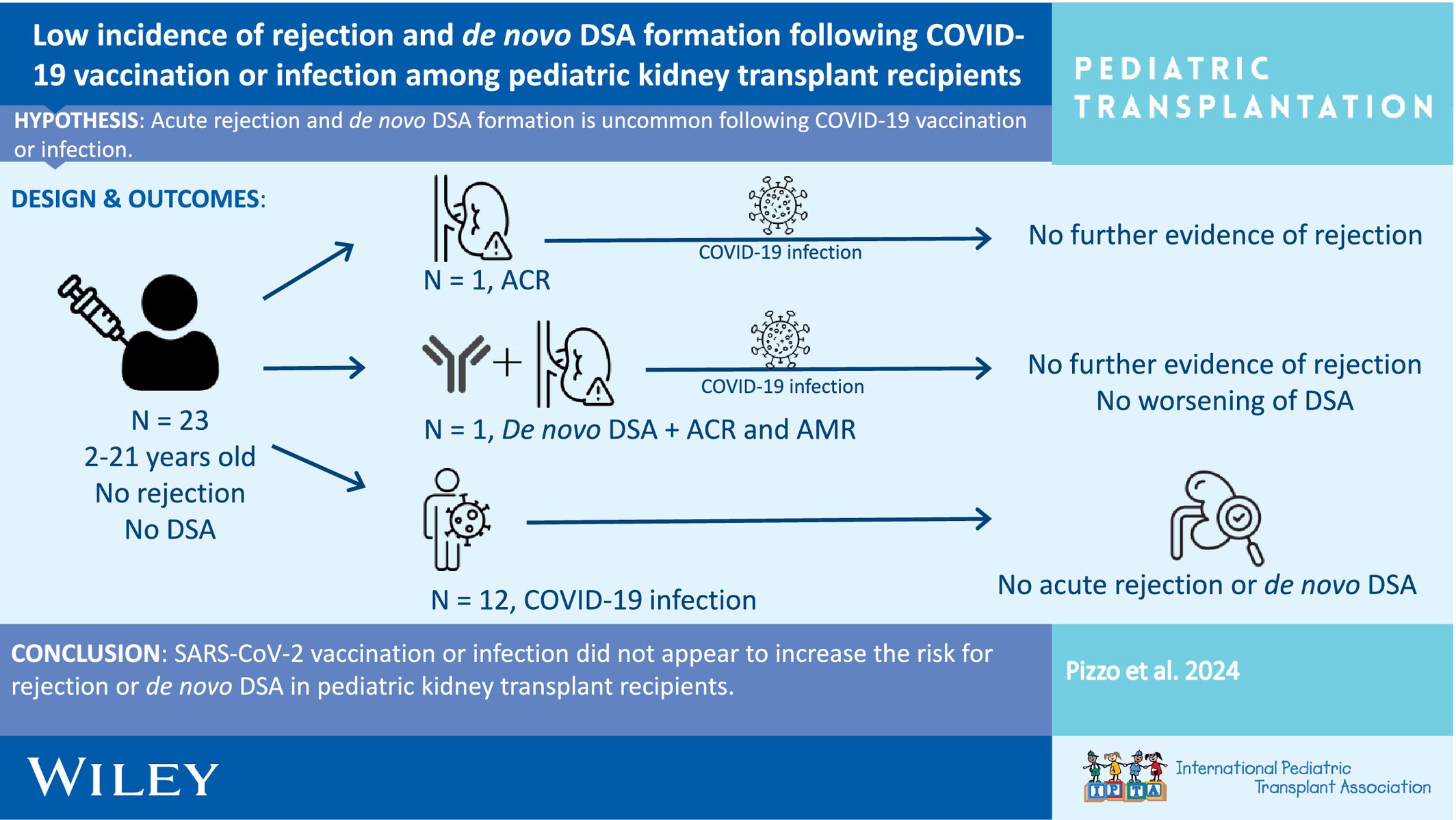
This study investigated the incidence of allograft rejection and de novo donor-specific antibody formation following COVID-19 vaccination or infection among pediatric kidney transplant recipients.
