All Pediatric Transplantation Articles
Export Citations
Download PDFs
-
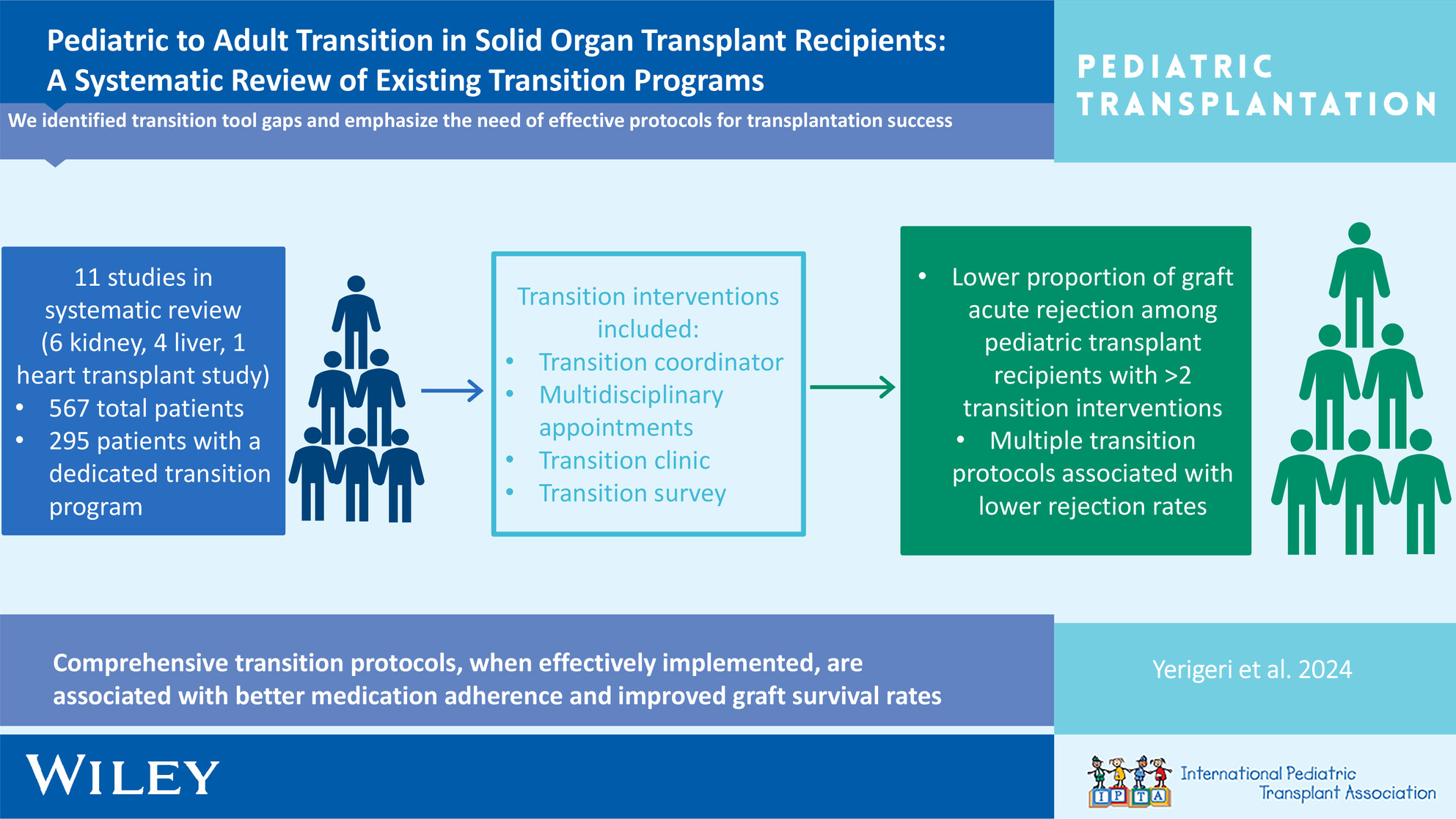
Absolute CD3+ T-Cell Counts After Anti-Thymocyte Globulin: Impact on Graft and Infectious Outcomes in Pediatric Kidney Recipientsno
Graphical Abstract
When pediatric kidney transplant recipients were compared based on the achievement (or not) of a CD3+ T-cell count < 25 cells/mm3 following rabbit anti-thymocyte globulin induction, there were no differences in infectious or graft outcomes by 12-months post-transplant.
