Structures for quality assurance and measurements for kidney replacement therapies: A multinational study from the ISN-GKHA
Corresponding Author
Udeme E. Ekrikpo
Department of Internal Medicine, University of Uyo Teaching Hospital, Uyo, Nigeria
Correspondence
Udeme E. Ekrikpo, Department of Internal Medicine, University of Uyo Teaching Hospital, Uyo, Nigeria.
Email: [email protected]
Search for more papers by this authorBianca Davidson
Division of Nephrology and Hypertension, Department of Medicine, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa
Search for more papers by this authorViviane Calice-Silva
Pro-Rim Foundation, Joinville, Santa Catarina, Brazil
Department of Clinical Medicine, Faculty of Medicine, University of the Region of Joinville (UNIVILLE), Joinville, Santa Catarina, Brazil
Search for more papers by this authorSabine Karam
Division of Nephrology and Hypertension, Department of Medicine, University of Minnesota, Minneapolis, Minnesota, USA
Division of Nephrology and Hypertension, Department of Internal Medicine, American University of Beirut, Beirut, Lebanon
Search for more papers by this authorMohamed A. Osman
Department of Family Medicine, University of Ottawa, Ottawa, Ontario, Canada
Search for more papers by this authorSilvia Arruebo
The International Society of Nephrology, Brussels, Belgium
Search for more papers by this authorFergus J. Caskey
Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK
Search for more papers by this authorSandrine Damster
The International Society of Nephrology, Brussels, Belgium
Search for more papers by this authorJo-Ann Donner
The International Society of Nephrology, Brussels, Belgium
Search for more papers by this authorVivekanand Jha
George Institute for Global Health, New Delhi, India
School of Public Health, Imperial College, London, UK
Manipal Academy of Higher Education, Manipal, India
Search for more papers by this authorAdeera Levin
Division of Nephrology, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada
Search for more papers by this authorMasaomi Nangaku
Division of Nephrology and Endocrinology, The University of Tokyo Graduate School of Medicine, Tokyo, Japan
Search for more papers by this authorSyed Saad
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Search for more papers by this authorMarcello Tonelli
Department of Medicine, University of Calgary, Calgary, Alberta, Canada
Canada and Pan-American Health Organization/World Health Organization Collaborating Centre in Prevention and Control of Chronic Kidney Disease, University of Calgary, Calgary, Alberta, Canada
Search for more papers by this authorFeng Ye
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Search for more papers by this authorIkechi G. Okpechi
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Division of Nephrology and Hypertension, University of Cape Town, Cape Town, South Africa
Kidney and Hypertension Research Unit, University of Cape Town, Cape Town, South Africa
Search for more papers by this authorAminu K. Bello
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Search for more papers by this authorDavid W. Johnson
Department of Kidney and Transplant Services, Princess Alexandra Hospital, Brisbane, Queensland, Australia
Centre for Kidney Disease Research, University of Queensland at Princess Alexandra Hospital, Brisbane, Queensland, Australia
Translational Research Institute, Brisbane, Queensland, Australia
Australasian Kidney Trials Network, University of Queensland, Brisbane, Queensland, Australia
Search for more papers by this authorCorresponding Author
Udeme E. Ekrikpo
Department of Internal Medicine, University of Uyo Teaching Hospital, Uyo, Nigeria
Correspondence
Udeme E. Ekrikpo, Department of Internal Medicine, University of Uyo Teaching Hospital, Uyo, Nigeria.