-
Precision Monitoring of Immunosuppressive Agent Concentrations in Cardiac Tissue of Pediatric Heart Transplant Recipientsoa
Graphical Abstract
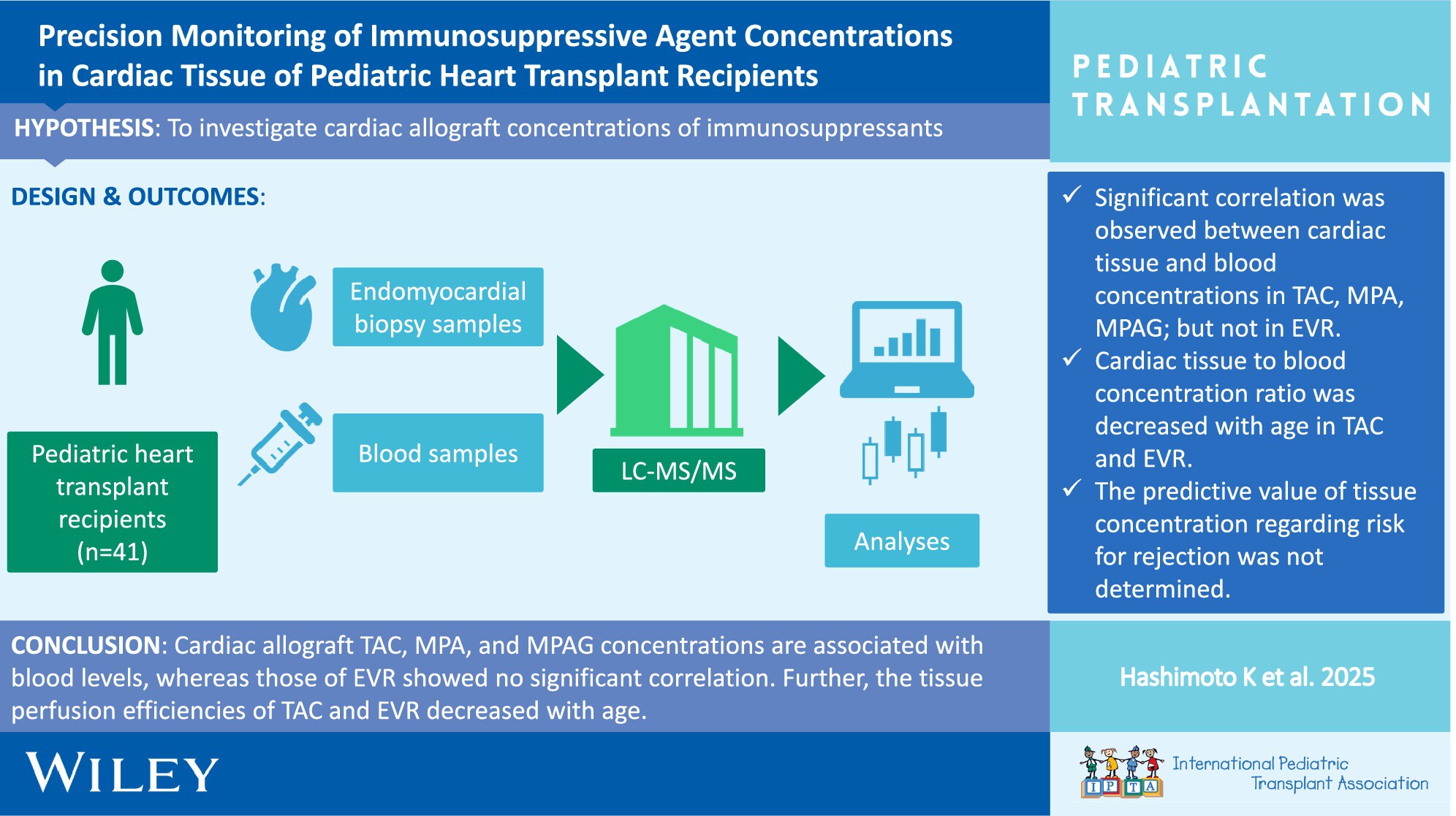
Cardiac allograft tissue concentrations of tacrolimus and mycophenolate acid are correlated with blood levels, whereas those of everolimus showed no correlation. Further, the tissue perfusion efficiencies of tacrolimus and everolimus decreased with age. The relationship between acute cellular rejection and cardiac tissue concentrations could not be elucidated in this study.
