A Rare and Unexpected Reason for Unilateral Epistaxis: Nasal Septal Schwannoma
Abstract
Nasal septal schwannoma is a rare tumor. It causes complaints such as nasal congestion, nosebleeds, and headaches. There are many diseases such as nasal polyps, antrochoanal polyp, chronic rhinosinusitis, concha bullosa, inverted papilloma, and retention cyst with schwannoma diagnosis. The diagnosis is made histopathologically, and the treatment is surgery. In this case report, we presented a male patient with septal schwannoma who had nasal obstruction for a year and reviewed the last 20 years of literature on nasal schwannoma.
1. Introduction
Schwannomas are benign tumors of the nerve sheath commonly associated with cranial nerve VIII. It is observed with a frequency of 25–45% among all head and neck tumors [1–4]. Only 4% of them are seen in the nose [1]. Nasal septum is one of the places where schwannoma is rarely seen in the nose [1–5]. In this study, we presented a case of a male with septal schwannoma who had suffered nasal congestion for a year. This study was conducted to examine the frequency of schwannomas among the causes of nasal obstruction. Therefore, we also reviewed last 20 years of literature about nasal schwannoma.
2. Case Report
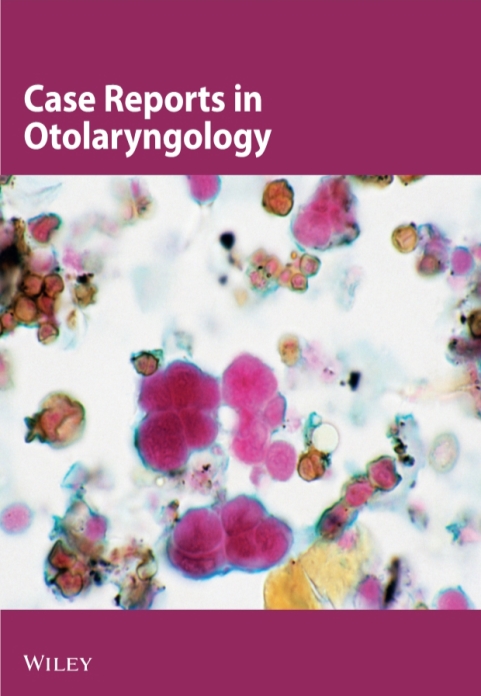
A 28-year-old male patient was admitted to our clinic with progressive nasal congestion and recurrent epistaxis. In rigid endoscopy, there was a polypoid mass originating from the septum with smooth surface and prone to bleeding. It was causing nasal obstruction on the left side of the nose (Figure 1). In paranasal sinus computed tomography (CT), approximately 16 × 40 × 35 mm-sized polypoid mass was observed on the left side, filling the nasal cavity completely (Figure 2). No extension or bone invasion to any paranasal sinuses was present. Magnetic resonance imaging (MRI) revealed a hypointense mass and heterogeneous contrast in T1 and T2 sections (Figure 3). The surgery was planned to the patient under general anesthesia. Endoscopically mucosal incision was made proximal to where the mass attaches to the septum. The procedure was continued by subperichondrial elevation. The mass was excised en bloc with the septum mucosa (Figure 4). In the histological examination of the mass, spindle cell proliferation consisting of photocellular and hypocellular alternating areas and diffuse positivity in spindle cells with S100 were observed (Figures 5 and 6). Vimentin staining was positive, though neuron-specific enolase and smooth muscle actin staining were negative. According to these observations, the mass was defined as a septum-derived schwannoma. No recurrence was observed during the patient’s 1-year follow-up.








