The effect of design thinking approach in interprofessional education programme of human sexuality course: A quasi-experimental design
Abstract
Aims
To determine the effect of design thinking approach in interprofessional education programme of human sexuality course.
Design
A pre-test and post-test of single-group quasi-experimental study.
Methods
The 35 nursing students and seven psychology students in their third year were selected by the computer randomly sampling through the lottery method. The course proceeded between September 2019 and January 2020. The participants had received an 8-week, 16-hr design thinking approach in interprofessional education programme of human sexuality course (one section per week, 2 hr per section). We used the nursing attitude toward sexual healthcare scale, nursing intervention toward sexual healthcare scale to assess students' attitude and behaviour intention toward sexual health care and competence of interprofessional education scale to assess students' competence of cooperation before and after the teaching programme. Data analysis used descriptive statistics and t-tests. A qualitative reflection log was also provided and analysed for themes. The SQUIRE-EDU checklist was followed.
Results
The students' attitude and behavioural intention dimension score in the post-test is higher than those in the pre-test and reach statistically significant differences both in total and subscale. Interprofessional core competence score of Observation Experience, Reflective Feedback, Interprofessional Cooperation, Innovative Design, and Applied Technology score in the post-test is higher than those in the pre-test and reach statistically significant differences both in total and subscale. Design thinking in interprofessional education programme of human sexuality course could significantly improve both nursing and psychology students' attitude, behaviour intention of providing sexual health care and competence of interprofessional cooperation.
1 INTRODUCTION
Sexual health is defined by the WHO as “a state of physical, emotional, mental and social well-being in relation to sexuality…” (WHO, 2018). From the definition, we recognize human sexuality is a complex topic that is influenced through biological, psychological and sociocultural perspectives. Sexual health is a highly important aspect of quality of life throughout human life course (Flynn et al., 2016). Many acute or chronic illnesses and their treatment may cause neurotic, vascular and endocrine impairment and psychologic stress of disease process which impinge on sexual health (Hassanin et al., 2018; Verschuren et al., 2010). Furthermore, compromised sexual dysfunction may also increase the patient's stress or cause low self-esteem, leading to destruction of trust and interpersonal relationship, adversely affect one's psycho-emotional, physical and social well-being (Cooper et al., 2018; Papadopoulou et al., 2019). Faced with the impact of sexual health caused by the disease process, learning to adapt to the new sexual life pattern has become an important consideration in restoring the quality of life (Elliott et al., 2017). Most patients are more likely to discuss their sexual health needs with their healthcare professionals; nevertheless, it is still a certain difficult task in clinical practice in today (Huang et al., 2020; Zéler & Troadec, 2020). To support students and obtain these comprehensive capabilities, medical education should expand beyond traditional single discipline-based, teacher-centred, lecture teaching, further emphasizing “learning by doing” and the need for teamwork and collaboration. Medical education scholars believe that interprofessional education (IPE) can have an impact on the organizational culture of clinical practice and promote collaborative care, thereby improving health outcomes (Cahn et al., 2016). The adoption of IPE across the learning continuum is urgently needed (Cox et al., 2016). Design thinking (DT) is a framework for interdisciplinary collaboration and ensure the process of problem-solving is always related to the patients (Van De Grift & Kroeze, 2016), and medical teachers should deepen the theory and practice in the application of DT in the teaching field (Madson, 2021).
Currently, the use of interprofessional collaboration to improve healthcare delivery is increasingly being used. They have been used to manage female sexual dysfunction (Chua et al., 2019), clinical education for increased paediatric sexual abuse emergency care confidence and self-efficacy (Jordan et al., 2019). Furthermore, a literature uses a DT strategy to assess health needs, including the sexual health of college students, and argues that DT is a suitable strategy for college students with IDD (Milroy et al., 2021). However, there is a lack of empirical studies investigating the effect of the application of DT approach in the IPE education programme to improve the competence of healthcare professionals in human sexuality in universities.
