A case of concentrated growth factor gel to fill the defect after large jaw cyst enucleation
Key Clinical Message
Management of large jaw cyst is challenging since high risks including pathologic fracture, limited opening, and insufficient bone healing occur after enucleation. The current case of concentrated growth factor (CGF) gel to fill defect after enucleation of large jaw cyst is rare. A 12-year-old boy with pain and swelling for 4 months in the left mandible region made a medical consultation at our hospital. Computerized tomography scan indicated that cystic lesion was found in the left mandible region. In this case, we present a patient with large jaw cyst (31 mm × 44 mm × 53 mm) who received enucleation followed by CGF gel filling the defect. The patient was discharged after 13 days without discomfort symptoms. The lesion size was reduced significantly at 1-month re-examination. No abnormality was detected in maxillofacial region at 1-year re-examination. Application of CGF gel is one of the possible options for filling defect after jaw cyst enucleation.
1 INTRODUCTION
As one of the most common diseases in oral and maxillofacial surgery, jaw cyst can be divided into odontogenic cyst and nonodontogenic cyst according to different focal areas of the cyst.1 At present, odontogenic cyst accounts for the majority of jaw cyst cases, and the lesions can occur at any jaw location without obvious clinical symptoms in the early stage.2, 3 However, with the development of cyst, bone resorption was observed in the affected area. Besides, swelling in the buccal region, jaw dysfunction, and pathological bone fracture could be diagnosed in several patients. Although conventional surgical treatment with enucleation is widely applied in these clinical settings, the outcome of larger defects by simple enucleation was not satisfactory because of high risk of wound infection.4, 5 Autogenous bone grafting was considered as the priority for reconstructing larger bony defects due to osteoconductive, osteoinductive, and little immunogenic properties.6 Limited bone quantity was the biggest disadvantage for grafting especially for several donor sites. Therefore, active bone regeneration materials were used to prevent infection and improve bone strength.7 The FDA has approved the use of growth factors in dentistry because growth factors have great capabilities to stimulate bone formation in various clinical and experimental settings.8
Concentrated growth factor (CGF) is regarded as a novel blood extraction, which have various growth factors, platelets, and fibrins to induce cell proliferation, periodontal regeneration, and skin wound healing process.9, 10 CGF is prepared from autologous venous blood by specific centrifugation program and takes the form of gel in clinical practice.11 The ultramicrostructure of CGF gel with three-dimensional model consisting of fibrin and growth factors enables malleable feature, which has great application potentials in many clinical scenarios including pulp regeneration, skin wound healing, and bone reconstruction.9, 12, 13 Mounting evidences demonstrate that CGF might be effective in filling defects after jaw cyst enucleation.
The aim of this study is to present a clinical case report of male patient with large jaw cyst treated with enucleation, followed by filling with CGF gel.
2 CASE PRESENTATION
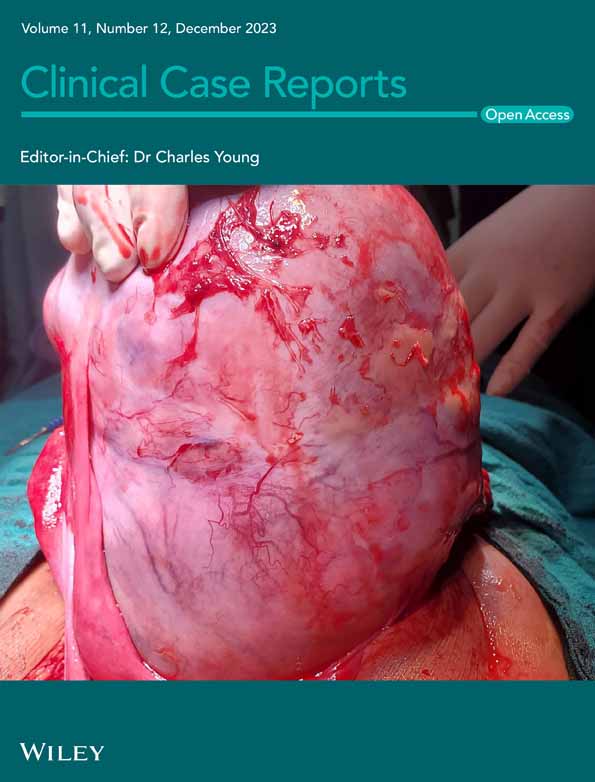
A 12-year-old male patient with pain and swelling in the left mandible region presented to the Department of Burn and Plastic Surgery, Shenzhen Longhua District Central Hospital for excision (Figure 1A,B). The patient family and social history was unremarkable. Physical examinations did not display any significant abnormalities with the body temperature of 36.8°C, the blood pressure of 126/77 mmHg, and the pulse of 95 beats per minute. The routine blood test was also carried out upon admission, and the results were as follows: white blood cell count of 6.1 × 109/L, red blood cell count of 5.32 × 1012/L, hemoglobin of 152 g/L, thrombocytes of 338 × 109/L, neutrophilic granulocyte percentage of 47.7%, lymphocyte percentage of 37.4%, monocyte percentage of 14.2%, and basophilic granulocyte percentage of 0.7%. The results of coagulation action test were as follows: thrombin time of 17.7 s, prothrombin time of 10.4 s, activated partial thromboplastin time of 31.0 s, fibrinogen of 3.18 g/L, and international normalized ratio of 0.9. Three-dimensional reconstruction of computed tomography (CT) scan revealed left lower jaw swelling and thinner cortical bone thickness (Figure 1C–E). The lesion size was 31 mm × 44 mm × 53 mm. No soft tissue mass was observed. The final diagnosis was odontogenic cyst with chronic suppurative inflammation.

