

Predictors of operative mortality among cardiac surgery patients with prolonged ventilation
Abstract
Background
Prolonged ventilation after cardiac surgery affects survival and increases morbidity. Previous studies have focused on predicting this complication preoperatively; however, indicators of poor outcome in those requiring prolonged ventilation remain ill-defined. We sought to identify predictors of operative mortality in cardiac surgery patients who experience prolonged mechanical ventilation.
Methods
1698 patients who underwent cardiac surgery (CAB, aortic valve replacement ± CAB, or mitral valve repair/replacement ± CAB) required prolonged postoperative mechanical ventilation (>24 hours) between 2012 to 2016 in a statewide consortium. Perioperative factors were evaluated to identify the association with operative mortality. Covariates were selected through bootstrap aggregation to fit multivariable logistic regression models. The relative strength of association was determined by the Wald chi-square statistic.
Results
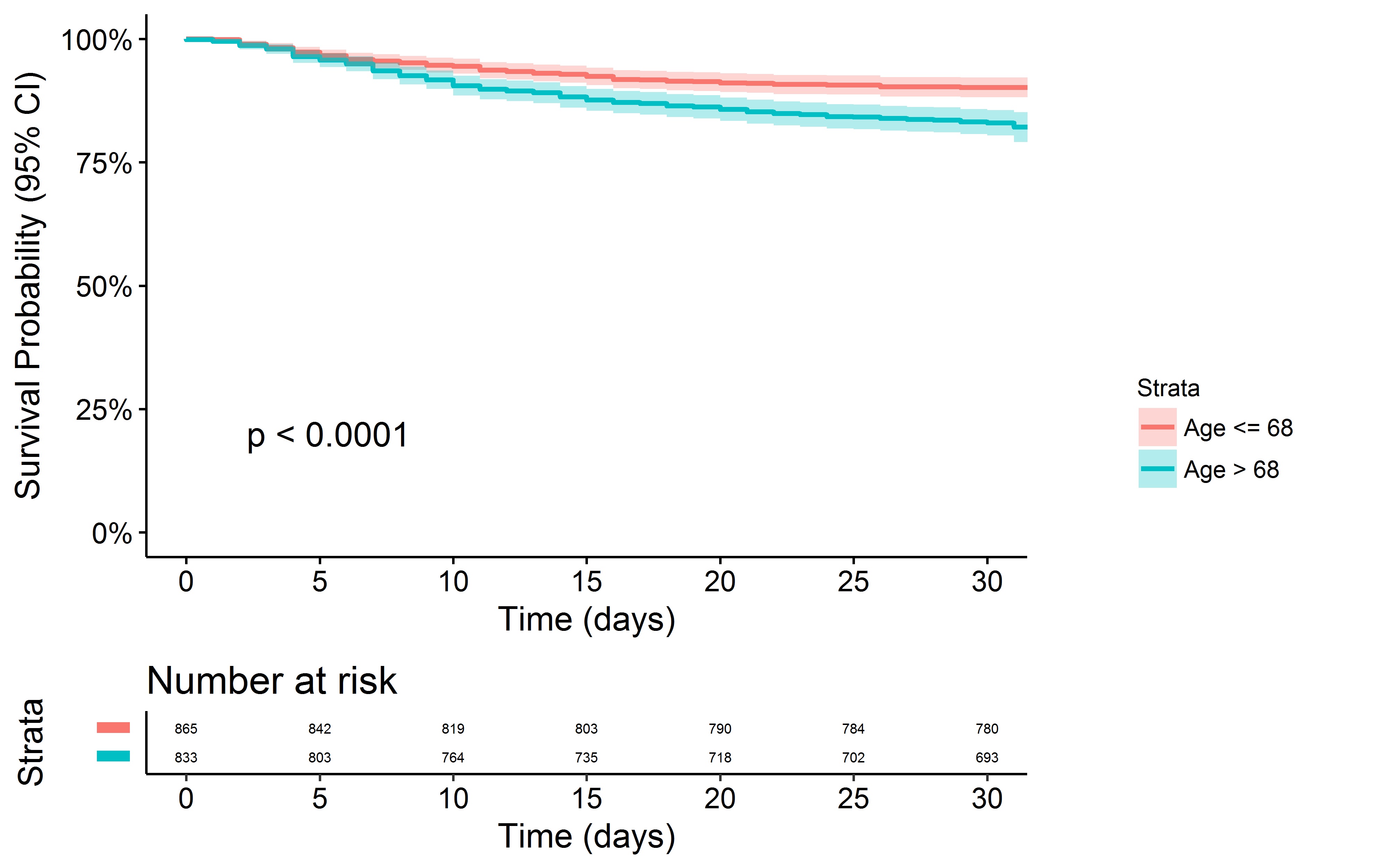
Median patient age was 68 years [IQR 61 to 76], 38% (644/1,698) were female, median duration of mechanical ventilation was 65 hours [IQR 38 to 143], median STS predicted risk of mortality was 3.1% [IQR 1.4 to 6.9%], and 15.7% (266/1698) suffered operative mortality. Among preoperative and operative characteristics, patient age and intraoperative initiation of extracorporeal membrane oxygenation (ECMO) were the strongest correlates of operative mortality on the multivariate analysis. Among postoperative factors, cardiac arrest and renal failure requiring dialysis were the strongest predictors of risk-adjusted operative mortality. Type of operation or surgical center had no association to mortality after risk adjustment.
Conclusion
Prolonged ventilation following cardiac surgery is associated with a five-fold increase in operative mortality. In these patients, operative mortality is associated with older age, intraoperative initiation of ECMO, postoperative cardiac arrest, and renal failure requiring dialysis.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}