-
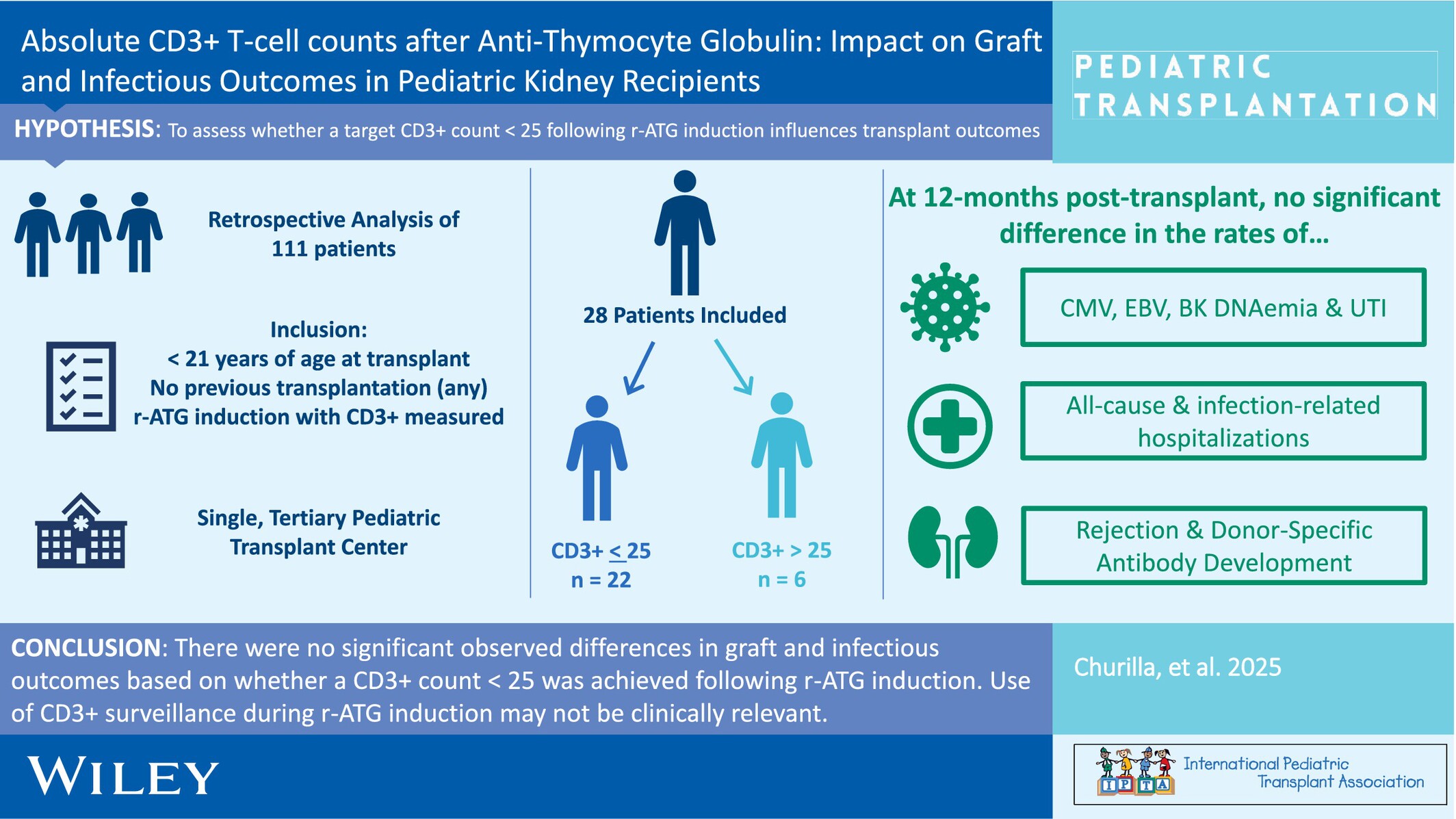
Pneumocystis jiroveci Pneumonia Infections in Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
In the current era, PJP remains a rare post-transplant complication in pediatric SOT patients. PJP infections are associated with significant morbidity, mortality, and costs. Risk factors for PJP are young age at transplant and heart transplantation. An assessment of individual risk factors should be regularly performed to optimize prevention strategies.
-
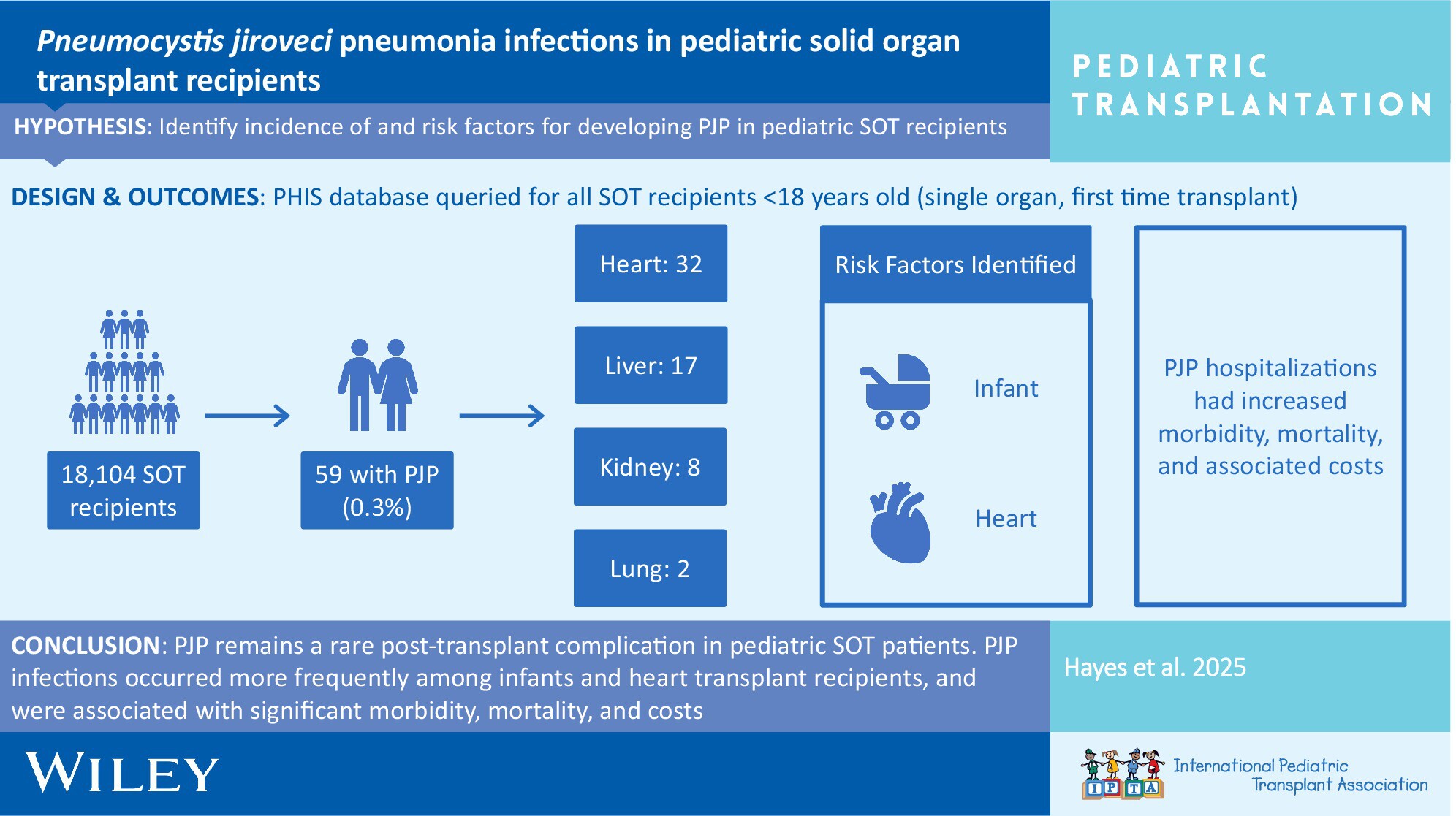
Low Incidence of Rejection and De Novo Donor-Specific Antibody Formation Following COVID-19 Vaccination or Infection Among Pediatric Kidney Transplant Recipientsno
Graphical Abstract