The patient received surgical treatment of conventional jaw cyst enucleation following with autologous CGF gel filling on the third day of admission. Written consent form was obtained from the patient's guardian, and all surgical procedures were conducted under general anesthesia according to the policy of Guangdong Medical University. The planned surgical procedures involve thorough disinfection, complete removal of pathological tissue, and filling the defect with CGF gel (Figure 2A). CGF gel was prepared immediately before surgery from patient's blood sample (total volume 90 mL), which was distributed into nine sterile centrifuge tubes (10 mL) without chemical additives (Figure 2B,C). The pathological tissue was sent for further immunohistochemical examination, which indicated that fibrocystic tissue was lined with squamous epithelium, along with serous inflammatory cells infiltration and bone trabecula (Figure 1F). The patient was instructed to hygienic dietary regimen to facilitate recovery after surgery and was discharged with complete resolution of symptoms on 28th July, 2020, 13 days after admission.

One month later, the patient had follow-up examination, which revealed that the lesion area significantly shrinked compared with that diagnosed on admission (Figure 3A–C). The patient received examination at 1-year postsurgical follow-up, and CT scan indicated no appreciable abnormalities were discovered (Figure 3D–H).

3 DISCUSSION
Cystectomy is an attractive technique, which was an incisional biopsy carried out prior to treatment with CGF. Cystectomy generally accounts for comforting outcome for small cysts; however, the risk of infection and complication was increased when applied to larger cysts.7 Fenestration and decompression were regarded as conservative approaches for large cyst, which need long-term therapy.14 In this case, the size of cyst is 31 mm × 44 mm × 53 mm, which is not suitable for cystectomy. Filling the cavity with autogenous grafts, allogenous grafts, xenografts or alloplastic, and synthetic grafts might be a classic treatment choice for this patient.
Increasing evidences have demonstrated the various biological effects of growth factors including promoting bone regeneration, regulating hematopoietic stem cell niche, stimulating immune system, and adjusting gastrointestinal function.15-18 CGF is a well-recognized blood extraction, which is enriched with mounts of growth factors and fibrins consisting the 3-D structure with elastic texture. It has been reported that the concentrations of vascular endothelial growth factor, fibroblast growth factor, epidermal growth factor, platelet-derived growth factor, insulin-like growth factor, and transforming growth factor beta 1 in CGF were much higher than those in whole blood.19 Synergy effects of these numerous growth factors enable CGF with multifaceted functions such as osteoconductive and osteoinductive properties, implied by CT scan in follow-up check in our study (Figure 3), which was consistent with previous study.20 Compared with previous studies using autologous bone grafting to fill the defect, CGF gel has several advantages including less surgical procedure, good medical compliance, and less medical expense.
In conclusion, this preliminary study suggests enucleation of jaw cysts and primary closure with CGF gel might be a reliable alternative for the management of odontogenic jaw cysts.
AUTHOR CONTRIBUTIONS
Binxiong Chen: Data curation; funding acquisition; investigation; writing – original draft. Yueming Liu: Formal analysis; resources; supervision; writing – original draft. Changneng Ke: Conceptualization; data curation; project administration; resources; supervision. Shi Xu: Funding acquisition; supervision; writing – review and editing.
FUNDING INFORMATION
This work was supported by the Scientific Research Projects of Medical and Health Institutions of Longhua District, Shenzhen (2022015, 2021065), Scientific Research Projects of Shenzhen Longhua District Central Hospital (202201), Regional Joint Fund of Guangdong Province (2021A1515111063), and Longhua District Social Public Welfare Scientific Research Project (LHQJCYJ202102).
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest related to this study.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Open Research
DATA AVAILABILITY STATEMENT
The data presented in this study are available from the corresponding author upon reasonable request.