Neuromuscular amyloidosis: Unmasking the master of disguise
Marcus V. Pinto MD, MS
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA
Department of Neurology, Federal University of Rio de Janeiro, National Amyloidosis Referral Center (CEPARM), Rio de Janeiro, Brazil
Search for more papers by this authorP. James B. Dyck MD
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA
Search for more papers by this authorCorresponding Author
Teerin Liewluck MD
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA
Correspondence
Teerin Liewluck, Department of Neurology, 200 First Street SW, Rochester, MN 55905, USA.
Email: [email protected]
Search for more papers by this authorMarcus V. Pinto MD, MS
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA
Department of Neurology, Federal University of Rio de Janeiro, National Amyloidosis Referral Center (CEPARM), Rio de Janeiro, Brazil
Search for more papers by this authorP. James B. Dyck MD
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA
Search for more papers by this authorCorresponding Author
Teerin Liewluck MD
Department of Neurology, Mayo Clinic, Rochester, Minnesota, USA
Correspondence
Teerin Liewluck, Department of Neurology, 200 First Street SW, Rochester, MN 55905, USA.
Email: [email protected]
Search for more papers by this authorAnswer questions and earn CME https://education.aanem.org/URL/JR84.
The objectives of this activity are to: 1) Be able to recognize the symptoms and signs of possible amyloidosis affecting the peripheral nervous system and order appropriate diagnostic testing; 2) Be able to recognize the symptoms and signs of possible amyloidosis affecting skeletal muscle and order appropriate diagnostic testing; 3) Become familiar with and be able to order appropriate testing for the various types of amyloidosis producing neuromuscular disorders.
Abstract
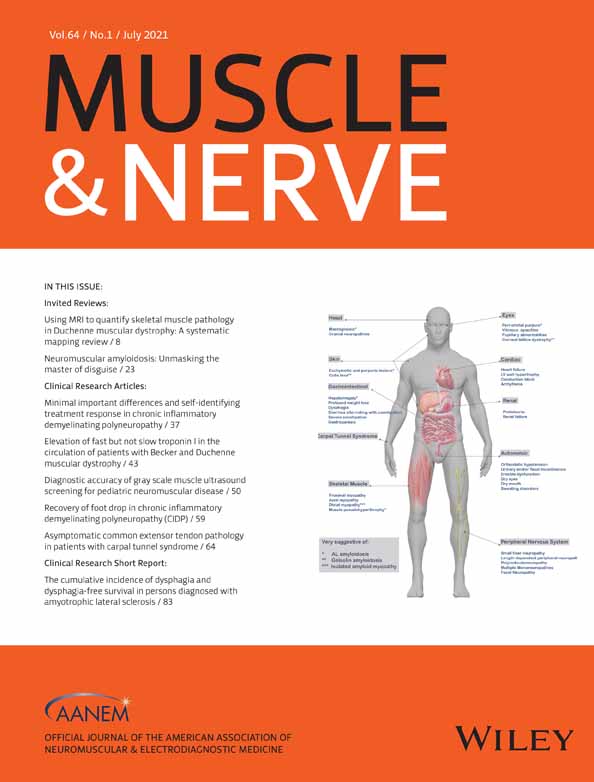
Amyloidosis refers to an etiologically heterogeneous group of protein misfolding diseases, pathologically characterized by extracellular amyloid fibrils producing congophillic amorphous deposits in organs and tissues, which may lead to severe organ dysfunction and mortality. Clinical presentations vary and are often nonspecific, depending on what organs or tissues are affected. In systemic amyloidosis, the peripheral nervous system is commonly affected, whereas the skeletal muscles are only rarely involved. Immunoglobulin light chain (AL) amyloidosis and hereditary transthyretin (ATTRv) amyloidosis are the most frequent types of systemic amyloidosis involving the neuromuscular system. Localized amyloidosis can occur in skeletal muscle, so-called isolated amyloid myopathy. Amyloid neuropathy typically involves small myelinated and unmyelinated sensory and autonomic nerve fibers early in the course of the disease, followed by large myelinated fiber sensory and motor deficits. The relentlessly progressive nature with motor, painful sensory and severe autonomic dysfunction, profound weight loss, and systemic features are distinct characteristics of amyloid neuropathy. Amyloid myopathy presentation differs between systemic amyloidosis and isolated amyloid myopathy. Long-standing symptoms, distal predominant myopathy, markedly elevated creatine kinase level, and lack of peripheral neuropathy or systemic features are highly suggestive of isolated amyloid myopathy. In ATTR and AL amyloidosis, early treatment correlates with favorable outcomes. Therefore, awareness of these disorders and active screening for amyloidosis in patients with neuropathy or myopathy are crucial in detecting these patients in the everyday practice of neuromuscular medicine. Herein, we review the clinical manifestations of neuromuscular amyloidosis and provide a diagnostic approach to this disorder.