This study investigated the incidence of allograft rejection and de novo donor-specific antibody formation following COVID-19 vaccination or infection among pediatric kidney transplant recipients.
-
Recurrence of Primary Sclerosing Cholangitis After Pediatric Liver Transplantation: A Single-Center, Retrospective Study in Japanno
Graphical Abstract
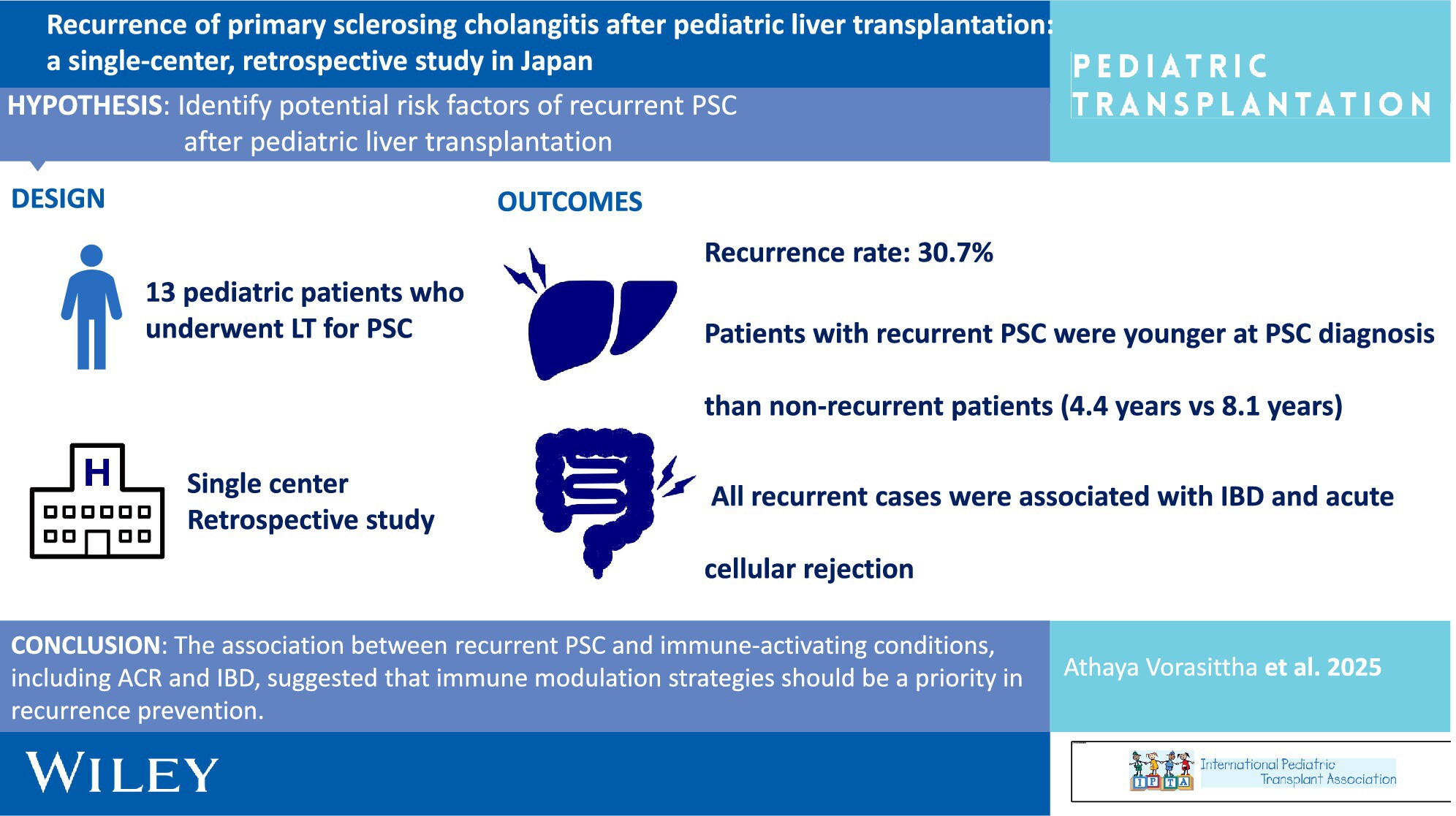
The recurrence rate was high in pediatric patients with PSC, emphasizing the need for tailored management strategies in children. The association between recurrent PSC and immune-activating conditions, including ACR and IBD, suggested that immune modulation strategies should be a priority in recurrence prevention.