1.1 Background
1.1.1 Interprofessional education
Healthcare professionals need to increase interprofessional cooperation to ensure comprehensive and efficient care in today's continuously changing healthcare environment (Guerin, 2014). IPE is a strategic, effectively instructive approach for preparing health professions students to deliver holistic care in the complex healthcare environment (Fusco & Foltz-Ramos, 2018; McGettigan & McKendree, 2015; Tsakitzidis et al., 2015). The perspectives involved in sexual health issues include physical and psychological perspectives (Rullo et al., 2018; Sung et al., 2016). Most patients are more likely to discuss their sexual health needs with their healthcare professionals; nevertheless, it is still a specific difficult task in clinical practice (Huang et al., 2020; Zéler & Troadec, 2020). More than 90% of health practitioners do not initiate discussions on sexual concerns with patients (Ho & Fernández, 2006). Clinical care providers cannot deal with patients' sexual health issues by relying on a single discipline. There are seldom professionals prepared for such discussion because of restrictive attitude, discomfort and inability to address patients' sexual concerns (Kim et al., 2011). In the 2019 review literature, the main factors affecting nurses providing sexual health care are personal knowledge, confidence and attitude, comfort discussing sexual health and time, responsibility pressure or institutional support (Fennell & Grant, 2019). Providing the opportunity to practice these discussions can increase nurses' communication skill and the comfort levels in providing sexual education (Jonsdottir et al., 2016). According to the report of Belgium for 10 years of IPE teamwork education and training, 80% of the participants in the IPE believe that the IPE model can increase professional knowledge, improve the relationship with other professionals and have a deeper understanding of the problem-solving methods in the team (Tsakitzidis et al., 2015). Therefore, students of psychology and nursing departments participate in IPE and learn from each other's majors, which helps develop empathy and care attitudes and behavioural intentions to deal with patients' sexual health problems. The intended consequence of effective IPE should be enhanced collaborative practice (Cahn et al., 2016).
1.1.2 Design thinking
The current various patient populations and the continuously changing complex healthcare system need healthcare professionals to possess creative thinking and empathy competency. The DT is a methodology for building students' creative problem-solving and empathy (Beaird et al., 2018). “DT” is a human-centred design spirit and problem-solving method that considers a humanistic approach and also considers the feasibility of technology (Brown, 2008). Most DT creativities in medical education are at beginning, only a few programmes in medical education (Madson, 2021). DT methodology is general in many professional educations, and applying DT to health care could enhance innovation, capability, and effectiveness by increasing focus on the patient and provider needs (Altman et al., 2018). This human-centred thinking mode is consistent with the holistic care of “patient-centred” health care. The IDEO organization develops the DT process in five steps, namely Empathy, Define (demand definition), Idea (creative brain), Prototype (prototype), and Test (actual test) (Van De Grift & Kroeze, 2016). Stanford University initially established this problem-solving method for product design and has been massively applied to service innovation and science to deal with complex problems but has only limited medical education (Van De Grift & Kroeze, 2016). The creative thinking, empathy and cooperative ability is the crucial essential competency of healthcare professionals. The cultivation of these abilities must rely on learning each other between different professions. There are 95% of clinical leader, clinicians and executives from members of the NEJM Catalyst Insights Council express DT can be helpful, have a statistically significant benefit in coordination, enable to encourage the care team member to put themselves in the patient's shoes to experience the system from client's perspective in healthcare surrounding (Compton-Phillips & Seth Mohta, 2018). The procedure of prototype and test is an experiential, learner-centred process. Experiential learning emphasizes the experience plays a central role in the learning process, and learning results from synergetic resolution and synergetic transactions between person and environment (Kolb et al., 2014). The effectiveness of DT requires extensive theoretical and practical verification by researchers (Madson, 2021).
Nursing and psychology are essential resources to help patients solve sexual health problems in practice. At present, neither the Department of Nursing nor the Department of Psychology has conducted IPE with DT strategies for sexual health care. To improve the quality of care, develop a teaching model of IPE and DT, which can provide nursing and psychology students with a chance to learn and develop practical cooperation and empathy. The DT method is a useful tool for fostering innovation, teaching creative thinking and empathy through teamwork and communication tested in nursing education (Beaird et al., 2018).
1.2 Aims and hypothesis
This study aims to describe a DT approach in IPE programme of human sexuality course for senior nursing and psychology students and determine its effectiveness. The following research hypotheses are investigated:
Hypothesis 1.DT approach in IPE programme of human sexuality course will significantly improve the attitudes and behavioural intentions of nursing students and psychology students to provide clinical patients' sexual health care.