Open Research
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article because no datasets were generated as this is a review article.
REFERENCES
- 1Benson MD, Buxbaum JN, Eisenberg DS, et al. Amyloid nomenclature 2018: recommendations by the International Society of Amyloidosis (ISA) nomenclature committee. Amyloid. 2018; 25(4): 215-219.
- 2Vaxman I, Gertz M. When to suspect a diagnosis of amyloidosis. Acta Haematol. 2020; 143: 304-311.
- 3Gertz MA, Dispenzieri A. Systemic amyloidosis recognition, prognosis, and therapy: a systematic review. JAMA. 2020; 324(1): 79-89.
- 4Liewluck T, Milone M. Characterization of isolated amyloid myopathy. Eur J Neurol. 2017; 24(12): 1437-1445.
- 5Pinto MV, Tracy J, Liewluck T. Teaching neuroImages: amyloid myopathy: not your usual suspects. Neurology. 2020; 95: e1290-e1291.
- 6Benson MD, Waddington-Cruz M, Berk JL, et al. Inotersen treatment for patients with hereditary transthyretin amyloidosis. N Engl J Med. 2018; 379(1): 22-31.
- 7Adams D, Gonzalez-Duarte A, O'Riordan WD, et al. Patisiran, an RNAi therapeutic, for hereditary transthyretin amyloidosis. N Engl J Med. 2018; 379(1): 11-21.
- 8Maurer MS, Schwartz JH, Gundapaneni B, et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018; 379(11): 1007-1016.
- 9Cook J, Muchtar E, Warsame R. Updates in the diagnosis and management of AL amyloidosis. Curr Hematol Malig Rep. 2020; 15(3): 155-167.
- 10Reilly MM. Hereditary amyloid neuropathy. In: PJ Dyck, PK Thomas, eds. Peripheral Neuropathy. Vol 2. 4th ed. Amsterdam, The Netherlands: Elsevier; 2005: 1921-1936.
10.1016/B978-0-7216-9491-7.50086-7 Google Scholar
- 11Kaku M, Berk JL. Neuropathy associated with systemic amyloidosis. Semin Neurol. 2019; 39(5): 578-588.
- 12Dyck PJ, Lambert EH. Dissociated sensation in amylidosis. Compound action potential, quantitative histologic and teased-fiber, and electron microscopic studies of sural nerve biopsies. Arch Neurol. 1969; 20(5): 490-507.
- 13Kelly JJ Jr, Kyle RA, O'Brien PC, Dyck PJ. The natural history of peripheral neuropathy in primary systemic amyloidosis. Ann Neurol. 1979; 6(1): 1-7.
- 14Loavenbruck AJ, Singer W, Mauermann ML, et al. Transthyretin amyloid neuropathy has earlier neural involvement but better prognosis than primary amyloid counterpart: an answer to the paradox? Ann Neurol. 2016; 80(3): 401-411.
- 15Pinto MV, Dyck PJB, Gove LE, et al. Kind and distribution of cutaneous sensation loss in hereditary transthyretin amyloidosis with polyneuropathy. J Neurol Sci. 2018; 394: 78-83.
- 16Pinto MV, Barreira AA, Bulle AS, et al. Brazilian consensus for diagnosis, management and treatment of transthyretin familial amyloid polyneuropathy. Arq Neuropsiquiatr. 2018; 76(9): 609-621.
- 17Adams D, Coelho T, Obici L, et al. Rapid progression of familial amyloidotic polyneuropathy: a multinational natural history study. Neurology. 2015; 85(8): 675-682.
- 18Kyle RA, Kelly JJ, Dyck PJ. Amyloidosis and neuropathy. In: PJ Dyck, PK Thomas, eds. Peripheral Neuropathy. Vol 2. 4th ed. Amsterdam, The Netherlands: Elsevier; 2005: 2427-2451.