-
Sex-Based Differences in Rejection Among Pediatric Solid Organ Transplant Recipientsno
Graphical Abstract
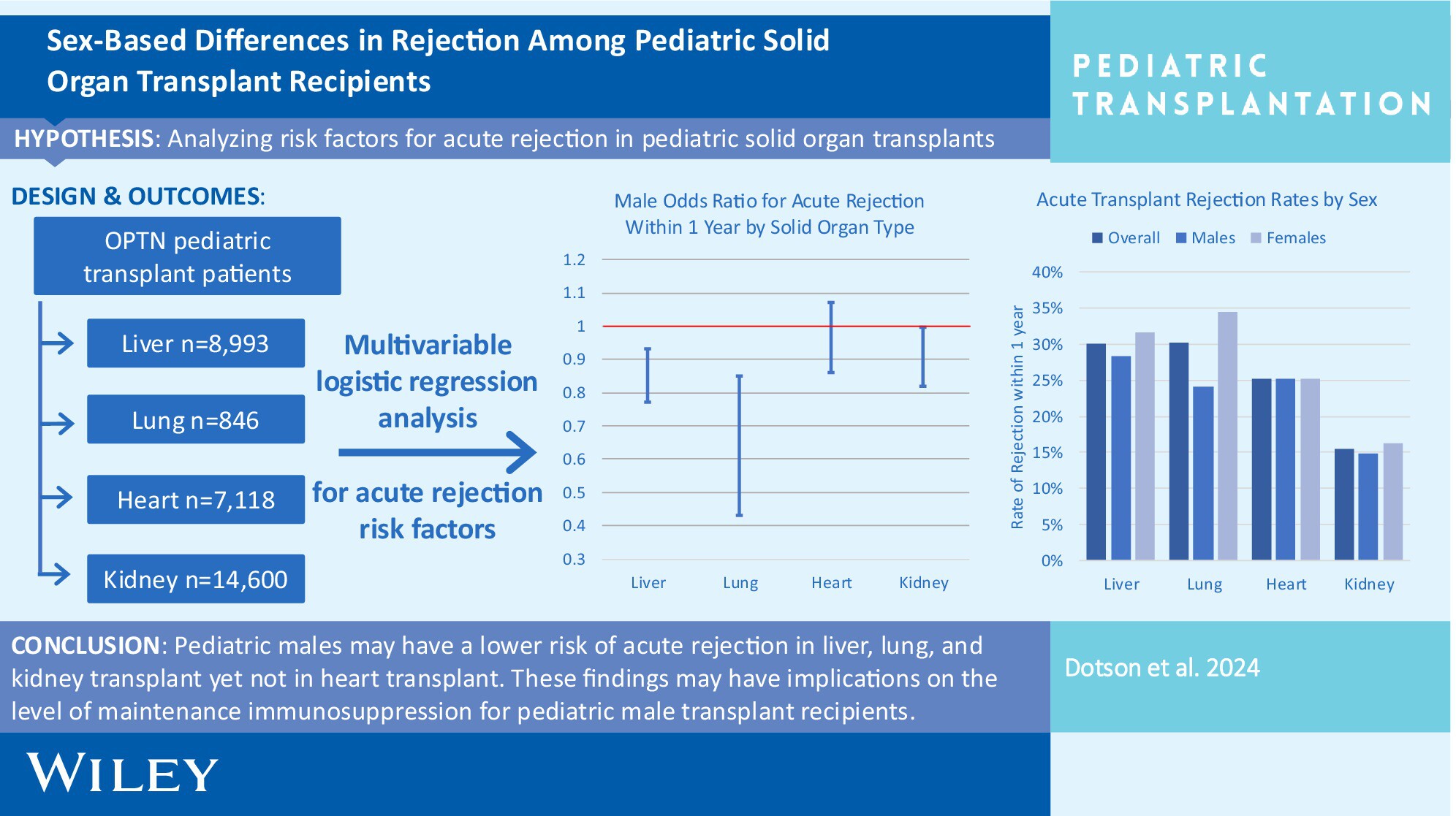
Pediatric males experienced relative protection from acute rejection in liver, lung, and kidney transplantation compared to their female counterparts in our study. This analysis helps clarify the role of recipient sex as a nonmodifiable risk factor for acute rejection and assists clinicians in stratifying risk and personalizing immunosuppression regimens.