Hypothesis 2.DT approach in IPE programme of human sexuality course will significantly improve the observation experience, reflection ability, cross-domain cooperation, innovative design, and technology application performance of nursing students and psychology students.
2 METHODOLOGY
2.1 Study design and participants
We conducted a single-group interventional study design to measure the effect of DT approach in IPE programme of human sexuality course on students' attitude, behavioural intention toward providing sexual health care, and the core competence of IPE. The study was conducted at a medical university in Taiwan between September 2019 and January 2020. This study is the first time to apply DT approach in education in this medical university. The calculation of the number of participants needed to conduct research was performed using the G*Power 3.1.3 programme. The t-test for difference from constant (one sample case), was performed with significance level α = 0.05, power (1−β) = 0.80, number of measurements = 2, number of groups = 1, correlation among repeated measures = 0.40, and medium effect size f = 0.50. The total sample size required is 41 based on the criteria above.
The inclusion criteria of participants are senior students of nursing department and psychology department and do not have a course on human sexuality beforehand. Over 90 nursing students and 12 psychology students applied for this course. All of them met the criteria for study participants. Computer randomly sampling through the lottery method, thirty-six third-year nursing students and eight third-year psychology enrolled in the teaching programme. We divided 44 participants into four groups. Each group comprised 10 to 11 participants, and the composition of each group must include two departments. The proportion of members of the two departments in each group is relatively equal to minimize the negative effect of information from a single department. Both departments of nursing (nursing student: NS) and psychology (Psychology student: PS) are four-year programme. Both programmes have a modular structure, and each modular run independently. Therefore, most students continue to accumulate single-subject professional knowledge in the learning process, thus causing the fragment information from each module to be added to their knowledge base, lacking mutual links and integration. In this study, we collected students' information through self-reported questionnaires. Two students withdrew from the programme because of personal reasons, resulting in a final sample of 42 students who completed the questionnaire, which meets the criteria of sample size.
2.2 Development and implementation of the intervention
2.2.1 Teaching team development
This programme's initial phase began in July 2019 by developing a teaching team that includes two nursing teachers who major in sexual healthcare education and one psychology teacher who major in clinical psychology to be the tutor of the plan. All of them have completed the IPE teacher training course and already have IPE teacher qualifications. The teaching team develops an IPE programme through team members comprising group discussion and assessing educational needs in the previous study (Tsai et al., 2013) and following plan development process below.
2.2.2 Teaching programme development process
- Identification of the programme objectives:
- Develop the programme structure (Table 1):
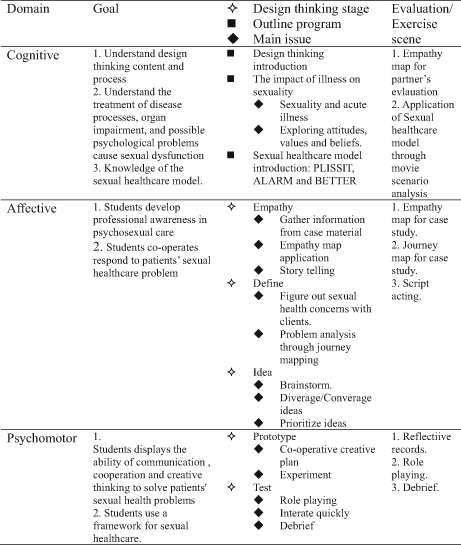
|
- Prototyping of scenario and learning material for the programme:
- Evaluation of the designed programme suited for the goal of IPE:
To confirm this teaching plan's applicability, we invited a nursing education expert and psychology counselling expert from two other teaching institutions for the consultant to review the teaching programme. There are 11 review items evaluated about programme objectives link the mission and belief statements to programme design, teaching and learning methods, and outcome. Each item is given a score, 1 – to be strengthened, 2 – to be acceptable, 3 – good, 4 – excellent, and finally give a comprehensive comment. Both scholars gave this teaching plan the highest score. They described that this teaching plan could arouse students' motivation and interest and align with IPE cooperation and innovative design, guiding students to reflect and increase empathy.