-
Frailty in Pediatric Liver Disease May Be Associated With an Increased Incidence of Readmissions After Pediatric Liver Transplantationno
Graphical Abstract

Pretransplant frailty in children is associated with worse post-LT outcomes. Multicenter study included patients who had frailty assessment and then underwent liver transplant. Clinical outcomes were collected up to 1 year post LT. 28 pediatric LT recipients were included, and 15 participants met criteria for frailty. Higher pre-transplant frailty scores were also significantly associated with an increased number of readmissions after transplantation (p = 0.034). Pediatric frailty is associated with increased frequency of hospitalization in the first year after pediatric liver transplantation. These data support the concept that frail children should be identified and targeted for prehabilitation prior to liver transplant.
-
Recurrence of Primary Sclerosing Cholangitis After Pediatric Liver Transplantation: A Single-Center, Retrospective Study in Japanno
Graphical Abstract
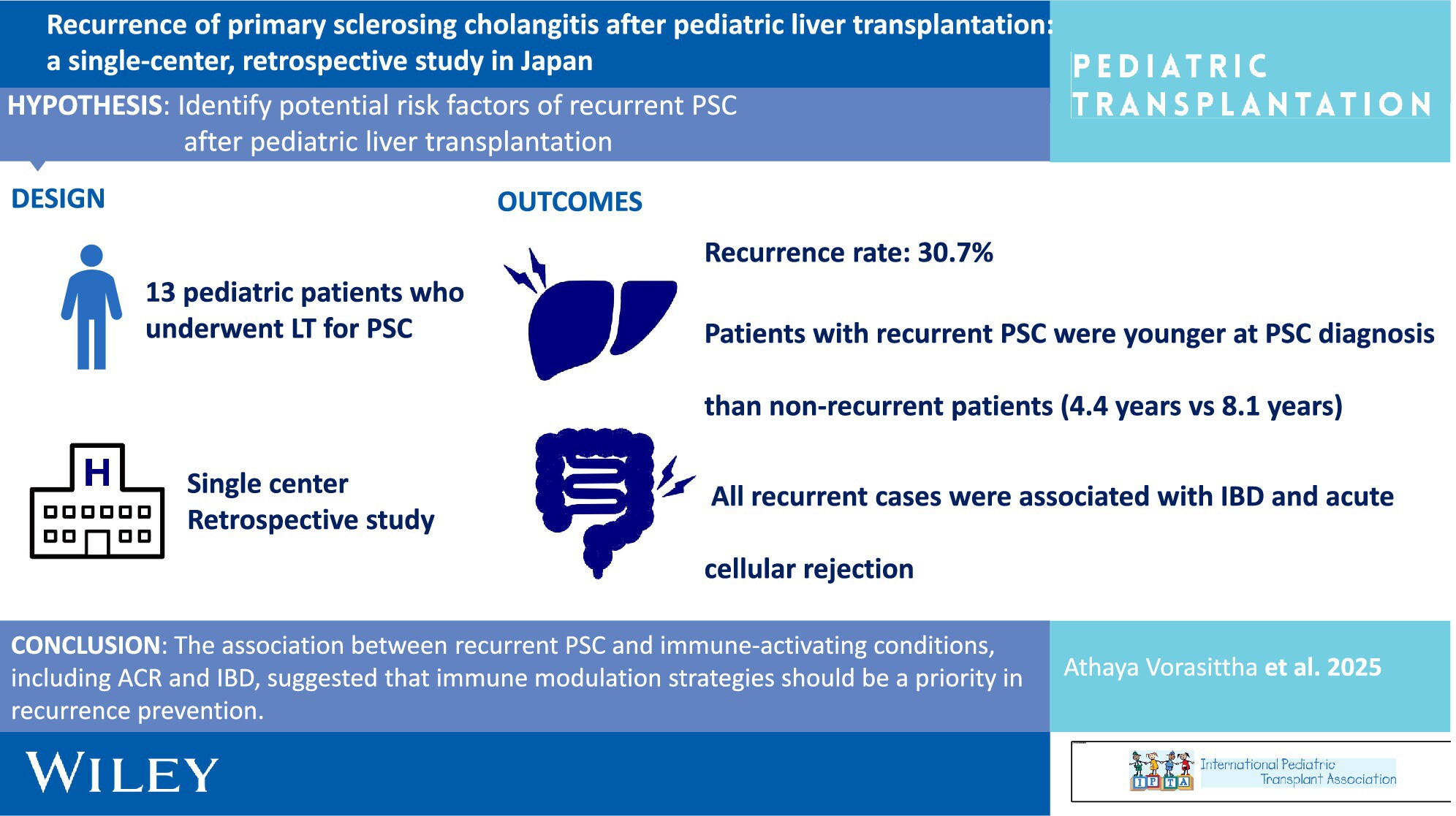
The recurrence rate was high in pediatric patients with PSC, emphasizing the need for tailored management strategies in children. The association between recurrent PSC and immune-activating conditions, including ACR and IBD, suggested that immune modulation strategies should be a priority in recurrence prevention.
-
ABO Incompatible Grafts Are Associated With Excellent Outcomes in Pediatric Liver Transplant Recipients: An Important Resource to Reduce Waitlist Mortalityno
Graphical Abstract
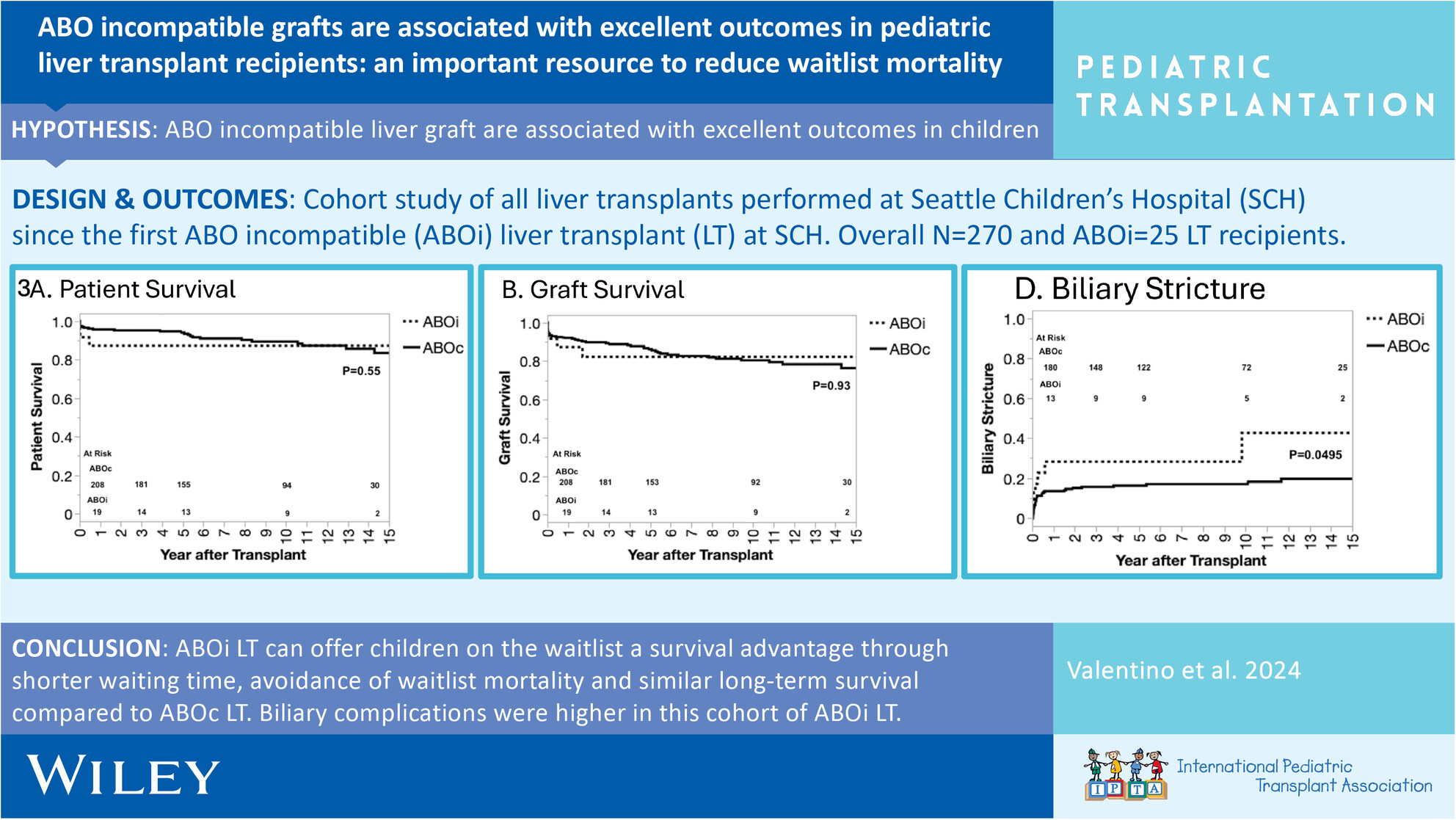
This is a large single-center investigation of pediatric ABO incompatible (ABOi) liver transplants (LT) in the United States demonstrating