-
Pre-Transplant Immunophenotyping in Pediatric Heart Transplant: A Role for the Immunologist?oa
Graphical Abstract
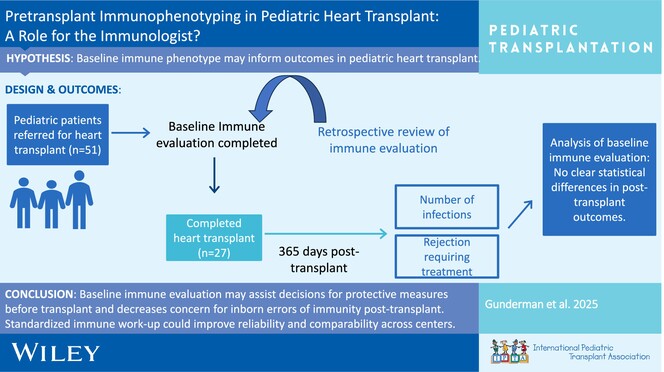
Baseline immune evaluation can assist in decisions for additional protective measures before transplant (avoidance of live vaccines, antimicrobial prophylaxis) and decrease the uncertainties in the evaluation of inborn errors of immunity after transplant. Ongoing work and developing standardized protocols for baseline immunologic work-up could improve reliability and comparability across different centers.
-
Evaluating Activated Regulatory T Cells as a Biomarker of Chronic Allograft Inflammation in Pediatric Kidney Transplant Recipientsoa
Graphical Abstract
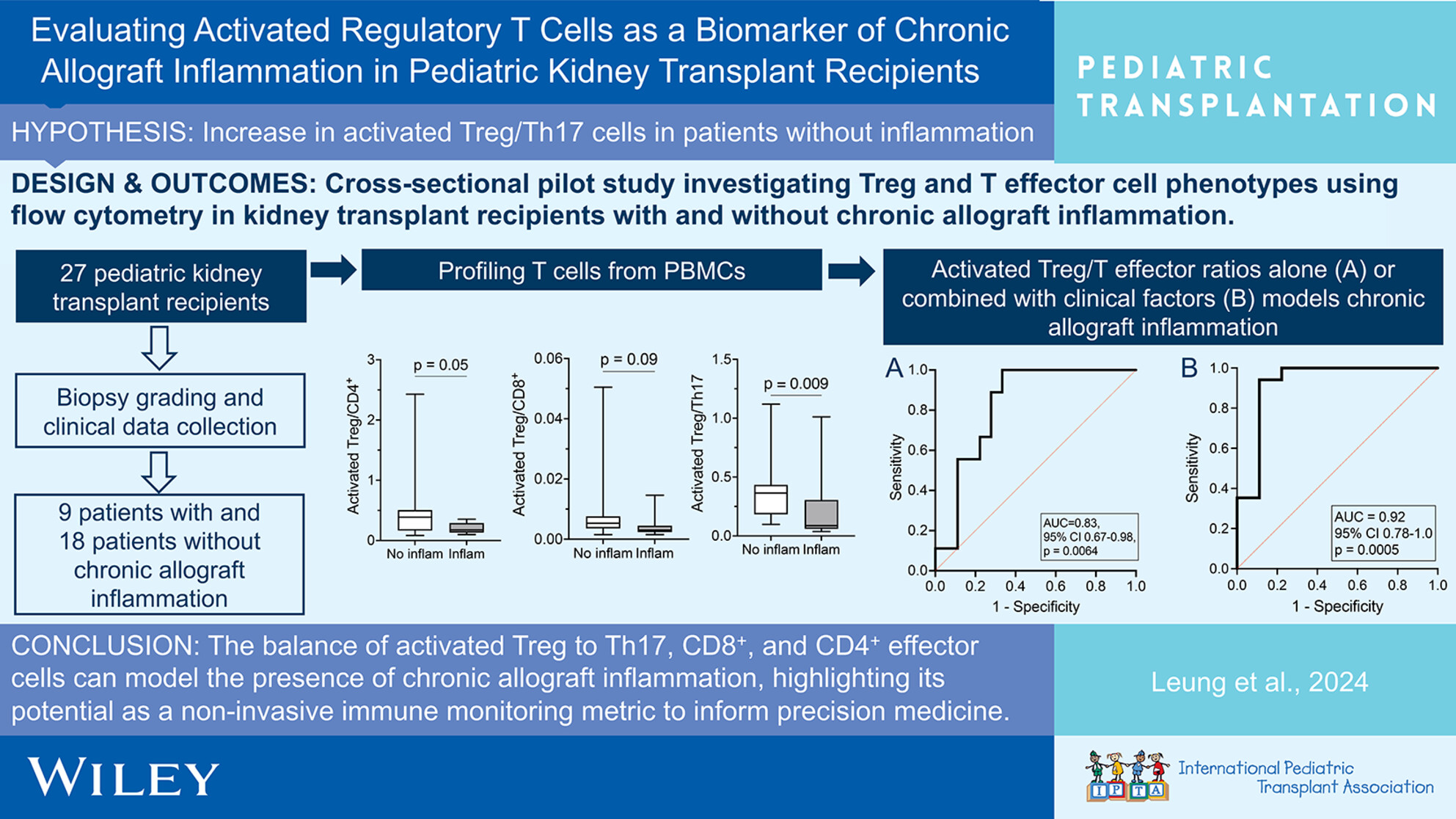
The balance between activated Treg/T effector cells demonstrates potential as a minimally invasive immune monitoring metric that can be used to help identify chronic allograft inflammation in pediatric kidney transplant recipients. Identifying patients with chronic allograft inflammation can help inform earlier intervention and precision medicine.