2.3 Measures
Building from a conceptual model theorizing the impact of IPE across the learning continuum, collecting qualitative and quantitative data can help identify the critical factors of collaboration (Cahn et al., 2016). The students completed a self-reported questionnaire survey at two points in time: at the beginning (pre), at the end of the programme (post), and a complete qualitative reflection log at the end of the programme.
2.3.1 Scale of IPE core competence
Students' learning performance evaluation adopts the IPE core competence measurements that have established reliability and validity to evaluate IPE learning effectiveness (Wang, 2017). The measurement contains five subscales corresponding with five core competence. Five-core competence is observation experience, reflection, interprofessional cooperation, innovative design and technology application, respectively. The numbers of questions and Cronbach's α in each domain are respectively: observation experience (21 items, Cronbach's α = 0.92), reflection (12 items, Cronbach's α = 0.92), interprofessional cooperation (13 items, Cronbach's α = 0.91), innovative design (20 items, Cronbach's α = 0.93) and technology application (17 items, Cronbach's α = 0.93) (Wang, 2017). The validity is confirmed by factor analysis. Each subscale's answer choices carry a point (1-never, 2-occasionally, 3-usually, 4-always) and are summed to obtain five domain scores. The higher scores signify better competence in each domain (Wang, 2017).
2.3.2 Attitude on sexual health care (NASH) and intention on sexual health care (NISH)
The NASH and NISH scales were developed based on the Permission/Limited Information/Specific Suggestions/Intensive Therapy model to evaluate attitude toward nursing intervention on sexual health care. Each item of NASH is answered using 5 points Likert-type scale (1 = strongly disagree to 5 = completely agree). The Cronbach's α was 0.85, four factors were extracted, explaining 60.63% of the variance, and all 15 items demonstrated moderate-to-strong loading (>0.50) (Huang et al., 2013). NISH items were answered using 7 points Likert-type scale (1 = definitely impossible to 7 = definitely possible). The overall Cronbach's alpha of the 19-item instrument was 0.96 and 72.42% of the cumulative variance explained by these three factors (Huang et al., 2012).
2.3.3 Reflection log
The students' reflection logs are a qualitative tool to understand students' detail personal experience in participating in the IPE project process. The students must respond to questions such as, what am I doing? What am I learning in the problem-solving process? How do these learning make me grow? How do I modify my perspective in this experience? Furthermore, through this reflection record, teacher could connect students to programme concept, understand the programme's pros and cons and improve plans.
2.4 Data collection
Students filled out three scales at the programme beginning (pre), at the end of the programme (post 1), and 3 months after the programme (post 2). They spent approximately 10–15 min completing the questionnaire. All participants were free to ask questions on the study or to request withdrawal from it. Students completed the questionnaire anonymously after their informed consent was returned. Similarly, to maintain confidentiality, students were instructed to return questionnaires in the envelopes provided. Results were presented only at the group level in order to ensure anonymity.
2.5 Data analysis
The data were analysed using the Statistical Package for the Social Sciences for Windows (Version 22.0; SPSS Inc.). Descriptive statistics, such as frequency, mean, and SD, were used to analyse the measurements' sociodemographic data and information. The paired t-test was used to evaluate the pre- and post-programme score variations at a significance level of .05. Because the question for the IPE core competence of five dimensions had different numbers of items, after the t-tests, we converted the students' raw scores to 100-unit scores to standardize the data by percentage to compare the differences in the growth rate of each dimension.
2.6 Ethical
This study was reviewed and approved by the Institutional Review Board of Chung Shan Medical University Hospital. The aims and procedures of the study were explained to each potential participant. A questionnaire packet that included a cover letter that described this programme's purpose and reputation, the right to turn down participation and a guarantee of anonymity was delivered to participants. After an explanation of the study, students signed informed consent forms to participate in this study. Once the study has begun, participants must be free to withdraw at any time without penalty. To guarantee anonymity, possible recognizing information, such as names or students' ID numbers, was eliminated from the records and was not displayed.