equivalent survival outcomes following transplantation, when compared to ABO compatible LT, and without an increase in acute rejection or vascular complications. Advocacy efforts are needed in the United States to change allocation policy to expand access to ABOi LT for children on the LT waitlist.
-
Post-Liver Transplantation–Burkitt Lymphoma in Children: A Single-Center Study of Clinical Characteristics, Treatment, and Outcomesno
Graphical Abstract
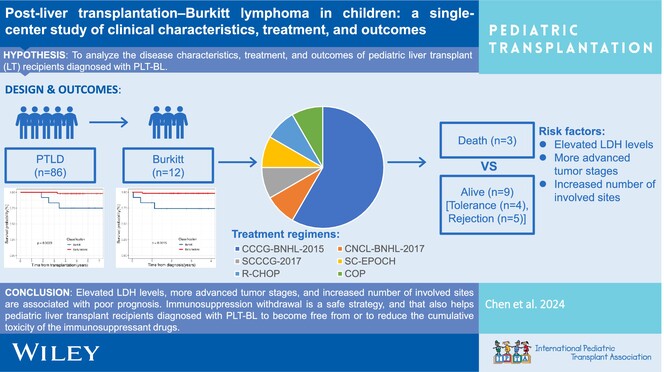
Elevated LDH levels, advanced tumor stages, and increased number of involved sites are associated with poor prognosis in post-liver transplantation–Burkitt lymphoma (PLT-BL). Immunosuppression withdrawal is a safe strategy, and that also helps pediatric LT recipients diagnosed with PLT-BL to become free from or to reduce the cumulative toxicity of the immunosuppressant drugs.