10.1016/B978-0-7216-9491-7.50111-3 Google Scholar
- 19Chaudhry HM, Mauermann ML, Rajkumar SV. Monoclonal gammopathy-associated peripheral neuropathy: diagnosis and management. Mayo Clin Proc. 2017; 92(5): 838-850.
- 20Tracy JA, Dyck PJ, Dyck PJB. Primary amyloidosis presenting as upper limb multiple mononeuropathies. Muscle Nerve. 2010; 41(5): 710-715.
- 21Briemberg HR, Amato AA. Transthyretin amyloidosis presenting with multifocal demyelinating mononeuropathies. Muscle Nerve. 2004; 29(2): 318-322.
- 22Adams D, Lozeron P, Lacroix C. Amyloid neuropathies. Curr Opin Neurol. 2012; 25(5): 564-572.
- 23Dyck PJB, Tracy JA. History, diagnosis, and management of chronic inflammatory demyelinating polyradiculoneuropathy. Mayo Clin Proc. 2018; 93(6): 777-793.
- 24Mariani LL, Lozeron P, Theaudin M, et al. Genotype-phenotype correlation and course of transthyretin familial amyloid polyneuropathies in France. Ann Neurol. 2015; 78(6): 901-916.
- 25Rajkumar SV, Gertz MA, Kyle RA. Prognosis of patients with primary systemic amyloidosis who present with dominant neuropathy. Am J Med. 1998; 104(3): 232-237.
- 26Allen JA. Chronic demyelinating polyneuropathies. Continuum (Minneap Minn). 2017; 23(5): 1310-1331.
- 27Cruz MW, Pinto MV, Pinto LF, et al. Baseline disease characteristics in Brazilian patients enrolled in Transthyretin Amyloidosis Outcome Survey (THAOS). Arq Neuropsiquiatr. 2019; 77(2): 96-100.
- 28Figueroa JJ, Dyck PJ, Laughlin RS, et al. Autonomic dysfunction in chronic inflammatory demyelinating polyradiculoneuropathy. Neurology. 2012; 78(10): 702-708.
- 29Karam C, Dimitrova D, Heitner SB. Misdiagnosis of hATTR amyloidosis: a single US site experience. Amyloid. 2020; 27(1): 69-70.
- 30Descamps E, Henry J, Labeyrie C, et al. Small fiber neuropathy in Sjögren syndrome: comparison with other small fiber neuropathies. Muscle Nerve. 2020; 61(4): 515-520.
- 31Waddington-Cruz M, Schmidt H, Botteman MF, et al. Epidemiological and clinical characteristics of symptomatic hereditary transthyretin amyloid polyneuropathy: a global case series. Orphanet J Rare Dis. 2019; 14(1): 34.
- 32Wang AK, Fealey RD, Gehrking TL, Low PA. Patterns of neuropathy and autonomic failure in patients with amyloidosis. Mayo Clin Proc. 2008; 83(11): 1226-1230.
- 33Ebert EC, Nagar M. Gastrointestinal manifestations of amyloidosis. Am J Gastroenterol. 2008; 103(3): 776-787.
- 34Casad DE, Bocian JJ. Primary systemic amyloidosis simulating acute idiopathic ulcerative colitis. Am J Dig Dis. 1965; 10(1): 63-74.
- 35Mian N, DeVito B, Lee T-P, Bernstein D. Gastrointestinal amyloidosis presenting as irritable bowel syndrome: 565. Am J Gastroenterol. 2006; 101:S235.
- 36Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011; 21(2): 69-72.
- 37Cheshire WPJ. Autonomic history, examination, and laboratory evaluation. Continuum (Minneap Minn). 2020; 26(1): 25-43.
- 38Palma JA, Gonzalez-Duarte A, Kaufmann H. Orthostatic hypotension in hereditary transthyretin amyloidosis: epidemiology, diagnosis and management. Clin Auton Res. 2019; 29(Suppl 1): 33-44.
- 39Norcliffe-Kaufmann L, Kaufmann H, Palma J-A, et al. Orthostatic heart rate changes in patients with autonomic failure caused by neurodegenerative synucleinopathies. Ann Neurol. 2018; 83(3): 522-531.
- 40Dixon DD, Muldowney JAS 3rd. Management of neurogenic orthostatic hypotension in the heart failure patient. Auton Neurosci. 2020; 227: 102691.
- 41Low PA. Composite autonomic scoring scale for laboratory quantification of generalized autonomic failure. Mayo Clin Proc. 1993; 68(8): 748-752.