3 RESULTS
3.1 General characteristics of study participants
There are 35 students from the school of Nursing and seven from the school of Psychology, and researcher received consent from all of the selected students. The mean age is 20.52 ± 0.97 of the participants (Table 2).
| Characteristics | Mean | SD | N | % |
|---|---|---|---|---|
| Age | 20.52 | 0.97 | ||
| Gender | ||||
| Male | 9 | 21.4 | ||
| Female | 33 | 78.6 | ||
| Department | ||||
| Nursing | 35 | 83.3 | ||
| Psychology | 7 | 16.7 | ||
3.2 Outcome evaluation
3.2.1 Effect on students' attitude and intention for providing sexual health care
At the pre-stage, the mean of level scores and standard deviation of whole attitude and subscale of NASCH (Attitude, Permission, Limited Information, Specific Suggestion, and Intensive Therapy) were 3.20 ± 0.91, 3.61 ± 0.47, 4.17 ± 0.44, 3.49 ± 0.69, and 4.24 ± 0.45, respectively. At the post-stage, the mean of scores and standard deviation are 4.16 ± 0.37, 5.20 ± 0.42, 4.47 ± 0.40, 4.10 ± 0.52 and 5.56 ± 0.76, respectively (Table 3). The students' attitude dimension score in the post-test is higher than those in the pre-test and reach statistically significant differences both in total and subscale (p < .05).
| Attitude/intention | Mean ± SD | T (p) | |
|---|---|---|---|
| Pre (N = 42) | Post (N = 42) | ||
| Attitude | |||
| Total score | 48.07 ± 4.53 | 62.40 ± 5.54 | <.05 |
| Mean of level score | 3.20 ± 0.91 | 4.16 ± 0.37 | <.05 |
| Mean of each level scores | |||
| Permission | 3.61 ± 0.47 | 5.20 ± 0.42 | <.05 |
| Limited information | 4.17 ± 0.44 | 4.47 ± 0.40 | <.05 |
| Specific suggestion | 3.49 ± 0.69 | 4.10 ± 0.52 | <.05 |
| Intensive therapy | 4.24 ± 0.45 | 5.56 ± 0.76 | <.05 |
| Intention | |||
| Total score | 72.86 ± 10.04 | 87.67 ± 6.90 | <.05 |
| Mean of level scores | 3.83 ± 0.53 | 4.61 ± 0.36 | <.05 |
| Mean of each level scores | |||
| Permission | 5.11 ± 0.67 | 5.63 ± 0.56 | <.05 |
| Limited information | 3.61 ± 0.62 | 4.31 ± 0.52 | <.05 |
| Specific suggestion | 3.27 ± 0.51 | 4.14 ± 0.54 | <.05 |
At the pre-stage, the mean of scores and standard deviation of total score and subscale of NISH (Behavioural Intention, Permission, Limited Information, Specific Suggestion) were 3.83 ± 0.53, 5.11 ± 0.67, 3.61 ± 0.62, and 3.27 ± 0.51, respectively. At the post-stage, the mean of scores and the standard deviation is 4.61 ± 0.36, 5.63 ± 0.56, 4.31 ± 0.52, and 4.14 ± 0.54, respectively. The students' behavioural intention dimension score in the post-test is higher than those in the pre-test and reach statistically significant differences both in total and subscale (p < .05). Therefore, Hypothesis 1 was supported.
3.2.2 Effect on Interprofessional core competence
At the pre-stage, the mean of scores and standard deviation of Interprofessional core competence in Observation Experience, Reflective Feedback, Interprofessional Cooperation, Innovative Design and Applied Technology each dimension were 2.70 ± 0.40, 2.39 ± 0.43, 2.37 ± 0.35, 2.00 ± 0.44, and 2.37 ± 0.47. (Table 4) At the post-stage, the mean of scores and standard deviation are 3.01 ± 0.38, 3.16 ± 0.57, 3.40 ± 0.44, 2.54 ± 0.50 and 2.74 ± 0.54. All of the post-scores of five core competence are higher than pre-test, indicating a statistically significant difference between two tests regarding each of the scales (p < .05). Therefore, Hypothesis 2 was supported.
| Dimension | Mean ± SD | T (p) | |
|---|---|---|---|
| Pre (N = 42) | Post (N = 42) | ||
| Observation experience | 2.70 ± 0.40 | 3.01 ± 0.38 | <.05 |
| Reflective feedback | 2.39 ± 0.43 | 3.16 ± 0.57 | <.05 |
| Interprofessional cooperation | 2.37 ± 0.35 | 3.40 ± 0.44 | <.05 |
| Innovative design | 2.00 ± 0.44 | 2.54 ± 0.50 | <.05 |
| Applied technology | 2.37 ± 0.47 | 2.74 ± 0.54 | <.05 |
After standardization based on percentages, each dimension of IPE's growth score is presented in a radar chart (Figure 1). It can be seen from Figure 1 that the growth score is in Interprofessional Cooperation and Reflective Feedback.