-
Impact of Hepatoblastoma on Infectious Complications Following Pediatric Liver Transplantationoa
Graphical Abstract
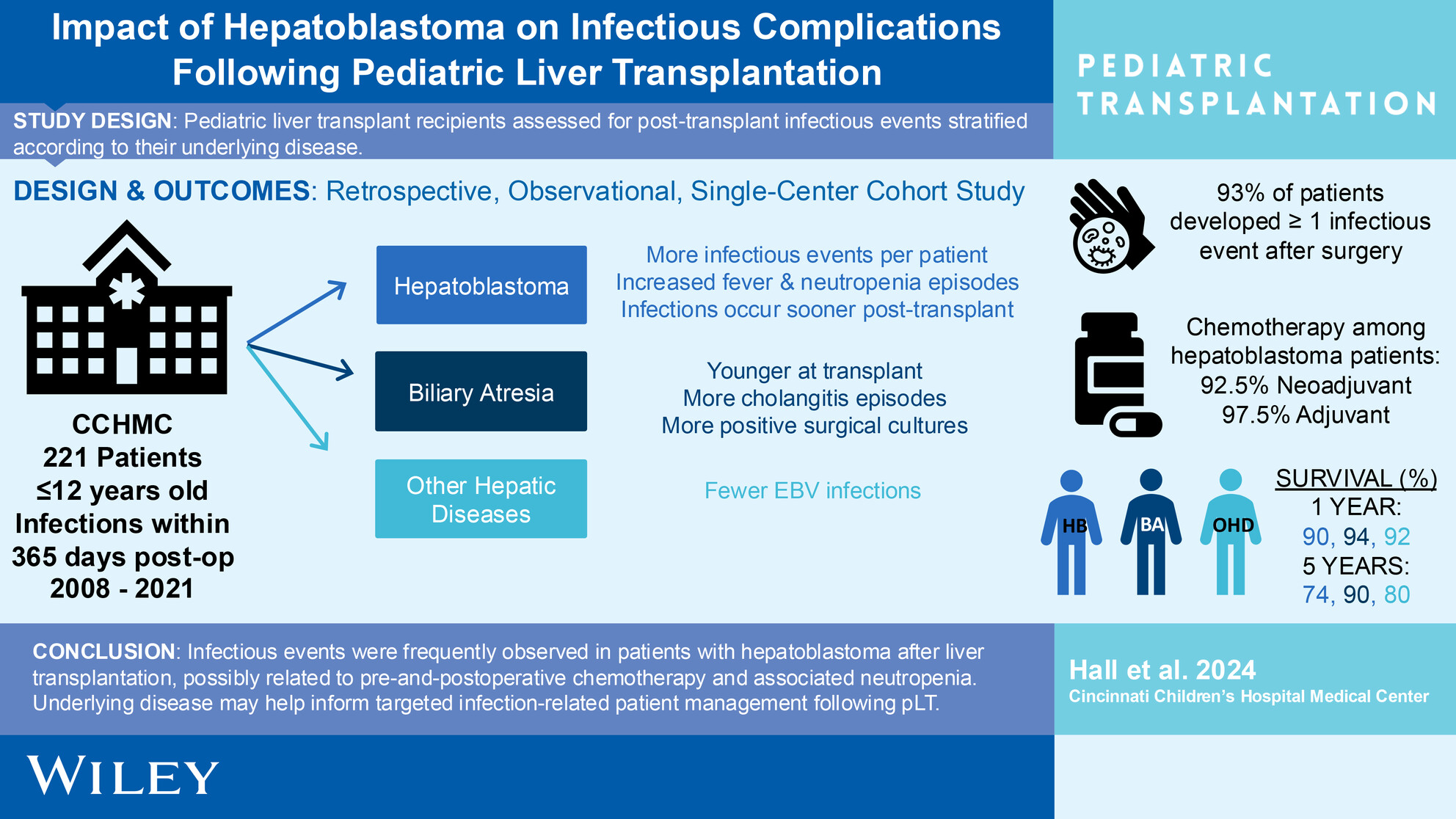
Our single-center retrospective study of pediatric patients following liver transplantation (pLT) found that hepatoblastoma (HB) patients had the most infectious events (IE) per patient and were more likely to develop fever & neutropenia than patients with biliary atresia or other hepatic diseases. Despite this finding, 1-and-5-year survival were not significantly different between patient groups. IE may inform specialized infection-related medical management driven by patients' underlying disease following pLT.