- 42Low PA. Testing the autonomic nervous system. Semin Neurol. 2003; 23(4): 407-421.
- 43Dingli D, Tan TS, Kumar SK, et al. Stem cell transplantation in patients with autonomic neuropathy due to primary (AL) amyloidosis. Neurology. 2010; 74(11): 913-918.
- 44Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol. 1995; 32(1): 45-59.
- 45Karam C, Dimitrova D, Christ M, Heitner SB. Carpal tunnel syndrome and associated symptoms as first manifestation of hATTR amyloidosis. Neurol Clin Pract. 2019; 9(4): 309-313.
- 46Pinney JH, Whelan CJ, Petrie A, et al. Senile systemic amyloidosis: clinical features at presentation and outcome. J Am Heart Assoc. 2013; 2(2):e000098.
- 47Hornigold R, Patel AV, Ward VM, O'Connor AF. Familial systemic amyloidosis associated with bilateral sensorineural hearing loss and bilateral facial palsies. J Laryngol Otol. 2006; 120(9): 778-780.
- 48Kapoor M, Rossor AM, Jaunmuktane Z, Lunn MPT, Reilly MM. Diagnosis of amyloid neuropathy. Pract Neurol. 2019; 19(3): 250-258.
- 49Sperry BW, Reyes BA, Ikram A, et al. Tenosynovial and cardiac amyloidosis in patients undergoing carpal tunnel release. J Am Coll Cardiol. 2018; 72(17): 2040-2050.
- 50McKechnie S, Yang F, Harper CG, et al. Amyloidoma of a spinal root. Neurology. 2003; 61(6): 834-836.
- 51Haridas A, Basu S, King A, Pollock J. Primary isolated amyloidoma of the lumbar spine causing neurological compromise: case report and literature review. Neurosurgery. 2005; 57(1): E196-E196.
- 52Ladha SS, Dyck PJ, Spinner RJ, et al. Isolated amyloidosis presenting with lumbosacral radiculoplexopathy: description of two cases and pathogenic review. J Peripher Nerv Syst. 2006; 11(4): 346-352.
- 53Loavenbruck AJ, Chaudhry V, Zeldenrust SR, Spinner RJ, Theis JD, Klein CJ. Mass spectrometry analysis reveals non-mutated apolipoprotein A1 lumbosacral radiculoplexus amyloidoma. Muscle Nerve. 2012; 46(5): 817-822.
- 54Cheng RR, Eskandari R, Welsh CT, Varma AK. A case of isolated amyloid light-chain amyloidosis of the radial nerve. J Neurosurg. 2016; 125(3): 598-602.
- 55Pihlamaa T, Salmi T, Suominen S, Kiuru-Enari S. Progressive cranial nerve involvement and grading of facial paralysis in gelsolin amyloidosis. Muscle Nerve. 2016; 53(5): 762-769.
- 56Traynor AE, Gertz MA, Kyle RA. Cranial neuropathy associated with primary amyloidosis. Ann Neurol. 1991; 29(4): 451-454.
- 57Muchtar E, Derudas D, Mauermann M, et al. Systemic immunoglobulin light chain amyloidosis-associated myopathy: presentation, diagnostic pitfalls, and outcome. Mayo Clin Proc. 2016; 91(10): 1354-1361.
- 58Pinto MV, Milone M, Mauermann ML, et al. Transthyretin amyloidosis: putting myopathy on the map. Muscle Nerve. 2020; 61(1): 95-100.
- 59Yamashita T, Ando Y, Katsuragi S, et al. Muscular amyloid angiopathy with amyloidgenic transthyretin Ser50Ile and Tyr114Cys. Muscle Nerve. 2005; 31(1): 41-45.
- 60Carr AS, Pelayo-Negro AL, Jaunmuktane Z, et al. Transthyretin V122I amyloidosis with clinical and histological evidence of amyloid neuropathy and myopathy. Neuromuscul Disord. 2015; 25(6): 511-515.
- 61Misumi Y, Doki T, Ueda M, et al. Myopathic phenotype of familial amyloid polyneuropathy with a rare transthyretin variant: ATTR Ala45Asp. Amyloid. 2014; 21(3): 216-217.
- 62Prayson RA. Amyloid myopathy: clinicopathologic study of 16 cases. Hum Pathol. 1998; 29(5): 463-468.