Email: [email protected]
Search for more papers by this authorBianca Davidson
Division of Nephrology and Hypertension, Department of Medicine, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa
Search for more papers by this authorViviane Calice-Silva
Pro-Rim Foundation, Joinville, Santa Catarina, Brazil
Department of Clinical Medicine, Faculty of Medicine, University of the Region of Joinville (UNIVILLE), Joinville, Santa Catarina, Brazil
Search for more papers by this authorSabine Karam
Division of Nephrology and Hypertension, Department of Medicine, University of Minnesota, Minneapolis, Minnesota, USA
Division of Nephrology and Hypertension, Department of Internal Medicine, American University of Beirut, Beirut, Lebanon
Search for more papers by this authorMohamed A. Osman
Department of Family Medicine, University of Ottawa, Ottawa, Ontario, Canada
Search for more papers by this authorSilvia Arruebo
The International Society of Nephrology, Brussels, Belgium
Search for more papers by this authorFergus J. Caskey
Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, UK
Search for more papers by this authorSandrine Damster
The International Society of Nephrology, Brussels, Belgium
Search for more papers by this authorJo-Ann Donner
The International Society of Nephrology, Brussels, Belgium
Search for more papers by this authorVivekanand Jha
George Institute for Global Health, New Delhi, India
School of Public Health, Imperial College, London, UK
Manipal Academy of Higher Education, Manipal, India
Search for more papers by this authorAdeera Levin
Division of Nephrology, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada
Search for more papers by this authorMasaomi Nangaku
Division of Nephrology and Endocrinology, The University of Tokyo Graduate School of Medicine, Tokyo, Japan
Search for more papers by this authorSyed Saad
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Search for more papers by this authorMarcello Tonelli
Department of Medicine, University of Calgary, Calgary, Alberta, Canada
Canada and Pan-American Health Organization/World Health Organization Collaborating Centre in Prevention and Control of Chronic Kidney Disease, University of Calgary, Calgary, Alberta, Canada
Search for more papers by this authorFeng Ye
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Search for more papers by this authorIkechi G. Okpechi
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Division of Nephrology and Hypertension, University of Cape Town, Cape Town, South Africa
Kidney and Hypertension Research Unit, University of Cape Town, Cape Town, South Africa
Search for more papers by this authorAminu K. Bello
Division of Nephrology and Immunology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Search for more papers by this authorDavid W. Johnson
Department of Kidney and Transplant Services, Princess Alexandra Hospital, Brisbane, Queensland, Australia
Centre for Kidney Disease Research, University of Queensland at Princess Alexandra Hospital, Brisbane, Queensland, Australia
Translational Research Institute, Brisbane, Queensland, Australia
Australasian Kidney Trials Network, University of Queensland, Brisbane, Queensland, Australia
Search for more papers by this authorAminu K. Bello and David W. Johnson are co-chairs for the International Society of Nephrology Global Kidney Health Atlas (ISN-GKHA) and co-senior authors.
Abstract
Aim
Optimal care for patients with kidney failure reduces the risks of adverse health outcomes, including cardiovascular events and death. We evaluated data from the third iteration of the International Society of Nephrology Global Kidney Health Atlas (ISN-GKHA) to assess the capacity for quality service delivery for kidney failure care across countries and regions.
Method
We explored the quality of kidney failure care delivery and the monitoring of quality indicators from data provided by an international survey of stakeholders from countries affiliated with the ISN from July to September 2022.
Results
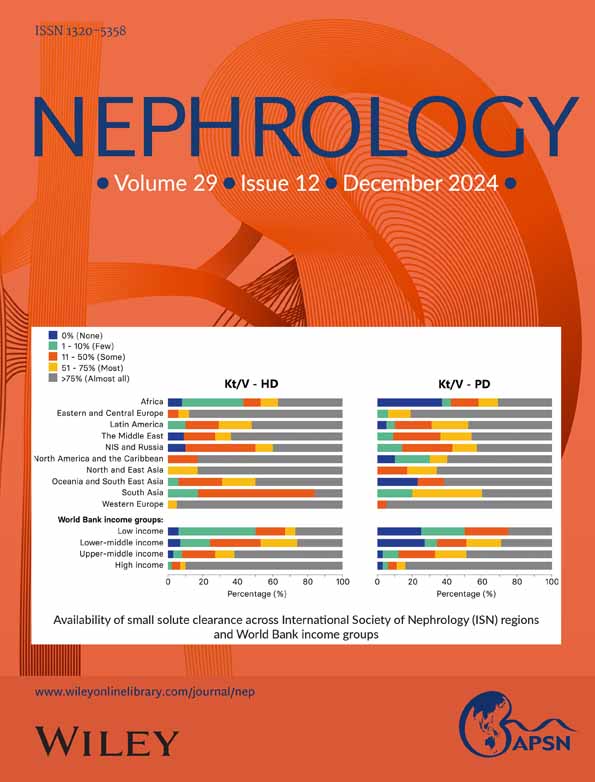
One hundred and sixty seven countries participated in the survey, representing about 97.4% of the world's population. In countries where haemodialysis (HD) was available, 81% (n = 134) provided standard HD sessions (three times weekly for 3–4 h per session) to patients. Among countries with peritoneal dialysis (PD) services, 61% (n = 101) were able to provide standard PD care (3–4 exchanges per day). In high-income countries, 98% (n = 62) reported that >75% of centers regularly monitored dialysis water quality for bacteria compared to 28% (n = 5) of low-income countries (LICs). Capacity to monitor the administration of immunosuppression drugs was generally available in 21% (n = 4) of LICs, compared to 90% (n = 57) of high-income countries. There was significant variability between and within regions and country income groups in reporting the quality of services utilized for kidney replacement therapies.