-
Natural Killer Cell Phenotypes and Clinical Outcomes in Pediatric Kidney TransplantationnoCollections: Special Issue on Festschrift for Richard Fine
Graphical Abstract
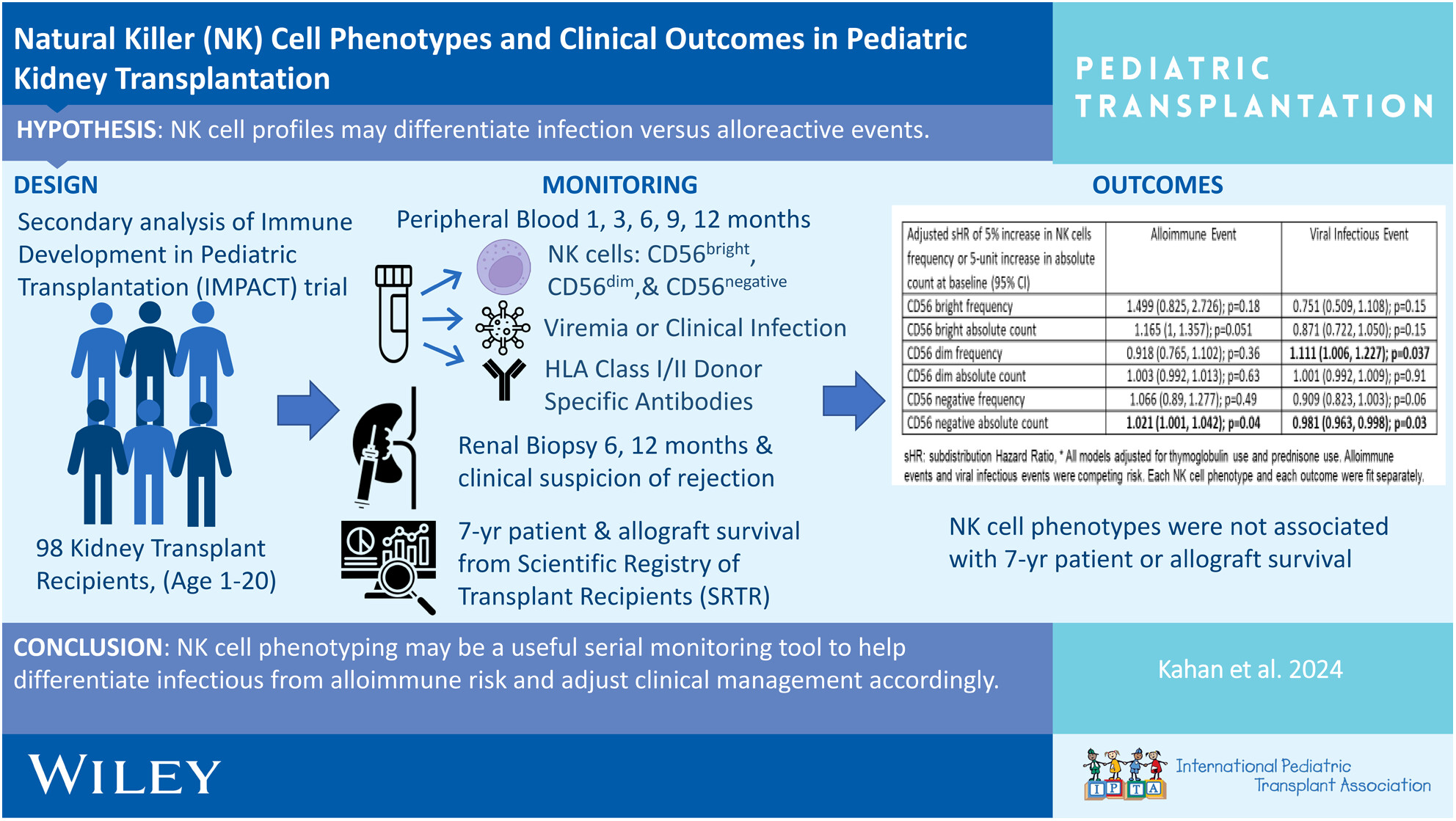
An analysis of 98 children with kidney transplants from the Immune Development of Pediatric Transplantation (IMPACT) Trial was conducted to determine the relationship between NK cell phenotypes with infection, alloreactive events, and patient/allograft survival. NK cell phenotypes may be a useful tool to differentiate between infectious and alloimmune events.
