Transseptal Access for Left Atrial Ablation: The Catheter-Probing Techniques Are Not Without Risk
No disclosures.
Risk of Catheter-Probing During Transseptal Access
Background
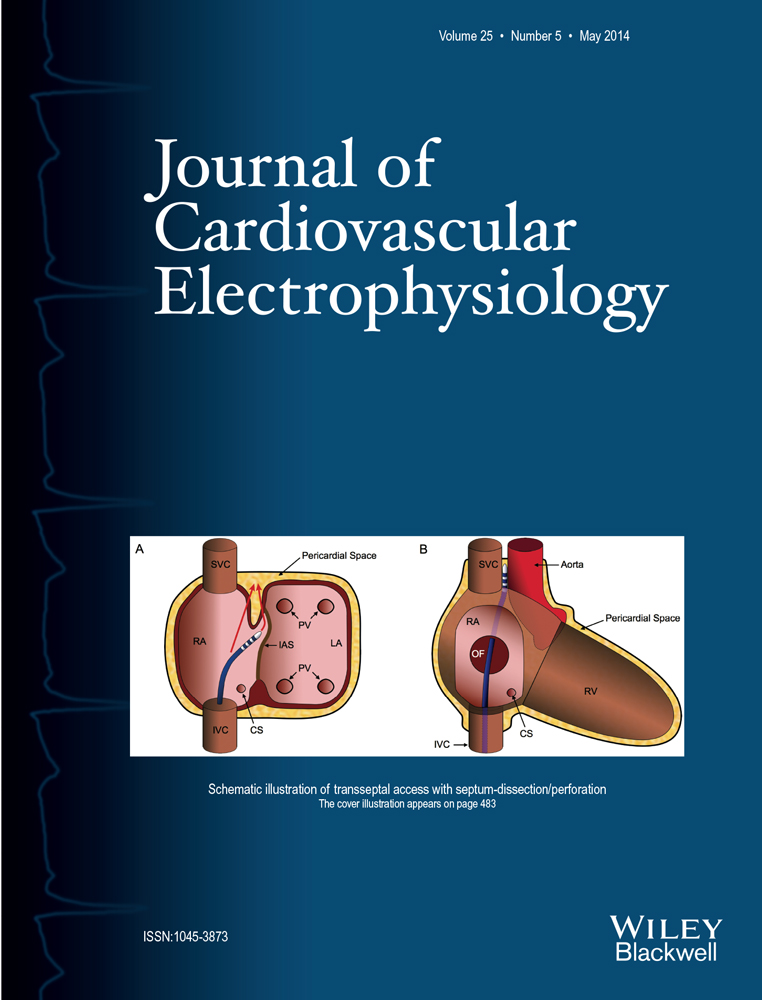
Transseptal puncture (TP) is a prerequisite for LA ablations. LA access can be gained by catheter probing in case of PFO (trans-PFO method) or puncture of the interatrial septum (IAS) using a transseptal needle. A 2nd access can again be gained via PFO, a 2nd TP or catheter probing of the previous puncture site (probe-TS method). This study investigates the risk factors and complications related to the mode of transseptal access.
Methods and Results
From August 2010 to August 2012, a total of 544 LA ablations, were performed. The mode of LA access was either a double TP or a single TP followed by the probe-TS or the trans-PFO method, respectively. TP was always guided by TEE and was successfully performed without complications in all cases. In contrast, 6/410 patients (1.5%) in whom catheter probing was performed (probe-TS, n = 4, trans-PFO, n = 2) had a dissection of the superior IAS originating from inside the oval fossa (n = 5) or perforation above the oval fossa (n = 1). Perforation into the pericardial space occurred in 4/6 patients, leading to one cardiac tamponade. In 5/6 patients, LA ablation was successfully completed, after repeated TP, despite effective anticoagulation. Patients with complications had the following characteristics: LA size 46 ± 4 mm, persistent AF (5/6), a repeat transseptal procedure (3/6) and a right-sided pouch (RSP, 5/6).
Conclusions
Interatrial septum dissection/perforation, occasionally with perforation into the pericardial space, is an unreported complication of TP, especially with the catheter-probing techniques. An RSP is an unrecognized risk factor in this context and can be visualized by TEE.