Conclusion
Quality assurance standards on diagnostic and treatment tools were variable and particularly infrequent in LICs. Standardization of delivered care is essential for improving outcomes for people with kidney failure.

Supporting Information
| Filename | Description |
|---|---|
| nep14402-sup-0001-Supplementary_Figure_1.tifTIFF image, 1.5 MB | Figure S1: Administration of incremental haemodialysis and peritoneal dialysis across ISN regions and World Bank income groups. |
| nep14402-sup-0002-Supplementary_Figure_2.tifTIFF image, 1.4 MB | Figure S2: Routine blood pressure monitoring in individuals on haemodialysis and peritoneal dialysis across the ISN regions and World Bank income groups. |
| nep14402-sup-0003-Supplementary_Figure_3.tifTIFF image, 1.2 MB | Figure S3: Frequency of nephrologist review of individuals on haemodialysis across ISN regions and World Bank income groups. |
| nep14402-sup-0004-Supplementary_Figure_4.tifTIFF image, 1.3 MB | Figure S4: Availability of multidisciplinary teams to cater to chronic haemodialysis patients across ISN regions and World Bank income groups. |
| nep14402-sup-0005-Supplementary_Figure_5.tifTIFF image, 1.3 MB | Figure S5: Reporting of delayed graft function across ISN regions and World Bank income groups. |
| nep14402-sup-0006-Supplementary_Figure_6.tifTIFF image, 1.2 MB | Figure S6: Routine measurement and reporting of graft rejection rates across ISN regions and World Bank income groups. |
| nep14402-sup-0007-Supplementary_Figure_7.tifTIFF image, 1.2 MB | Figure S7: Allograft function monitoring across ISN regions and World Bank income groups. |
| nep14402-sup-0008-Supplementary_Tables.pdfPDF document, 373.8 KB | Table S1: Routine monitoring of hemoglobin and bone mineral disease parameters in the hemodialysis population. Table S2: Routine monitoring of HIV, Hepatitis B and C virology in the haemodialysis population. Table S3: Routine monitoring of haemoglobin and bone mineral disease parameters in the peritoneal dialysis population. Table S4: Early provision of culturally appropriate information to patients, caregivers, and relatives about the risks and benefits of transplantation. Table S5: Availability of effective preventive therapy to control viral and bacterial infections in transplant patients. Table S6: Timely access to operating space for kidney transplantation. Table S7: Standard framework for organ transplantation. |
Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
- 1Luyckx VA, Smyth B, Harris DC, et al. Dialysis funding, eligibility, procurement, and protocols in low-and middle-income settings: results from the International Society of Nephrology collection survey. Kidney Int Suppl. 2020; 10: e10-e18.
- 2Thurlow JS, Joshi M, Yan G, et al. Global epidemiology of end-stage kidney disease and disparities in kidney replacement therapy. Am J Nephrol. 2021; 52: 98-107.
- 3Bello AK, Okpechi IG, Levin A, et al. An update on the global disparities in kidney disease burden and care across world countries and regions. Lancet Glob Health. 2024; 12: e382-e395.
- 4Bello AK, Levin A, Lunney M, et al. Status of care for end stage kidney disease in countries and regions worldwide: international cross sectional survey. BMJ. 2019; 367.
- 5Li P, Garcia-Garcia G, Lui S-F, et al. Kidney health for everyone everywhere–from prevention to detection and equitable access to care. Braz J Med Biol Res. 2020; 53:e9614.
- 6Robinson BM, Akizawa T, Jager KJ, Kerr PG, Saran R, Pisoni RL. Factors affecting outcomes in patients reaching end-stage kidney disease worldwide: differences in access to renal replacement therapy, modality use, and haemodialysis practices. Lancet. 2016; 388: 294-306.
- 7Bello AK, Johnson DW, Feehally J, et al. Global kidney health atlas (GKHA): design and methods. Kidney Int Suppl. 2017; 7: 145-153.