-
Longitudinal Changes in Estimated Glomerular Filtration Rate Following Repeat Heart Transplant in Children and Young Adultsno
Graphical Abstract
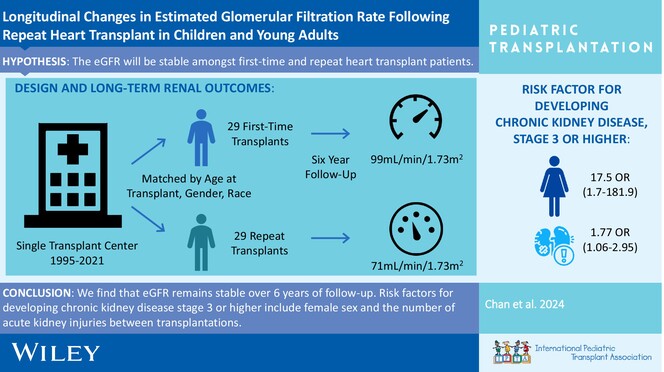
We find that renal function remains stable over a median follow-up time of 6 years for first-time repeat heart transplant recipients. Major risk factors for more advanced renal dysfunction being female sex and number of acute kidney injuries between first-time heart transplant and first-time repeat heart transplant.
-
De Novo and Progressive Pulmonary Vein Stenosis Following Pediatric Heart Transplantation: A Multicenter Retrospective Studyno
Graphical Abstract
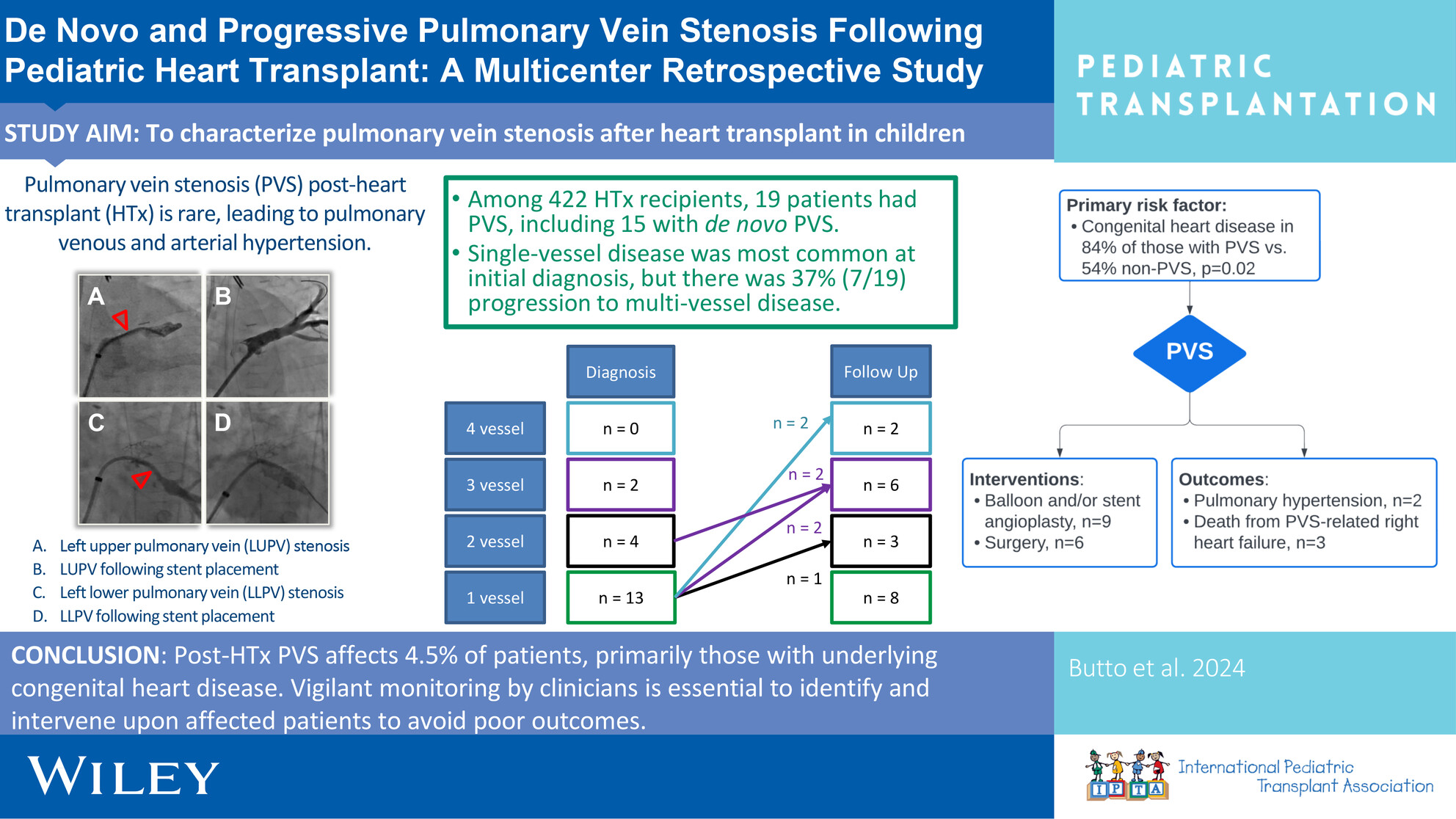
Investigating pulmonary vein stenosis following heart transplantation in children, this is the largest study of its kind that examines the prevalence, risk factors, and interventions for post-transplant PVS at two large transplant centers.