- 63Patel K, Tagoe C, Bieri P, Weidenheim K, Tauras JM. γ. Amyloid. 2018; 25: 211-212.
- 64Rezania K, Pytel P, Smit LJ, et al. Systemic transthyretin amyloidosis in a patient with bent spine syndrome. Amyloid. 2013; 20(2): 131-134.
- 65Huser S, Loavenbruck A, Manousakis G. Wild-type transthyretin amyloid myopathy with an inclusion body myositis phenotype. J Clin Neuromuscul Dis. 2020; 22(1): 53-57.
- 66Gertz MA, Kyle RA, Griffing WL, Hunder GG. Jaw claudication in primary systemic amyloidosis. Medicine. 1986; 65(3): 173-179.
- 67Delcey V, Hachulla E, Michon-Pasturel U, et al. [Camptocormia: a sign of axial myopathy. Report of 7 cases]. Rev Med Interne. 2002; 23(2): 144-154.
- 68Triplett JD, Pinto MV, Hosfield EA, Milone M, Liewluck T. Myopathies featuring early or prominent dysphagia. Muscle Nerve. 2020; 62(3): 344-350.
- 69Ghosh PS, Thaera GM, Tracy JA. Teaching neuroimages: dyspnea as a presenting manifestation of amyloid myopathy. Neurology. 2013; 81(24):e184.
- 70Spuler S, Emslie-Smith A, Engel AG. Amyloid myopathy: an underdiagnosed entity. Ann Neurol. 1998; 43(6): 719-728.
- 71Liewluck T, Milone M. Untangling the complexity of limb-girdle muscular dystrophies. Muscle Nerve. 2018; 58(2): 167-177.
- 72Spuler S, Carl M, Zabojszcza J, et al. Dysferlin-deficient muscular dystrophy features amyloidosis. Ann Neurol. 2008; 63(3): 323-328.
- 73Liewluck T, Winder TL, Dimberg EL, et al. ANO5-muscular dystrophy: clinical, pathological and molecular findings. Eur J Neurol. 2013; 20(10): 1383-1389.
- 74Rosales XQ, Gastier-Foster JM, Lewis S, et al. Novel diagnostic features of dysferlinopathies. Muscle Nerve. 2010; 42(1): 14-21.
- 75Anandan C, Milone M, Liewluck T. Intramuscular interstitial amyloid deposition does not impact anoctaminopathy-5 phenotype. Muscle Nerve. 2019; 59(1): 133-137.
- 76Gertz MA. Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment. Am J Hematol. 2020; 95(7): 848-860.
- 77Solomon JP, Page LJ, Balch WE, Kelly JW. Gelsolin amyloidosis: genetics, biochemistry, pathology and possible strategies for therapeutic intervention. Crit Rev Biochem Mol Biol. 2012; 47(3): 282-296.
- 78Meretoja J. Genetic aspects of familial amyloidosis with corneal lattice dystrophy and cranial neuropathy. Clin Genet. 1973; 4(3): 173-185.
- 79Kiuru-Enari S, Keski-Oja J, Haltia M. Cutis laxa in hereditary gelsolin amyloidosis. Br J Dermatol. 2005; 152(2): 250-257.
- 80Reynolds MM, Veverka KK, Gertz MA, et al. Ocular manifestations of familial transthyretin amyloidosis. Am J Ophthalmol. 2017; 183: 156-162.
- 81Reynolds MM, Veverka KK, Gertz MA, et al. Ocular manifestations of systemic amyloidosis. Retina. 2018; 38(7): 1371-1376.
- 82Tanskanen M, Peuralinna T, Polvikoski T, et al. Senile systemic amyloidosis affects 25% of the very aged and associates with genetic variation in alpha2-macroglobulin and tau: a population-based autopsy study. Ann Med. 2008; 40(3): 232-239.
- 83Martinez-Naharro A, Baksi AJ, Hawkins PN, Fontana M. Diagnostic imaging of cardiac amyloidosis. Nat Rev Cardiol. 2020; 17(7): 413-426.
- 84Witteles RM, Bokhari S, Damy T, et al. Screening for transthyretin amyloid cardiomyopathy in everyday practice. JACC Heart Fail. 2019; 7(8): 709-716.
- 85Pagourelias ED, Mirea O, Duchenne J, et al. Echo parameters for differential diagnosis in cardiac amyloidosis: a head-to-head comparison of deformation and nondeformation parameters. Circ Cardiovasc Imaging. 2017; 10(3):e005588.