3.2.3 Reflection log data
Almost all respondents have a positive response for the design-thinking framework for IPE in human sexuality course. Over the study's progress, we summarized the data from the students' reflection logs as follows.
Knowing different perspective from interdisciplinary cooperation and having great empathy
The students stated that they get a different perspective of sexuality from empathy map work, drama and the chance to approach sexual concerns. The students highlighted the value of cooperation with different discipline in the DT process, such as happy to know each other (PS 1, PS 3, NS 13), interdisciplinary cooperation is meaningful (NS 15, NS 27), as exemplified by the following information from some students:
… from the drama process, I can learn from a different perspective, and different things (ex, communication skill) … (NS 7)
… from the course, I understand that many people have different ideas about sexuality, and everyone has about ‘sexual’ concern or question…. (PS 1)
In the past, I did not clearly understand the counseling process. I thought that the counselor would directly answer the questions of the case. Through discussions with the psychology students, I realized that the counseling is to guide the case to come up with solutions, not to directly answer the case. (NS 17)
I can understand exposure to sexual behavior is a normal thing, there is no need to avoid the taboos, but you must know how to protect yourself already. (NS 11)
Discuss different opinions through the DT process to reach consensus and inspire greater creativity
I have the feeling of opening up another world, but the same education will have all kinds of different ideas. I also know that many physiologic conditions affect patients' psychology, and I learned to care for the case from different professional angles and understand more about ‘sex’. (PS 4)
In the process of solving the problem of a case, the empathy map can be used to understand the situation of the case and clarify the needs of the case, and develop new ideas… (NS 15)
Sexuality involves too many aspects. Discuss the empathy map together, discover the different thinking patterns of others, and stir up new ideas from brainstorming. (NS 22)
Be more confident to face interdisciplinary cooperation and complicated problems of patients
Through several group discussions, different disciplines can express different opinions, coordinate with each other, and come up with solutions together. This course made me more courageous to express my profession, understand and support the ideas of other professionals. (NS 4)
Understanding that the directions and perspectives of each professional field on the same issue are different. In this way, interprofessional education helps me know more that multi-directional thinking is critical to solving patients' complicated problems. (PS 5)
Through discussion and commentary, I feel that it can be applied to many problems in the future. Many things are not a single perspective. On the contrary, there are more points to be considered, and many rewards are obtained. (NS 8)
4 DISCUSSION
4.1 Effectiveness of the programme on attitude and behaviour intention of SHC
This study is the first trial using a DT strategy in sexual healthcare education programme. The average mean of the level score of post-test from this study is higher compared with baseline and the previous study (Huang et al., 2013). This study indicated that an IPE combined with a DT approach teaching programme could significantly improve both nursing and psychology students' attitude and behaviour intention of Sexual health care (SHC). However, behavioural intentions are an essential indicator of predictive execution (Ajzen, 2011). These results were similar to other educational programmes conducted with clinical nurses (Sung et al., 2016), nurse and physicians (Jonsdottir et al., 2016), and medical students (Faulder et al., 2004; Gianotten et al., 2006). The dimensions involved in sexual health care are quite complex. Through the divergence and convergence cycles of Empathy, Define (demand definition), Idea (creative brain), Prototype (Prototype) and Test (actual test) of DT, students observe and understand the situation of the case holistically, practice communication skills, and empathize with patients, and finally focus on solving individual problems. These “Learning by Doing” steps fully provide practice opportunities. The growth of student attitudes and behavioural intentions echoes the “Experiential Learning Theory” proposed by scholar Kolb (Kolb et al., 2014). Through the prototype and actual test, students practice learning experience, hands-on learning and conflict resolution to think deeply about the complex process of learning. In other words, the DT process encompasses the “learning by doing” experimental teaching model, which explores the science of care through experiential learning methods. The perception of practical doing experience is more potent than text and language conveyed by traditional teaching models. DT can accumulate students' ability to respond appropriately to new situations.