-
Norovirus Management and Outcomes in a Multicenter Pediatric Kidney Transplant Populationoa
Graphical Abstract
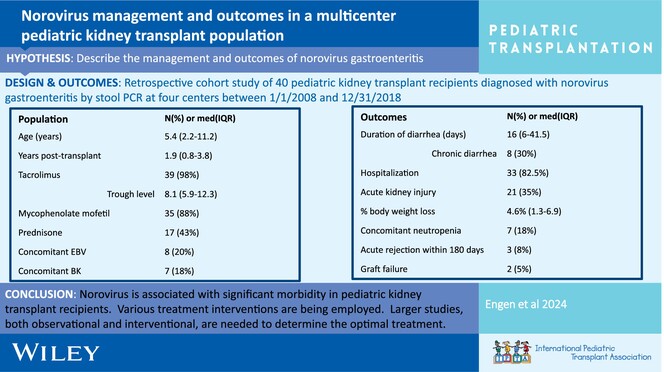
Post-transplant norovirus diarrhea persists for a median of 16 days (IQR 6–41.5 days) with 30% of patients developing chronic diarrhea. Morbidity is high, including AKI in 53% of patients, reduction in immunosuppression 20%, and acute rejection in 8% within 6 months of diagnosis.
-
BK polyomavirus DNAemia, allograft rejection, and de novo donor-specific antibodies after lowering target tacrolimus levels in pediatric kidney transplant recipientsno
Graphical Abstract
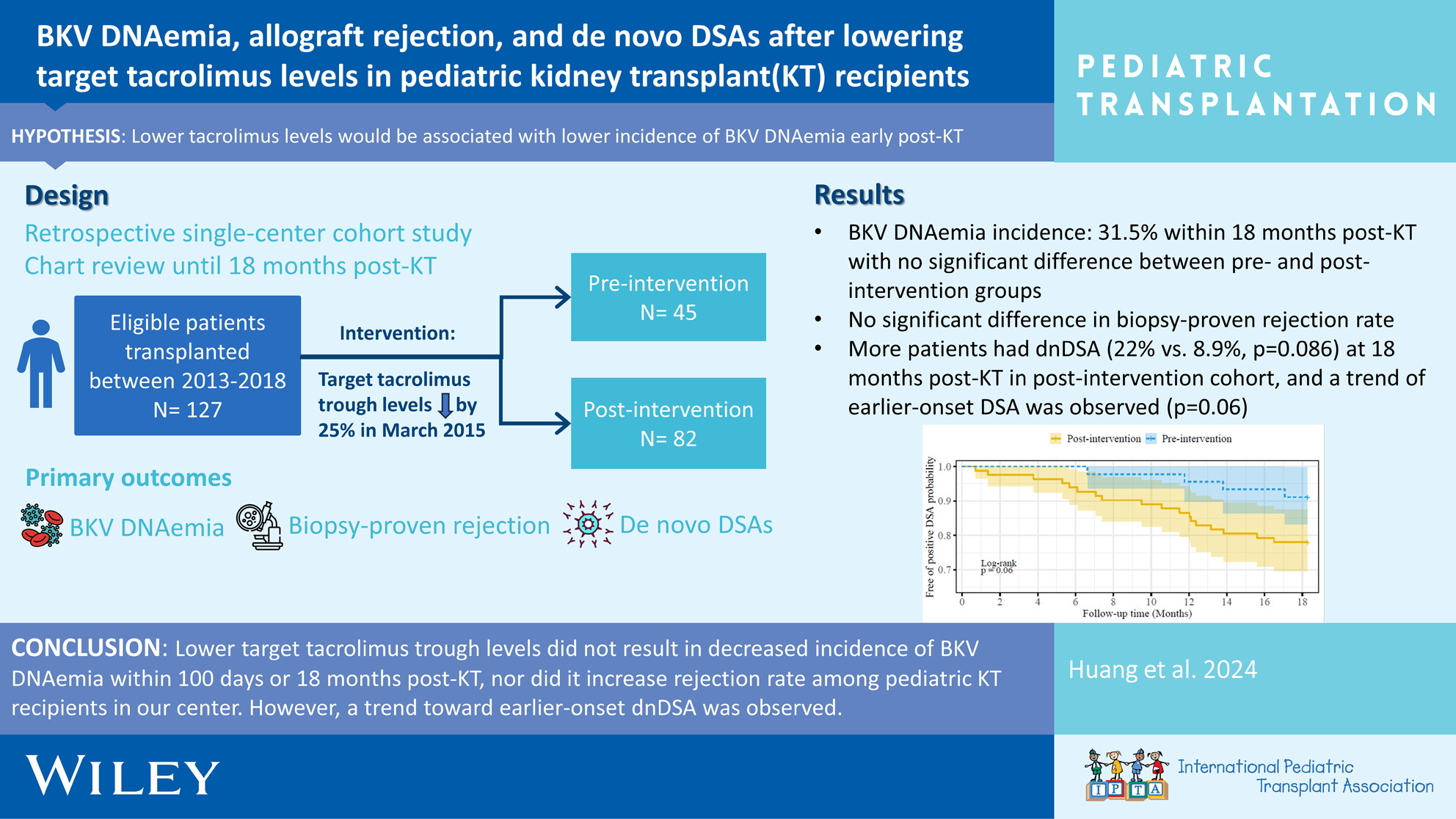
Early BKV DNAemia is common post-pediatric kidney transplant, especially in younger ages, with ~30% incidence within 18 months post-transplant. Favorable outcomes are achieved with (1) frequent monitoring of viremia and (2) timely reduction of immunosuppressive medications, which must be balanced against risk of rejection and development of HLA antibodies.