- 86Vogelsberg H, Mahrholdt H, Deluigi CC, et al. Cardiovascular magnetic resonance in clinically suspected cardiac amyloidosis: noninvasive imaging compared to endomyocardial biopsy. J Am Coll Cardiol. 2008; 51(10): 1022-1030.
- 87Gillmore Julian D, Maurer Mathew S, Falk Rodney H, et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016; 133(24): 2404-2412.
- 88Musumeci MB, Cappelli F, Russo D, et al. Low sensitivity of bone scintigraphy in detecting Phe64Leu mutation-related transthyretin cardiac amyloidosis. J Am Coll Cardiol Img. 2020; 13(6): 1314-1321.
- 89Rapezzi C, Merlini G, Quarta CC, et al. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation. 2009; 120(13): 1203-1212.
- 90Gillmore JD, Damy T, Fontana M, et al. A new staging system for cardiac transthyretin amyloidosis. Eur Heart J. 2017; 39(30): 2799-2806.
- 91Go RS, Rajkumar SV. How I manage monoclonal gammopathy of undetermined significance. Blood. 2018; 131(2): 163-173.
- 92Kyle RA, Therneau TM, Rajkumar SV, et al. Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med. 2006; 354(13): 1362-1369.
- 93Rajkumar SV, Kyle RA, Therneau TM, et al. Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance. Blood. 2005; 106(3): 812-817.
- 94Kyle RA, Larson DR, Therneau TM, et al. Long-term follow-up of monoclonal gammopathy of undetermined significance. N Engl J Med. 2018; 378(3): 241-249.
- 95Phull P, Sanchorawala V, Connors LH, et al. Monoclonal gammopathy of undetermined significance in systemic transthyretin amyloidosis (ATTR). Amyloid. 2018; 25(1): 62-67.
- 96Vrana JA, Gamez JD, Madden BJ, Theis JD, Bergen HR 3rd, Dogan A. Classification of amyloidosis by laser microdissection and mass spectrometry-based proteomic analysis in clinical biopsy specimens. Blood. 2009; 114(24): 4957-4959.
- 97Vrana JA, Theis JD, Dasari S, et al. Clinical diagnosis and typing of systemic amyloidosis in subcutaneous fat aspirates by mass spectrometry-based proteomics. Haematologica. 2014; 99(7): 1239-1247.
- 98Klein CJ, Vrana JA, Theis JD, et al. Mass spectrometric–based proteomic analysis of amyloid neuropathy type in nerve tissue. Arch Neurol. 2011; 68(2): 195-199.
- 99Dasari S, Theis JD, Vrana JA, et al. Clinical proteome informatics workbench detects pathogenic mutations in hereditary amyloidoses. J Proteome Res. 2014; 13(5): 2352-2358.
- 100Dasari S, Theis JD, Vrana JA, et al. Amyloid typing by mass spectrometry in clinical practice: a comprehensive review of 16,175 samples. Mayo Clin Proc. 2020; 95(9): 1852-1864.
- 101Koike H, Hashimoto R, Tomita M, et al. Diagnosis of sporadic transthyretin Val30Met familial amyloid polyneuropathy: a practical analysis. Amyloid. 2011; 18(2): 53-62.
- 102Shouman K, Broski SM, Muchtar E, et al. Novel imaging techniques using (18) F-Florbetapir PET/MRI can guide fascicular nerve biopsy in amyloid multiple Mononeuropathy. Muscle Nerve. 2021; 63: 104-108.
- 103Vogt B, Chahin N, Wiszniewski W, Ragole T, Karam C. Screening for genetic mutations in patients with neuropathy without definite etiology is useful. J Neurol. 2020; 267(9): 2648-2654.
- 104Kyle RA, Larson DR, Kurtin PJ, et al. Incidence of AL amyloidosis in Olmsted County, Minnesota, 1990 through 2015. Mayo Clin Proc. 2019; 94(3): 465-471.
- 105Kyle RA, Bayrd ED. Amyloidosis: review of 236 cases. Medicine. 1975; 54(4): 271-299.
- 106Muchtar E, Gertz MA, Kyle RA, et al. A modern primer on light chain amyloidosis in 592 patients with mass spectrometry-verified typing. Mayo Clin Proc. 2019; 94(3): 472-483.