4.2 Effectiveness of the programme on IPE core competence
The average mean of level scores of the post was significantly higher than the baseline in IPE core competence, especially in dimensions of interprofessional cooperation and reflective feedback. This result is consistent with previous studies. The essential intermediate step in linking IPE with health outcomes is enhanced collaborative behaviour and performance in practice (Cox et al., 2016). Compared with the examples of 21 students in a previous ageing technology workshop conducted in Taiwan (Wang, 2017), the growth slope of an average mean of level score from this study was higher in Observation Experience, Reflective Feedback, Interprofessional Cooperation and less in Innovative Design and Applied Technology. This result indicates that this programme provides an actual opportunity for interprofessional cooperation and reflective feedback practice. The reason for the various growth slope in different dimensions belongs to different problem attributes. The focus of IPE structured with the DT framework-teaching programme is to cultivate the students' competence of cooperation and provision of sexual health care, which different from innovating new technology tools in the ageing technology workshop. The different attributes of the problem cause differences in the learning and growth of students in different aspects.
4.3 The reflection of IPE structured with DT framework
For this study, we attach great importance to students' reflective records. Almost all students gave a positive evaluation, believing that they have made progress both personally and professionally, having experienced such a course. Personal progress includes communication skills, empathy and respect for others, and confidence in conflict resolution. Professional growth includes understanding the connotation and role functions of different majors and being more confident in their professional roles. Healthcare organizations are often structured as network organizations to provide patient-centred care within interdisciplinary networks. However, medical education has only limitedly institutionalized the teaching of skills and knowledge on critical thinking, creative problem-solving, collaborative working and effective communication (Van De Grift & Kroeze, 2016). Students' positive evaluation of self and professional growth demonstrates their successful ability to transform learning into future problem-solving, which echoes DT as a methodology for building students' skills in creative problem-solving and empathy (Beaird et al., 2018). Although the programme provides empirical evidence about the effect of IPE and DT to improve the competence of providing sexual health care, the explanation effect of this study needs to be more rigorous because DT and IPE simultaneously applied.
5 CONCLUSION
Interprofessional education combined with a DT approach teaching programme could significantly improve both nursing and psychology students' attitude and behaviour intention of SHC. Through the prototype and actual test, students practice learning experience, hands-on learning and conflict resolution to think deeply about the complex process of learning. The IPE core competence, especially in dimensions of interprofessional cooperation and reflective feedback, was significantly improved. Almost all students gave a positive evaluation for IPE combined with a DT approach teaching programme, believing that they have made progress both personally and professionally, having experienced such a course.
6 LIMITATION
This study has some limitations, including that lack of a control group and the sample is small because of limitation by the appropriate number of team members and the ratio of instructors at one single university, which limits the generalizability of the study findings. Moreover, due to the limitation of school size, we only have one class of human sexuality course. Therefore, it is challenging to organize a human sexuality course with nursing and psychology students from a similar background of participants at the same time. Second, the proportion of group members, the proportion of psychology students is less than the nursing department. Although the number of nursing students from the original mother group is about three times that of psychology students, the proportion of research participants is 4.8 times. Although the research results have achieved good results in interprofessional cooperation, if the proportion of participants can be closer to reality, it will help the inference of the research results. Besides, we did not collect information about personal personality traits and sexual health history, which may distort the questionnaire's responses.
AUTHOR CONTRIBUTIONS
- substantial contributions to conception and design, acquisition of data or analysis and interpretation of data;
- drafting the article or revising it critically for important intellectual content.
ACKNOWLEDGEMENTS
We want to thank two educational experts for the evaluation teaching plan, nursing students and psychology students for their participation.
FUNDING INFORMATION
This research study was sponsored by the Ministry of Education Teaching Practice Research Program (PMN1080171).
CONFLICT OF INTEREST
No conflict of interest has been declared by the authors.
ETHICAL STATEMENT
This study was reviewed and approved by the Institutional Review Board of Chung Shan Medical University Hospital (CSMU No: CS2-19067).
Open Research
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to the privacy of research participants.