3. Discussion
Schwannoma is a class sheath tumor often seen in the head and neck region. While approximately 25–45% of schwannomas are seen in the head and neck region [1–4], only 4% of them are seen in the nose [6]. The case of schwannoma in the nasal septum was first reported by Betkowski et al. in 1943 [7]. Schwannoma is seen especially in the 4th and 6th decades, and there is no gender dominance [8]. Nasal septal schwannoma cases reported in the last 20 years are shown in Table 1. Schwannoma often originates from the posterior part of the septum in the nose and makes complaints such as nasal congestion, nosebleeds, and headaches [6]. In our case, it originated from the anterior-middle region of the septum at young age different from the other cases. The unilateral mass in the nose was observed at 22% nasal polyps, 19% antrochoanal polyp, 13% chronic rhinosinusitis, 11% concha bullosa, 6% inverted papilloma, and 6% retention cyst. More rarely, fibrous dysplasia, lymphoma, pleomorphic adenoma, and schwannoma are seen. In such a large list, only observation is not sufficient for diagnosis [9]. Paranasal CT findings are nonspecific. CT often helps with the size of the tumor and where it originates. MRI tumor is better at differentiating from inflammatory diseases and normal tissue. It also shows intracranial extension [10]. In previous studies, findings such as “target sign” and “fascicular sign,” which are specifically observed in schwannoma tumors on MRI, have been reported [11–14].
| Author(s) | Year | Age/sex | Symptoms | Site | Treatment | Follow-up |
|---|---|---|---|---|---|---|
| Berlucchi et al. [4] | 2000 | 29/M | NO, Ep | NS | Ex | 7 years |
| Wada et al. [18] | 2000 | 62/F | NO | NS | Ex | 15 months |
| Wang et al. [12] | 2004 | 55/M | NO | NS | Ex | — |
| Rajagopal | 2005 | 54/F | NO | NS | Ex | 6 months |
| Shinohara et al. [14] | 2005 | 50/M | NO | NS | Ex | 3 years |
| Kodama et al. [19] | 2009 | 41/F | NO | NS | Ex | 2 years |
| Pauna et al. [8] | 2013 | 78/M | NO | NS | Ex | — |
| Gulia et al. [20] | 2013 | 35/F | NO | Membranous NS | Ex | 6 months |
| Cadd et al. [21] | 2014 | 31/M | NO, Ep | NS | Ex | — |
| Dhingra et al. [22] | 2014 | 28/F | NO, Ep | NS | Ex | — |
| Karatas [23] | 2016 | 31/F | NO, Ep | NS | Ex | 8 months |
| Gerritsen et al. [24] | 2017 | 16/M | NO | NS | Ex | 1 month |
| Gupta et al. [25] | 2017 | 40/F | NO, Ep | NS | Ex | 1 year |
| Valsamidis et al. [26] | 2017 | 54/M | NO, Ep | NS | Ex | 6 months |
| Min et al. [3] | 2017 | 65/F | NO | NS | Ex | 2 years |
| Devaraja et al. [27] | 2018 | 57/M | NO | NS | Ex | — |
| Alrasheed et al. [28] | 2019 | 64/F | NO, Ep | NS | Ex | 3 years |
| Bie et al. [29] | 2019 | 47/M | NO, Ep | NS | Ex | 6 months |
| Our case | 2020 | 28/M | NO, Ep | NS | Ex | 1 year |
- M: male; F: female; NO: nasal obstruction; Ep: epistaxis; NS: nasal septum; Ex: excision.
The definitive diagnosis of schwannoma tumor is made histopathologically. Schwannoma tumors are macroscopically seen as bordered and encapsulated. When stained with hemotoxylin-eosin stain and analyzed microscopically, it is divided into two patterns, Antoni A and Antoni B. Antoni A consists of spindle cells that form palisade by lining the nuclei side by side. Antoni B consists of loose myxoid stroma and a small amount of spindle cells. It is stained strongly with S-100 immunohistochemically [4, 15, 16]. In the histological examination of the mass of our patient, spindle cell proliferation consisting of photocellular and hypocellular alternating areas with S-100 and diffuse positivity in spindle cells were observed. Although neuron-specific enolase and smooth muscle actin staining were negative, vimentin staining was positive. Based on these observations, the mass was defined as septum-derived schwannoma. Treatment of nasal septal schwannoma is extensive surgical excision with a negative surgical margin. No recurrence cases were reported in literature after excision [17–29].
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.