- 107Duston MA, Skinner M, Anderson J, Cohen AS. Peripheral neuropathy as an early marker of AL amyloidosis. Arch Intern Med. 1989; 149(2): 358-360.
- 108Lousada I, Comenzo RL, Landau H, Guthrie S, Merlini G. Light chain amyloidosis: patient experience survey from the amyloidosis research consortium. Adv Ther. 2015; 32(10): 920-928.
- 109Muchtar E, Dispenzieri A, Lacy MQ, et al. Overuse of organ biopsies in immunoglobulin light chain amyloidosis (AL): the consequence of failure of early recognition. Ann Med. 2017; 49(7): 545-551.
- 110Quarta CC, Gonzalez-Lopez E, Gilbertson JA, et al. Diagnostic sensitivity of abdominal fat aspiration in cardiac amyloidosis. Eur Heart J. 2017; 38(24): 1905-1908.
- 111Kimmich C, Schönland S, Kräker S, et al. Amyloid in bone marrow smears in systemic light-chain amyloidosis. Amyloid. 2017; 24(1): 52-59.
- 112Muchtar E, Gertz MA, Kumar SK, et al. Improved outcomes for newly diagnosed AL amyloidosis between 2000 and 2014: cracking the glass ceiling of early death. Blood. 2017; 129(15): 2111-2119.
- 113Pinto MV, Shelly S, Low P, et al. Autologous stem cell transplantation may halt peripheral neuropathy progression and improve survival in immunoglobulin light chain amyloid neuropathy. J Peripher Nerv Syst. 2020; 25; 2020 Peripheral Nerve Society Virtual Event: poster 1328.
- 114Inês M, Coelho T, Conceição I, Duarte-Ramos F, de Carvalho M, Costa J. Epidemiology of transthyretin familial amyloid polyneuropathy in Portugal: a nationwide study. Neuroepidemiology. 2018; 51(3–4): 177-182.
- 115Sekijima Y. Transthyretin (ATTR) amyloidosis: clinical spectrum, molecular pathogenesis and disease-modifying treatments. J Neurol Neurosurg Psychiatry. 2015; 86(9): 1036-1043.
- 116Adams D, Koike H, Slama M, Coelho T. Hereditary transthyretin amyloidosis: a model of medical progress for a fatal disease. Nat Rev Neurol. 2019; 15(7): 387-404.
- 117Swiecicki PL, Zhen DB, Mauermann ML, et al. Hereditary ATTR amyloidosis: a single-institution experience with 266 patients. Amyloid. 2015; 22(2): 123-131.
- 118Buxbaum JN, Ruberg FL. Transthyretin V122I (pV142I)* cardiac amyloidosis: an age-dependent autosomal dominant cardiomyopathy too common to be overlooked as a cause of significant heart disease in elderly African Americans. Genet Med. 2017; 19(7): 733-742.
- 119Buxbaum J, Jacobson DR, Tagoe C, et al. Transthyretin V122I in African Americans with congestive heart failure. J Am Coll Cardiol. 2006; 47(8): 1724-1725.
- 120Andrade C. A peculiar form of peripheral neuropathy; familiar atypical generalized amyloidosis with special involvement of the peripheral nerves. Brain. 1952; 75(3): 408-427.
- 121Ikeda S, Hanyu N, Hongo M, et al. Hereditary generalized amyloidosis with polyneuropathy. Clinicopathological study of 65 Japanese patients. Brain. 1987; 110(Pt 2): 315-337.
- 122Koike H, Misu K, Ikeda S, et al. Type I (transthyretin Met30) familial amyloid polyneuropathy in Japan: early- vs late-onset form. Arch Neurol. 2002; 59(11): 1771-1776.
- 123Pinto MV, Pinto LF, Dias M, et al. Late-onset hereditary ATTR V30M amyloidosis with polyneuropathy: characterization of Brazilian subjects from the THAOS registry. J Neurol Sci. 2019; 403: 1-6.
- 124Do Amaral B, Coelho T, Sousa A, Guimaraes A. Usefulness of labial salivary gland biopsy in familial amyloid polyneuropathy Portuguese type. Amyloid. 2009; 16(4): 232-238.
- 125de Paula Eduardo F, de Mello Bezinelli L, de Carvalho DL, et al. Minor salivary gland biopsy for the diagnosis of familial amyloid polyneuropathy. Neurol Sci. 2017; 38(2): 311-318.