- 8Bello AK, Levin A, Tonelli M, et al. Assessment of global kidney health care status. JAMA. 2017; 317: 1864-1881.
- 9Bello AK, Okpechi IG, Jha V, Harris DCH, Levin A, Johnson DW. Understanding distribution and variability in care organization and services for the management of kidney care across world regions. Kidney Int Suppl. 2021; 11: e4-e10.
- 10Lowrie E, Laird N, Parker T, et al. Effect of the hemodialysis prescription on patient morbidity: report from the National Cooperative Dialysis Study. N Engl J Med. 1981; 305: 1176-1181.
- 11Cheung AK, Levin NW, Greene T, et al. Effects of high-flux hemodialysis on clinical outcomes: results of the HEMO study. J Am Soc Nephrol. 2003; 14: 3251-3263.
- 12Paniagua R, Amato D, Vonesh E, et al. Effects of increased peritoneal clearances on mortality rates in peritoneal dialysis: ADEMEX, a prospective, randomized, controlled trial. J Am Soc Nephrol. 2002; 13: 1307-1320.
- 13Lo W, Bargman JM, Burkart J, et al. ISPD. Guías clínicas/Recomendaciones. Perit Dial Int. 2006; 26: 520-522.
- 14Chan CT, Blankestijn PJ, Dember LM, et al. Dialysis initiation, modality choice, access, and prescription: conclusions from a kidney disease: improving global outcomes (KDIGO) controversies conference. Kidney Int. 2019; 96: 37-47.
- 15Brown EA, Blake PG, Boudville N, et al. International Society for peritoneal dialysis practice recommendations: prescribing high-quality goal-directed peritoneal dialysis. Perit Dial Int. 2020; 40: 244-253.
- 16Bharati J, Jha V, Levin A. The global kidney health atlas: burden and opportunities to improve kidney health worldwide. Ann Nutr Metab. 2020; 76: 25-30.
- 17Hyodo T, Hirawa N, Hayashi M, et al. Present status of renal replacement therapy at 2015 in Asian countries (Myanmar, Vietnam, Thailand, China, and Japan). Renal Replacement Therapy. 2017; 3: 1-14.
10.1186/s41100-016-0082-7 Google Scholar
- 18Cheetham MS, Cho Y, Krishnasamy R, et al. Multicentre registry analysis of incremental peritoneal dialysis incidence and associations with patient outcomes. Perit Dial Int. 2023; 43: 383-394.
- 19Dhoot A, Brown EA, Robinson B, et al. Incremental peritoneal dialysis: Incremental gains. SAGE Publications; 2023: 355-358.
- 20Sandrini M, Vizzardi V, Valerio F, et al. Incremental peritoneal dialysis: a 10 year single-centre experience. J Nephrol. 2016; 29: 871-879.
- 21Figueiredo AE, de Souza UJ, Bernardini J, et al. Determining nurse staffing dor peritoneal dialysis care. Nephrol Nurs J. 2016; 43: 6.
- 22Bernardini J. A formula for determining appropriate nurse: patient ratios in PD programs. Perit Dial Int. 2009; 29:S13.
- 23Finkelstein FO, Ezekiel OO, Raducu R. Development of a peritoneal dialysis program. Blood Purif. 2011; 31: 121-124.
- 24Abu-Aisha H, Elamin S. Peritoneal dialysis in Africa. Perit Dial Int. 2010; 30: 23-28.
- 25Bharati J, Jha V. Achieving dialysis adequacy: a global perspective. Seminars in Dialysis. Vol 33. Wiley; 2020: 490, 490-498, 498.
10.1111/sdi.12924 Google Scholar
- 26Oguejiofor F, Kiggundu DS, Bello AK, et al. International Society of Nephrology Global Kidney Health Atlas: structures, organization, and services for the management of kidney failure in Africa. Kidney Int Suppl. 2021; 11: e11-e23.
- 27Ashu JT, Mwangi J, Subramani S, Kaseje D, Ashuntantang G, Luyckx VA. Challenges to the right to health in sub-Saharan Africa: reflections on inequities in access to dialysis for patients with end-stage kidney failure. Int J Equity Health. 2022; 21: 126.
- 28Hasan LM, Shaheen DA, El Kannishy GA, et al. Is health-related quality of life associated with adequacy of hemodialysis in chronic kidney disease patients? BMC Nephrol. 2021; 22: 1-12.