- 126Ebenezer GJ, Liu Y, Judge DP, et al. Cutaneous nerve biomarkers in transthyretin familial amyloid polyneuropathy. Ann Neurol. 2017; 82(1): 44-56.
- 127Holmgren G, Steen L, Ekstedt J, et al. Biochemical effect of liver transplantation in two Swedish patients with familial amyloidotic polyneuropathy (FAP-met30). Clin Genet. 1991; 40(3): 242-246.
- 128Carvalho A, Rocha A, Lobato L. Liver transplantation in transthyretin amyloidosis: issues and challenges. Liver Transpl. 2015; 21(3): 282-292.
- 129Suhr OB, Holmgren G, Steen L, et al. Liver transplantation in familial amyloidotic polyneuropathy. Follow-up of the first 20 Swedish patients. Transplantation. 1995; 60(9): 933-938.
- 130Ericzon BG, Wilczek HE, Larsson M, et al. Liver transplantation for hereditary transthyretin amyloidosis: after 20 years still the best therapeutic alternative? Transplantation. 2015; 99(9): 1847-1854.
- 131Yazaki M, Mitsuhashi S, Tokuda T, et al. Progressive wild-type transthyretin deposition after liver transplantation preferentially occurs onto myocardium in FAP patients. Am J Transplant. 2007; 7(1): 235-242.
- 132Oshima T, Kawahara S, Ueda M, et al. Changes in pathological and biochemical findings of systemic tissue sites in familial amyloid polyneuropathy more than 10 years after liver transplantation. J Neurol Neurosurg Psychiatry. 2014; 85(7): 740-746.
- 133Misumi Y, Ueda M, Masuda T, et al. Characteristics of acquired transthyretin amyloidosis: a case series and review of the literature. Neurology. 2019; 93(17): e1587-e1596.
- 134Puffer RC, Spinner RJ, Bi H, et al. Fatal TTR amyloidosis with neuropathy from domino liver p.Val71Ala transplant. Neurol Genet. 2019; 5(5): e351.
- 135Coelho T, Maia LF, Martins da Silva A, et al. Tafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trial. Neurology. 2012; 79(8): 785-792.
- 136Waddington Cruz M, Benson MD. A review of tafamidis for the treatment of transthyretin-related amyloidosis. Neurol Ther. 2015; 4(2): 61-79.
- 137Berk JL, Suhr OB, Obici L, et al. Repurposing diflunisal for familial amyloid polyneuropathy: a randomized clinical trial. JAMA. 2013; 310(24): 2658-2667.
- 138Moshe-Lilie O, Dimitrova D, Heitner SB, et al. TTR gene silencing therapy in post liver transplant hereditary ATTR amyloidosis patients. Amyloid. 2020; 27(4): 250-253.
- 139Geller HI, Singh A, Alexander KM, Mirto TM, Falk RH. Association between ruptured distal biceps tendon and wild-type transthyretin cardiac amyloidosis. JAMA. 2017; 318(10): 962-963.
- 140Yungher FW, Kim A, Boehme A, et al. Peripheral neuropathy symptoms in wild type transthyretin amyloidosis. J Peripher Nerv Syst. 2020; 25(3): 265-272.
- 141Hutt DF, Quigley A-M, Page J, et al. Utility and limitations of 3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy in systemic amyloidosis. Eur Heart J Cardiovasc Imaging. 2014; 15(11): 1289-1298.
- 142Meretoja J. Familial systemic paramyloidosis with lattice dystrophy of the cornea, progressive cranial neuropathy, skin changes and various internal symptoms. A previously unrecognized heritable syndrome. Ann Clin Res. 1969; 1(4): 314-324.
- 143Kiuru S. Gelsolin-related familial amyloidosis, Finnish type (FAF), and its variants found worldwide. Amyloid. 1998; 5(1): 55-66.
- 144Kiuru-Enari S, Haltia M. Hereditary gelsolin amyloidosis. Handb Clin Neurol. 2013; 115: 659-681.
- 145Kiuru S, Matikainen E, Kupari M, Haltia M, Palo J. Autonomic nervous system and cardiac involvement in familial amyloidosis, Finnish type (FAF). J Neurol Sci. 1994; 126(1): 40-48.
- 146Kiuru S, Salonen O, Haltia M. Gelsolin-related spinal and cerebral amyloid angiopathy. Ann Neurol. 1999; 45(3): 305-311.
Citing Literature